Approach to patient with HTN
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
"hypertension" AND "management"
Loading Image
Reading File
I now have excellent, comprehensive data from multiple authoritative sources. Let me compile the full answer.
Approach to the Patient with Hypertension
1. Background and Significance
Hypertension remains the leading cause of cardiovascular mortality and morbidity - stroke, heart disease, kidney disease, and peripheral vascular disease. The BP-CV risk relationship is linear and continuous: for adults aged 40-69 years, every 20 mmHg rise in SBP or 10 mmHg in DBP doubles mortality risk from stroke, ischemic heart disease, and vascular causes across a range of 115/75 to 185/115 mmHg. Lifetime risk of developing HTN is approximately 90%.
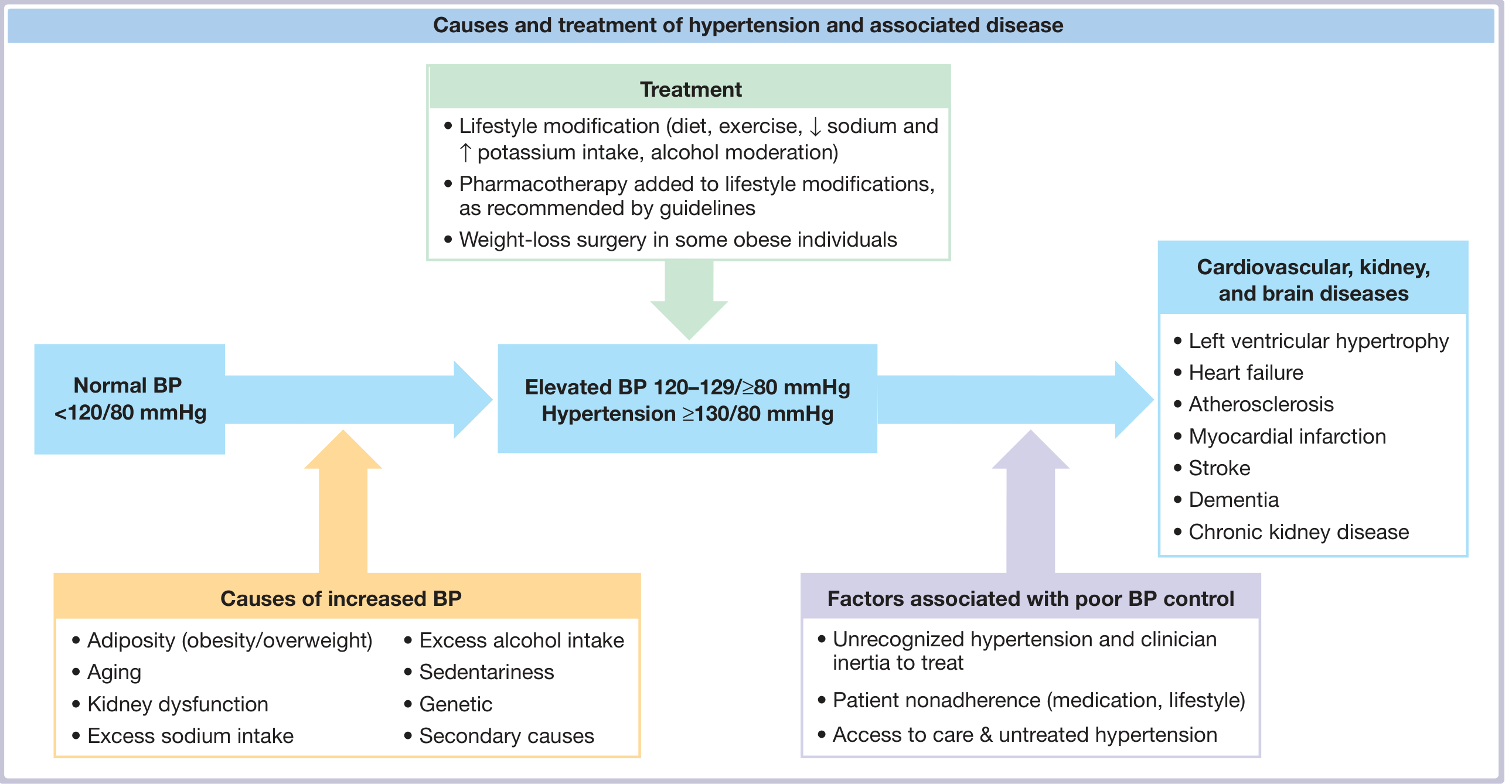
2. Classification of Blood Pressure (ACC/AHA 2017/2025)
| Category | SBP (mmHg) | DBP (mmHg) | |
|---|---|---|---|
| Normal | < 120 | and | < 80 |
| Elevated | 120-129 | and | < 80 |
| Stage 1 HTN | 130-139 | or | 80-89 |
| Stage 2 HTN | ≥ 140 | or | ≥ 90 |
Note: A new 2025 AHA/ACC guideline has been published (PMID: 40811516, Hypertension Oct 2025) - thresholds may be updated. The 2024 ESC guidelines (PMID: 39210715) define HTN at ≥ 140/90 mmHg, with a lower intervention threshold in high-risk patients.
3. Three Key Questions at Every Evaluation
The structured approach addresses three core questions:
- Is this primary (essential) or secondary hypertension?
- What are the additional CV risk factors?
- Is there end-organ damage present?
4. Accurate Blood Pressure Measurement
Errors in BP measurement are common. Key steps:
- Patient seated quietly for ≥5 minutes, back supported, legs uncrossed, no talking
- Use a validated upper-arm cuff of appropriate size (bladder encircles ≥80% of arm)
- Take ≥2 readings per visit, ≥2 separate occasions for initial diagnosis
- Measure both arms at first visit; use the arm with the higher reading subsequently
- Consider out-of-office BP (home or ambulatory) to confirm diagnosis and avoid white-coat effect
Pseudohypertension: In elderly patients with calcified, stiff brachial arteries, the cuff pressure needed to occlude the vessel may exceed true intraluminal pressure. Osler's maneuver (palpating the radial pulse while the cuff is inflated above systolic) helps identify this.
5. History and Physical Examination
History should cover:
- Duration and prior readings
- Symptoms: headache, flushing, palpitations, sweating (pheochromocytoma clues), snoring/apnea, muscle weakness (hyperaldosteronism)
- Medications: NSAIDs, OCPs, decongestants, stimulants, steroids, calcineurin inhibitors
- Lifestyle: sodium intake, alcohol, physical activity, diet
- Family history of premature CVD, CKD, HTN
- Personal history of diabetes, dyslipidemia, CKD, sleep apnea
Physical examination:
- BP both arms (and legs if coarctation suspected)
- BMI and waist circumference
- Fundoscopy: AV nicking, flame hemorrhages, papilledema (hypertensive retinopathy grades I-IV)
- Cardiovascular: S4 gallop, signs of heart failure, carotid/renal/femoral bruits
- Abdomen: renal masses, abdominal bruits
- Neurologic: signs of prior stroke
6. Initial Laboratory Work-up
| Test | Rationale |
|---|---|
| Fasting glucose | Screen for diabetes; baseline |
| Lipid profile (fasting) | ASCVD risk calculation |
| Serum Na, K, Cr + eGFR | Electrolyte disorders, CKD, baseline before drugs |
| Serum calcium | Hyperparathyroidism |
| TSH | Thyroid disease as secondary cause |
| CBC | Polycythemia (sleep apnea), anemia |
| Urinalysis (with microscopy) | Proteinuria, hematuria - glomerulonephritis, CKD |
| Urine albumin:creatinine ratio | Target organ damage marker |
| 12-lead ECG | LVH (Sokolow-Lyon criteria), arrhythmia |
| Echocardiogram (selective) | Sensitive for LVH and LV function; complements ECG |
7. Cardiovascular Risk Assessment
CVD risk drives treatment decisions, especially for Stage 1 HTN. Use the ACC/AHA Pooled Cohort Equations (PCE) for US adults aged 40-79 without prior CVD. Inputs include age, sex, race, SBP, cholesterol, diabetes, smoking, and current treatment. Those with 10-year ASCVD risk ≥10% are considered high risk.
High-risk without calculation needed: established CVD, CKD, diabetes mellitus, age ≥65 years.
Cardiovascular risk factors in HTN:
| Modifiable | Fixed / Less Modifiable |
|---|---|
| Smoking, DM, dyslipidemia, obesity, inactivity, unhealthy diet | Age, male sex, family history, CKD, obstructive sleep apnea, psychosocial stress, LVH, albuminuria ≥30 mg/g |
8. Screening for Secondary Hypertension
Screen at initial evaluation and again in resistant HTN (BP >140/90 on 3 maximally dosed drugs including a diuretic).
| Clue from Workup | Suspected Cause |
|---|---|
| Low K, high HCO3 | Primary aldosteronism (Conn), hypercortisolism |
| High K | Gordon syndrome, CKD |
| Elevated Cr, low eGFR | CKD, renal artery stenosis |
| Hematuria/proteinuria | Glomerulonephritis, interstitial nephritis |
| High Ca | Primary hyperparathyroidism |
| High Hct | Polycythemia, obstructive sleep apnea |
Common causes of secondary HTN and directed tests:
- Primary aldosteronism (~20% of resistant HTN): plasma aldosterone/renin ratio (ARR)
- Renovascular HTN / Renal artery stenosis (~25% of resistant HTN): renal Doppler US, CT angiography
- Obstructive sleep apnea (>50% of resistant HTN): sleep study (polysomnography)
- Pheochromocytoma/Paraganglioma: 24-hr urine catecholamines/metanephrines, plasma metanephrines
- Cushing's syndrome: 24-hr urine free cortisol, overnight dexamethasone suppression test
- Thyroid disease: TSH
- Coarctation of aorta: BP differential arms vs. legs, imaging
9. End-Organ Damage Assessment
| Organ | Manifestation |
|---|---|
| Heart | LVH, diastolic dysfunction, HFpEF, IHD, AF |
| Brain | Stroke (ischemic/hemorrhagic), hypertensive encephalopathy, dementia, white matter lesions |
| Kidney | Proteinuria, declining eGFR, hypertensive nephrosclerosis |
| Eye | Hypertensive retinopathy (grade I-IV) |
| Vasculature | Aortic aneurysm, peripheral artery disease |
10. Treatment
Lifestyle Modifications (All stages; foundation of treatment)
| Intervention | Expected SBP Reduction |
|---|---|
| DASH diet | 8-14 mmHg |
| Sodium restriction (<2.3 g/day) | 2-8 mmHg |
| Weight reduction (per 10 kg lost) | 5-10 mmHg |
| Aerobic exercise (30 min, 5 days/week) | 4-9 mmHg |
| Limit alcohol (≤1 drink/day women, ≤2 men) | 2-4 mmHg |
When to Start Pharmacotherapy
| Situation | Threshold to Treat |
|---|---|
| Stage 1 HTN + high ASCVD risk (≥10%) or CVD | ≥130/80 |
| Stage 1 HTN + low ASCVD risk | ≥130/80 (lifestyle first, re-evaluate at 3-6 months) |
| Stage 2 HTN | ≥140/90 - start immediately |
| Diabetes / CKD / established CVD | ≥130/80 |
First-Line Antihypertensive Classes
Four classes are first-line (Grade I, Level A):
- Thiazide/thiazide-like diuretics (chlorthalidone, hydrochlorothiazide, indapamide)
- Calcium channel blockers - CCBs (amlodipine, nifedipine - dihydropyridines preferred)
- ACE inhibitors (ramipril, lisinopril, enalapril)
- Angiotensin receptor blockers - ARBs (losartan, telmisartan, valsartan)
ACE inhibitors and ARBs should not be combined (dual RAS blockade increases risk of hyperkalemia and AKI without added benefit).
Monotherapy vs. Combination
- Stage 1 HTN: initiate single agent; titrate and add sequentially to achieve target
- Stage 2 HTN (BP >20/10 above target): start with two-drug combination (Grade I, Level C) - more effective than doubling a single drug, blocks counter-regulatory mechanisms
Why combination is superior: Single-drug BP lowering triggers counter-regulatory responses (e.g., diuretic or CCB activates RAAS). A two-drug combination blocks multiple mechanisms simultaneously, producing greater BP reduction with less dose-related side effects.
Compelling Indications and Preferred Agents
| Comorbidity | Preferred Agent(s) |
|---|---|
| Heart failure with reduced EF | ACEi/ARB + beta-blocker + diuretic + MRA |
| Post-MI | ACEi + beta-blocker |
| CKD with proteinuria | ACEi or ARB (first-line) |
| Diabetes | ACEi or ARB (if proteinuria/CKD present) |
| Isolated systolic HTN (elderly) | Thiazide or CCB |
| Pregnancy | Labetalol, nifedipine, methyldopa |
| Angina | Beta-blocker or CCB |
| Benign prostatic hyperplasia | Alpha-blocker (add-on) |
BP Targets
- General population: < 130/80 mmHg (ACC/AHA 2017/2025)
- High CV risk (SPRINT trial): < 120 mmHg SBP reduced CV events further
- Age ≥65 (non-frail): < 130/80 acceptable; caution in frail elderly - avoid excessive lowering (risk of falls, hypoperfusion)
- CKD with proteinuria: < 130/80
- Pregnancy: 120-160/80-110 (avoid hypotension)
11. Special Populations
| Population | Key Consideration |
|---|---|
| Elderly (≥65) | Start low, go slow; prefer thiazide or CCB; watch for orthostatic hypotension |
| Diabetes | ACEi/ARB preferred if proteinuria; target < 130/80 |
| CKD | ACEi/ARB slow progression; watch K and Cr after initiation |
| Pregnancy | Avoid ACEi/ARB/direct renin inhibitors (teratogenic); use labetalol, nifedipine, methyldopa |
| Black patients | CCB + thiazide more effective; ACEi/ARB less effective as monotherapy but still indicated with DM/CKD |
| Resistant HTN | Ensure adherence, correct technique; add spironolactone as 4th agent; investigate secondary causes |
12. Follow-Up and Monitoring
- Monthly visits until BP at target
- Once stable: every 3-6 months
- Monitor electrolytes and creatinine 2-4 weeks after starting ACEi/ARB or diuretic
- Reinforce lifestyle modifications at every visit
- Encourage home BP monitoring (HBPM) - improves adherence and control
13. Resistant Hypertension
Defined as BP above target despite 3 drugs (including a diuretic) at maximal/maximally tolerated doses. Management:
- Verify true resistance: confirm adherence, check technique, rule out white-coat effect with ambulatory monitoring
- Screen for all secondary causes
- Add spironolactone (50-100 mg/day) as 4th agent - evidence from PATHWAY-2 trial
- Consider referral to hypertension specialist
Sources:
- NKF Primer on Kidney Diseases, 8e - Chapters 64-65
- Fuster and Hurst's The Heart, 15th Ed. - Chapter 5
- Comprehensive Clinical Nephrology, 7th Ed. - Chapter 37
- 2025 AHA/ACC Guideline for Prevention, Detection, Evaluation and Management of High Blood Pressure (PMID: 40811516), Hypertension Oct 2025
- 2024 ESC Guidelines for Management of Elevated Blood Pressure and Hypertension (PMID: 39210715), Eur Heart J Oct 2024
Guideline update alert: A new 2025 AHA/ACC guideline has been published and may revise BP thresholds, treatment targets, and drug recommendations beyond what is covered in the textbooks above. Review PMID 40811516 for the most current recommendations.
This is a shared conversation. Sign in to Orris to start your own chat.