explain me 10 common heart disease with ECG changes and ECG image of those disease
Reading File
Finding Sources
Finding Sources
Searching the Web
ECG changes 10 common heart diseases STEMI atrial fibrillation heart block images
Finding Sources
Finding Sources
Finding Sources
Searching the Web
ECG images STEMI NSTEMI atrial fibrillation heart block ventricular tachycardia Wolff-Parkinson-White site:litfl.com OR site:ecgwaves.com
Reading File
Reading File
Reading Web Page
https://litfl.com/ecg-library/
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Finding Sources
I have rich ECG images from authoritative textbooks. I now have enough material to write a comprehensive answer. Let me compile everything into a detailed, well-organized response covering 10 common heart diseases with ECG changes and images from the medical library.
10 Common Heart Diseases: ECG Changes and Images
1. ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery causing transmural ischemia.
ECG Changes:
- ST-segment elevation ≥1 mm in ≥2 contiguous limb leads or ≥2 mm in ≥2 contiguous precordial leads (V1-V6)
- Hyperacute T-waves (early sign - tall, peaked)
- Pathological Q-waves (>40 ms wide, >25% of R-wave height) - indicate completed infarction
- ST depression in reciprocal leads
- T-wave inversions (late finding)
Localisation by leads:
- Anterior STEMI: ST elevation in V1-V4 (LAD occlusion)
- Inferior STEMI: ST elevation in II, III, aVF (RCA occlusion)
- Lateral STEMI: ST elevation in I, aVL, V5-V6 (LCx occlusion)
ECG - Inferior-Lateral MI (Left Circumflex Occlusion):
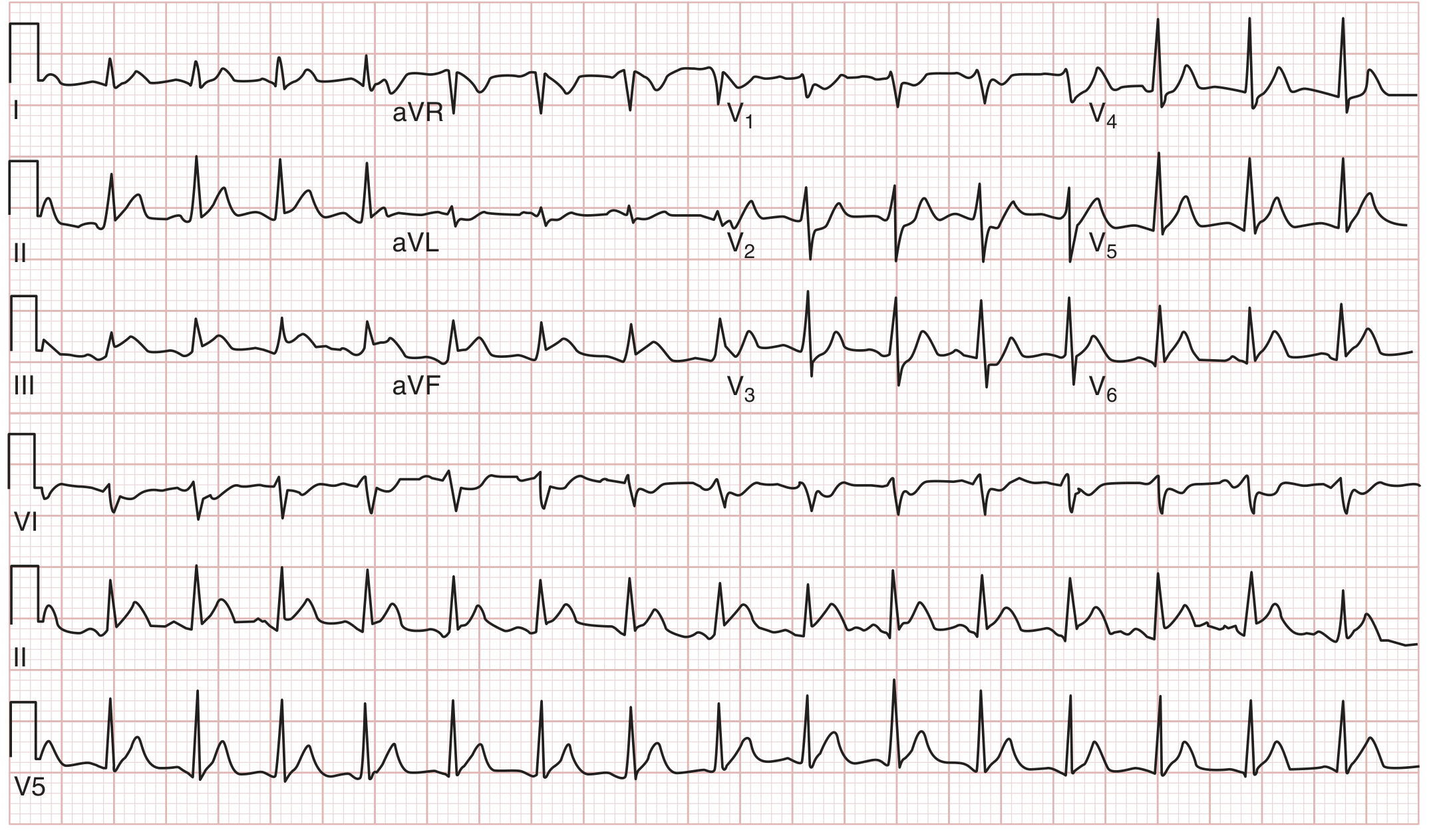
ST-segment elevation in leads II, III, aVF (inferior), and V5-V6 (lateral), with reciprocal ST depression in V1-V3. This patient had 100% occlusion of the left circumflex coronary artery. - Rosen's Emergency Medicine
2. NSTEMI / Unstable Angina (Non-ST Elevation ACS)
Pathophysiology: Partial or intermittent coronary occlusion causing subendocardial ischemia.
ECG Changes:
- ST-segment depression (horizontal or downsloping, ≥0.5 mm in ≥2 contiguous leads)
- T-wave inversions (≥1 mm), particularly in precordial leads
- No ST elevation
- No pathological Q-waves
- ECG may be entirely normal in up to 6% of NSTEMIs
- Dynamic ECG changes (serial ECGs may show evolution)
Key point: Diagnosis requires elevated troponin in the absence of ST elevation. Serial ECG monitoring is vital, as changes diagnostic of STEMI may evolve. - Tintinalli's Emergency Medicine
ECG - aVR elevation suggesting left main/proximal LAD occlusion (NSTEMI pattern):
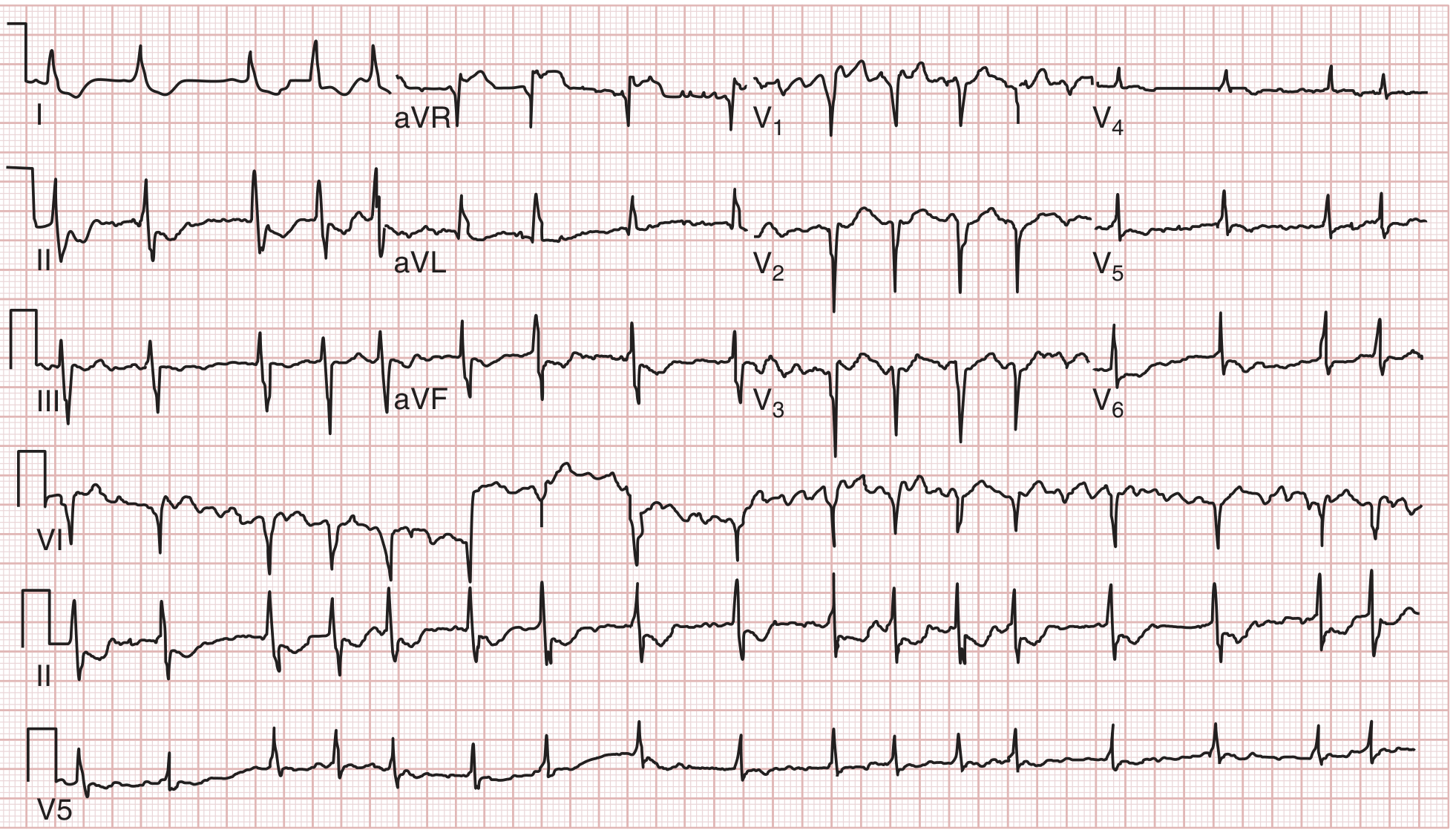
ST elevation in aVR greater than V1, suggesting left main or proximal LAD occlusion - a high-risk NSTEMI/ACS pattern with diffuse ST depression and aVR elevation. - Tintinalli's Emergency Medicine
3. Atrial Fibrillation (AF)
Pathophysiology: Chaotic, disorganized electrical activity from multiple re-entrant circuits throughout the atria. Rate typically 125-150 bpm when untreated.
ECG Changes:
- Absent P-waves - replaced by fibrillatory (f) waves (irregular, low-amplitude baseline oscillations >300/min)
- Irregularly irregular RR intervals (hallmark sign)
- Normal QRS morphology (unless aberrant conduction)
- Ventricular rate variable, typically 100-160 bpm if untreated
- No organized atrial activity visible
"The irregular pattern... is one of the clinical findings used to diagnose the condition. Therefore, atrial fibrillation is often described as an irregularly, irregular rhythm." - Guyton and Hall Medical Physiology
ECG - Atrial Fibrillation (Lead II):

Lead II showing irregularly irregular QRS complexes with no discernible P-waves. The fibrillatory baseline replaces organized atrial activity. - Guyton and Hall Medical Physiology
4. Atrioventricular (AV) Heart Block
Pathophysiology: Impaired conduction through the AV node or His-Purkinje system.
ECG Changes by Degree:
| Degree | ECG Finding |
|---|---|
| 1st degree | PR interval >200 ms (>5 small squares), all P-waves conduct |
| 2nd degree Mobitz I (Wenckebach) | Progressive PR prolongation until a P-wave is not followed by QRS ("dropped beat"), then cycle repeats |
| 2nd degree Mobitz II | Fixed PR interval with sudden failure of conduction (dropped QRS without warning) |
| 3rd degree (Complete) | Complete AV dissociation - P-waves and QRS complexes are completely independent; atrial rate > ventricular rate |
"Complete heart block (third-degree block) involves complete AV dissociation with a ventricular rate that is slower than the atrial rate." - Harrison's Principles of Internal Medicine 22E
ECG - All Degrees of AV Block (A to E):

(A) First-degree AVB: PR >200 ms, no dropped beats. (B) Mobitz I (Wenckebach): group beating with progressive PR prolongation before dropped beat. (C) Mobitz II: abrupt dropped QRS without prior PR prolongation. (D) 2:1 AVB: alternating conducted/non-conducted P-waves. (E) Complete heart block: completely independent atrial and ventricular rhythms (junctional escape). - Washington Manual of Medical Therapeutics
5. Ventricular Fibrillation (VF)
Pathophysiology: Completely disorganized ventricular electrical activity with no effective contraction - a cardiac arrest rhythm. Most commonly seen with severe ischemic heart disease.
ECG Changes:
- No recognizable P-waves, QRS complexes, or T-waves
- Chaotic, irregular, continuously varying waveforms
- Amplitude can be coarse (easier to defibrillate) or fine (harder to defibrillate)
- No organized rhythm whatsoever
- Incompatible with cardiac output - causes immediate cardiac arrest
ECG - Three Forms of Ventricular Fibrillation:
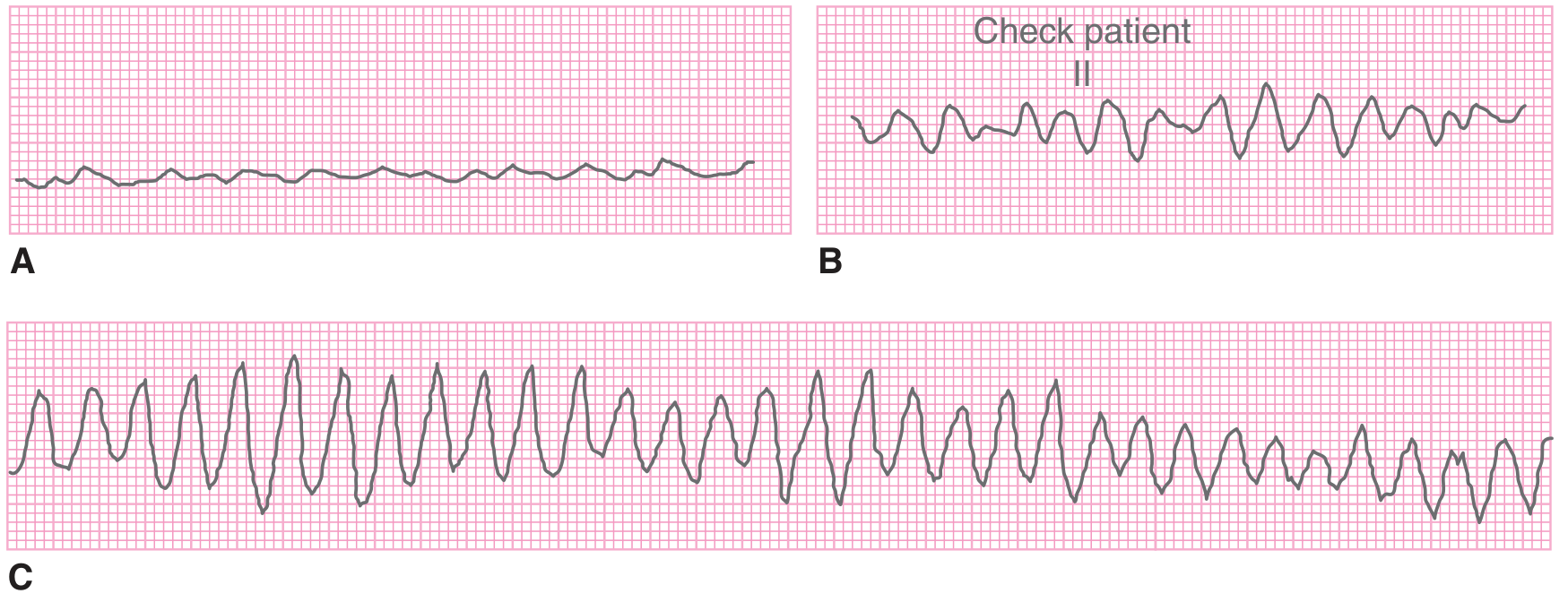
(A) Fine amplitude VF - almost flat, difficult to distinguish from asystole. (B) Coarse amplitude VF - larger chaotic waves. (C) Coarse VF that can mimic ventricular tachycardia. Treatment: immediate defibrillation + CPR. - Tintinalli's Emergency Medicine
6. Wolff-Parkinson-White (WPW) Syndrome
Pathophysiology: An accessory conduction pathway (Bundle of Kent) bypasses the AV node, creating ventricular pre-excitation. This sets up re-entrant tachyarrhythmias.
ECG Changes (in sinus rhythm):
- Short PR interval (<120 ms) - impulse bypasses the AV node delay
- Delta wave - slurred initial upstroke of QRS (pre-excitation of the ventricle via the accessory pathway)
- Wide QRS complex (>120 ms) due to the delta wave
- Secondary ST-T changes (discordant to QRS)
- During tachycardia: narrow QRS (orthodromic AVRT) or wide QRS (antidromic AVRT, which mimics VT)
"WPW syndrome is a form of ventricular preexcitation involving an accessory conduction pathway that bypasses the AV node and creates a direct electrical connection between the atria and ventricles." - Tintinalli's Emergency Medicine
ECG - WPW Syndrome (12-lead with delta wave):
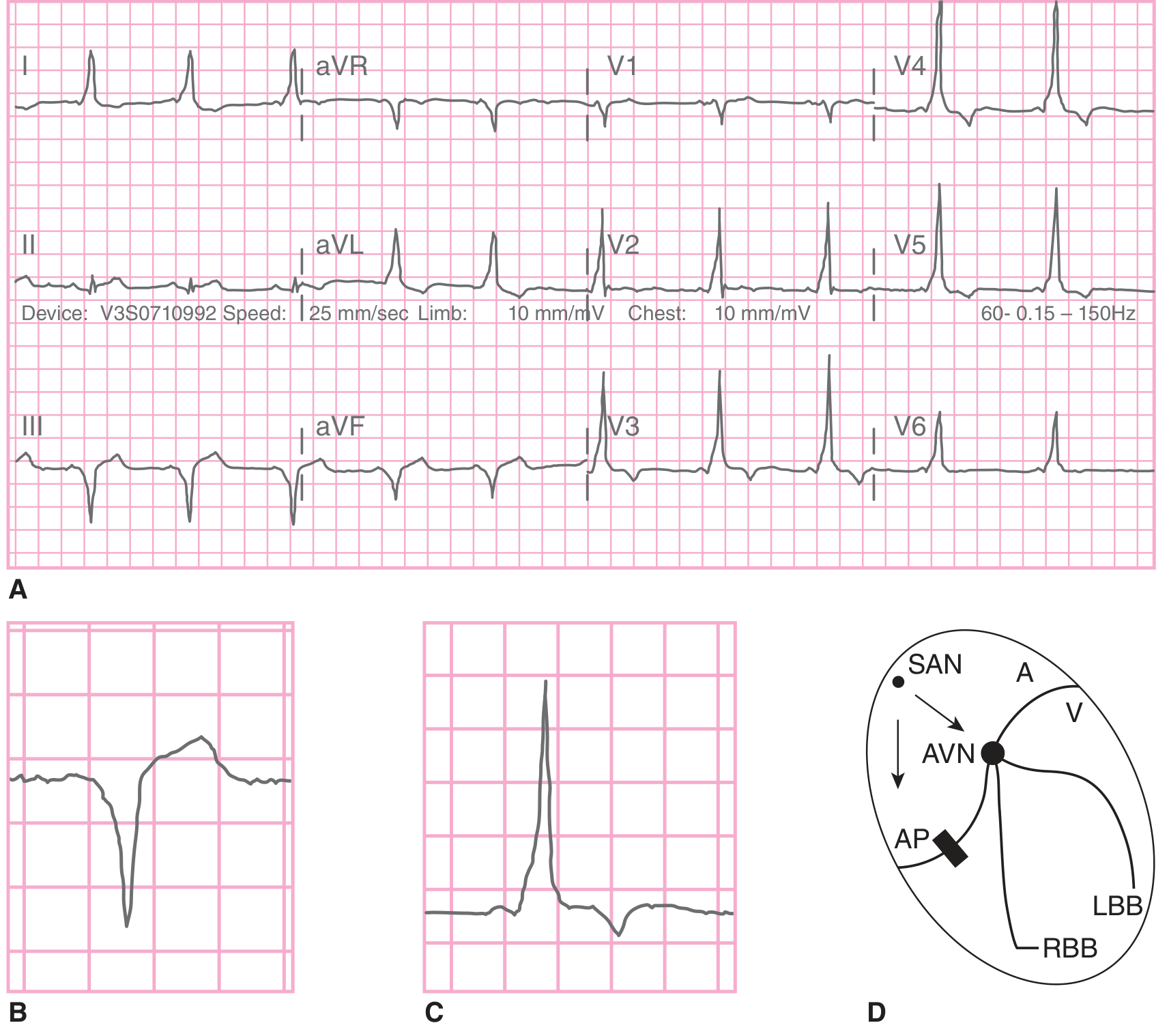
(A) 12-lead ECG showing classic WPW pattern: short PR interval, delta waves (slurred QRS upstroke), wide QRS complexes, and secondary ST-T changes. (B) Enlarged delta wave morphology. (C) Normal QRS for comparison. (D) Diagram showing the accessory pathway (AP) bypassing the AV node (AVN). - Tintinalli's Emergency Medicine
7. Ventricular Tachycardia (VT)
Pathophysiology: Three or more consecutive ventricular beats at ≥100 bpm, originating below the bundle of His. Most common in patients with ischemic heart disease or cardiomyopathy.
ECG Changes:
- Wide QRS complex (>120 ms) tachycardia at 100-250 bpm
- AV dissociation - P-waves march through independently, unrelated to QRS (pathognomonic when present)
- Fusion beats - hybrid QRS from simultaneous sinus and ventricular activation (pathognomonic)
- Capture beats - rare normal-looking QRS in midst of VT (sinus impulse captures the ventricle)
- Concordance of QRS in all precordial leads (all positive or all negative)
- QRS axis typically abnormal (left axis, or extreme right axis)
- No response to adenosine (distinguishes from SVT with aberrancy)
"For wide-QRS complex tachycardias, the 12-lead ECG is useful in distinguishing a supraventricular tachycardia (with aberrancy) from a ventricular tachycardia. The presence of fusion beats or AV dissociation during a wide-QRS complex tachycardia strongly suggests VT." - Goldman-Cecil Medicine
8. Atrial Flutter
Pathophysiology: A macro-reentrant circuit in the right atrium (typically around the tricuspid annulus) firing at ~300 bpm. The AV node blocks most impulses, typically with 2:1 conduction (ventricular rate ~150 bpm).
ECG Changes:
- "Sawtooth" flutter (F) waves at 250-350/min, best seen in leads II, III, aVF, and V1
- No isoelectric baseline between atrial waves
- Regular or regularly irregular ventricular response
- QRS morphology is normal (unless aberrant conduction)
- Classic 2:1 block = flutter rate 300/min → ventricular rate 150 bpm
- Can have 3:1 or 4:1 block (ventricular rates of 100 or 75 bpm)
Key clinical point: A regular tachycardia at exactly 150 bpm should always raise suspicion for atrial flutter with 2:1 block.
9. Left Ventricular Hypertrophy (LVH)
Pathophysiology: Increased left ventricular muscle mass from chronic pressure overload (hypertension, aortic stenosis) or volume overload. The enlarged LV generates larger electrical signals.
ECG Changes:
- Sokolow-Lyon criteria: S in V1 + R in V5 or V6 > 35 mm
- Cornell criteria: R in aVL + S in V3 > 28 mm (men) or >20 mm (women)
- Tall R-waves in lateral leads (I, aVL, V5-V6) with deep S-waves in right precordial leads (V1-V2)
- "LV strain" pattern: ST depression and T-wave inversion in leads with tall R-waves (I, aVL, V5-V6) - indicates pressure overload
- Left axis deviation
- Widened QRS (can be up to 110 ms)
- Large, broad P-waves or notched P-waves (P mitrale) - if left atrial enlargement co-exists
10. Pericarditis (Acute)
Pathophysiology: Inflammation of the pericardium, causing irritation of the adjacent epicardium, which produces diffuse ST-T wave changes. Unlike MI, the inflammation is diffuse rather than territorial.
ECG Changes (4 classic stages):
| Stage | ECG Finding | Timing |
|---|---|---|
| Stage 1 | Diffuse concave ("saddle-shaped") ST elevation in almost all leads except aVR and V1; PR depression (most specific sign) in II, V5-V6; PR elevation in aVR | Hours to days |
| Stage 2 | ST normalizes, T-waves flatten | Days |
| Stage 3 | Diffuse T-wave inversions | Days to weeks |
| Stage 4 | ECG returns to normal | Weeks |
Key distinctions from STEMI:
- ST elevation is concave (upward dome shape) in pericarditis vs convex (tombstone) in STEMI
- ST elevation is diffuse (all leads) in pericarditis vs regional (territorially localized) in STEMI
- PR depression is characteristic of pericarditis
- No reciprocal ST depression (except aVR) in pericarditis
- No Q-waves in pericarditis
"In pericarditis, the ST segments are concave, with an initial upslope contour... PR segment depression is an insensitive yet specific associated electrocardiographic finding in pericarditis." - Rosen's Emergency Medicine
Quick Reference Summary Table
| # | Condition | Key ECG Finding | Rate | Rhythm |
|---|---|---|---|---|
| 1 | STEMI | Regional ST elevation, Q-waves | Variable | Regular |
| 2 | NSTEMI | ST depression, T inversion, or normal | Variable | Regular |
| 3 | Atrial Fibrillation | No P-waves, irregularly irregular | 100-160 | Irregular |
| 4 | AV Block | Long PR / dropped beats / AV dissociation | Slow | Variable |
| 5 | Ventricular Fibrillation | Chaotic, no QRS/P/T waves | >300 | Chaotic |
| 6 | WPW Syndrome | Delta wave, short PR, wide QRS | Variable | Variable |
| 7 | Ventricular Tachycardia | Wide QRS, AV dissociation | 100-250 | Regular |
| 8 | Atrial Flutter | Sawtooth F-waves, 2:1 block | ~150 | Regular |
| 9 | LVH | High voltage (S-V1 + R-V5 >35 mm), strain | Normal | Regular |
| 10 | Pericarditis | Diffuse concave ST↑, PR depression | Normal | Regular |
Sources: Guyton and Hall Medical Physiology | Harrison's Principles of Internal Medicine 22E | Tintinalli's Emergency Medicine | Rosen's Emergency Medicine | Washington Manual of Medical Therapeutics | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.