Patient has acute urticaria what are the treatment
Reading File
Finding Sources
Searching PubMed
"acute urticaria" AND treatment
Reading File
Finding Sources
Reading Article
PMID: 38280453
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Here is the full treatment guide for acute urticaria:
Treatment of Acute Urticaria
1. First Step: Identify and Remove the Trigger
The most important initial step is identifying and avoiding the inciting agent. All potential causes - including prescription drugs, OTC medications, supplements, NSAIDs, opiates, alcohol, and foods - should be eliminated or substituted. Most cases of acute urticaria are self-limited and resolve spontaneously.
2. Stepwise Pharmacological Treatment by Severity
A. Mild to Moderate Acute Urticaria
First-line: H1 Antihistamines (preferred)
-
Second-generation (non-sedating) - preferred due to lower risk of psychomotor impairment and sedation:
- Cetirizine 5-10 mg/day PO
- Levocetirizine 2.5-5 mg/day PO
- Fexofenadine 180 mg/day PO
- Loratadine 10 mg/day PO
-
First-generation (sedating) - if needed:
- Diphenhydramine 25-50 mg PO every 4-6 hours
- Hydroxyzine 10-25 mg PO every 6 hours
Per a 2024 meta-analysis (Jamjanya et al., J Allergy Clin Immunol Pract 2024), intravenous second-generation H1-antihistamines are preferred in the ED setting - they show comparable symptom relief to first-generation agents but with a significantly lower risk of return visits (OR 0.31) and adverse events (OR 0.24).
Dose escalation: If symptoms persist after 2 weeks, the dose can be increased up to 4x the standard dose before escalating therapy.
H2 Antihistamines (adjunctive): Famotidine 20 mg twice daily or ranitidine may be added to H1 antihistamines. Note: H2 blockers should NOT be used as monotherapy, as they may interfere with feedback inhibition of histamine release.
B. Severe Acute Urticaria with or without Angioedema
- H1-antihistamines: Diphenhydramine 25-50 mg PO, or 10-50 mg IV/IM every 4-6 hours (max 400 mg/24 hr)
- Corticosteroids (to prevent relapse; not immediate effect):
- Prednisone 10-60 mg PO every morning, tapering over 2 weeks
- Triamcinolone 40-60 mg IM (single dose)
- Dexamethasone 4-20 mg/day IV/IM (single dose or divided q6-12h depending on severity)
- Methylprednisolone 250 mg IV (or hydrocortisone 250 mg IV every 6 hours for 2-4 doses)
- Prescribe self-administered epinephrine auto-injector if patient has systemic symptoms
A 2024 systematic review (Chu et al., J Allergy Clin Immunol Pract) evaluated systemic corticosteroids for urticaria - they are effective for symptom control but their routine use in all acute urticaria cases remains debated; reserve for moderate-to-severe cases.
C. Anaphylaxis / Life-threatening Presentation
This is a medical emergency requiring immediate action:
| Priority | Action |
|---|---|
| A - Airway | Intubation if required |
| B - Breathing | Supplemental oxygen |
| C - Circulation | Epinephrine 0.3-0.5 mL of 1:1000 solution IM; repeat every 10-20 minutes as needed. IV saline/volume expanders |
| Adjuncts | IV methylprednisolone 1-2 mg/kg/day; diphenhydramine 25-50 mg IV + famotidine 20 mg IV |
In children: half-strength epinephrine dilution. Intubation or tracheotomy may be needed in rapidly progressive cases.
3. Special Considerations
- NSAIDs, opiates, vancomycin, alcohol - avoid as they cause nonspecific mast cell degranulation and can worsen urticaria
- Biopsy: If individual lesions persist >24 hours, perform skin biopsy to rule out urticarial vasculitis
- Omalizumab (anti-IgE monoclonal antibody, 150-300 mg SC monthly) - used primarily for chronic urticaria refractory to antihistamines; may be started in acute cases if antihistamines fail
- Skin testing/allergy referral: Consider in recurrent cases to identify a specific trigger
Summary Table
| Setting | Drug | Dose |
|---|---|---|
| Mild-moderate | Cetirizine (2nd gen AH) | 10 mg/day PO |
| Mild-moderate | Loratadine | 10 mg/day PO |
| Mild-moderate | Fexofenadine | 180 mg/day PO |
| Mild-moderate | Diphenhydramine (1st gen) | 25-50 mg PO q4-6h |
| Mild-moderate | Hydroxyzine (1st gen) | 10-25 mg PO q6h |
| Severe / ED | Diphenhydramine | 10-50 mg IV/IM q4-6h |
| Severe | Prednisone | 10-60 mg PO (taper x 2 wk) |
| Severe | Dexamethasone | 4-20 mg IV/IM |
| Anaphylaxis | Epinephrine | 0.3-0.5 mL of 1:1000 IM |
Sources:
- Goldman-Cecil Medicine, Table 407-2 (Treatment of Urticaria)
- Washington Manual of Medical Therapeutics, p. 435
- [Andrews' Diseases of the Skin, p. 3263]
- Jamjanya et al. 2024 - Meta-analysis on pharmacological treatments for acute urticaria (PMID 38280453)
- Chu et al. 2024 - Systemic corticosteroids for urticaria (PMID 38642709)
Vertigo in details
Reading File
Finding Sources
Searching PubMed
"vertigo" AND diagnosis AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Excellent - I have rich, comprehensive content from multiple textbooks plus a diagnostic algorithm image. Now I have everything needed to compose a detailed, well-structured answer.
Vertigo - A Comprehensive Clinical Overview
Definition
Vertigo is the perceived sensation of motion - usually spinning - of the person relative to the environment, or vice versa. It is not simply "dizziness"; the term is specifically reserved for an illusory sense of movement. It is almost always accompanied by nausea, vomiting, pallor, and diaphoresis. The sense of imbalance often accompanies an attack but dissipates when the episode ends.
True vertigo most often indicates dysfunction of the vestibular system, either peripheral (inner ear or vestibular nerve) or central (brainstem, cerebellum, thalamus, or cortex).
Classification of Dizziness
Before labeling a complaint as vertigo, it must be distinguished from the four major categories of dizziness:
| Type | Description | Common Cause |
|---|---|---|
| Vertigo | Illusion of spinning/motion | Vestibular disorder |
| Presyncope | Feeling of impending faint | Cardiovascular, orthostatic |
| Disequilibrium | Unsteadiness without spinning | Neurological, musculoskeletal |
| Lightheadedness | Vague "floating" sensation | Anxiety, hyperventilation, medications |
Peripheral vestibular disorders account for 38-56% of all persistent dizziness cases. Psychogenic causes account for 6-33%. Central etiologies are uncommon, <10% of cases. - Textbook of Family Medicine 9e
Diagnostic Framework: Episodic vs. Constant
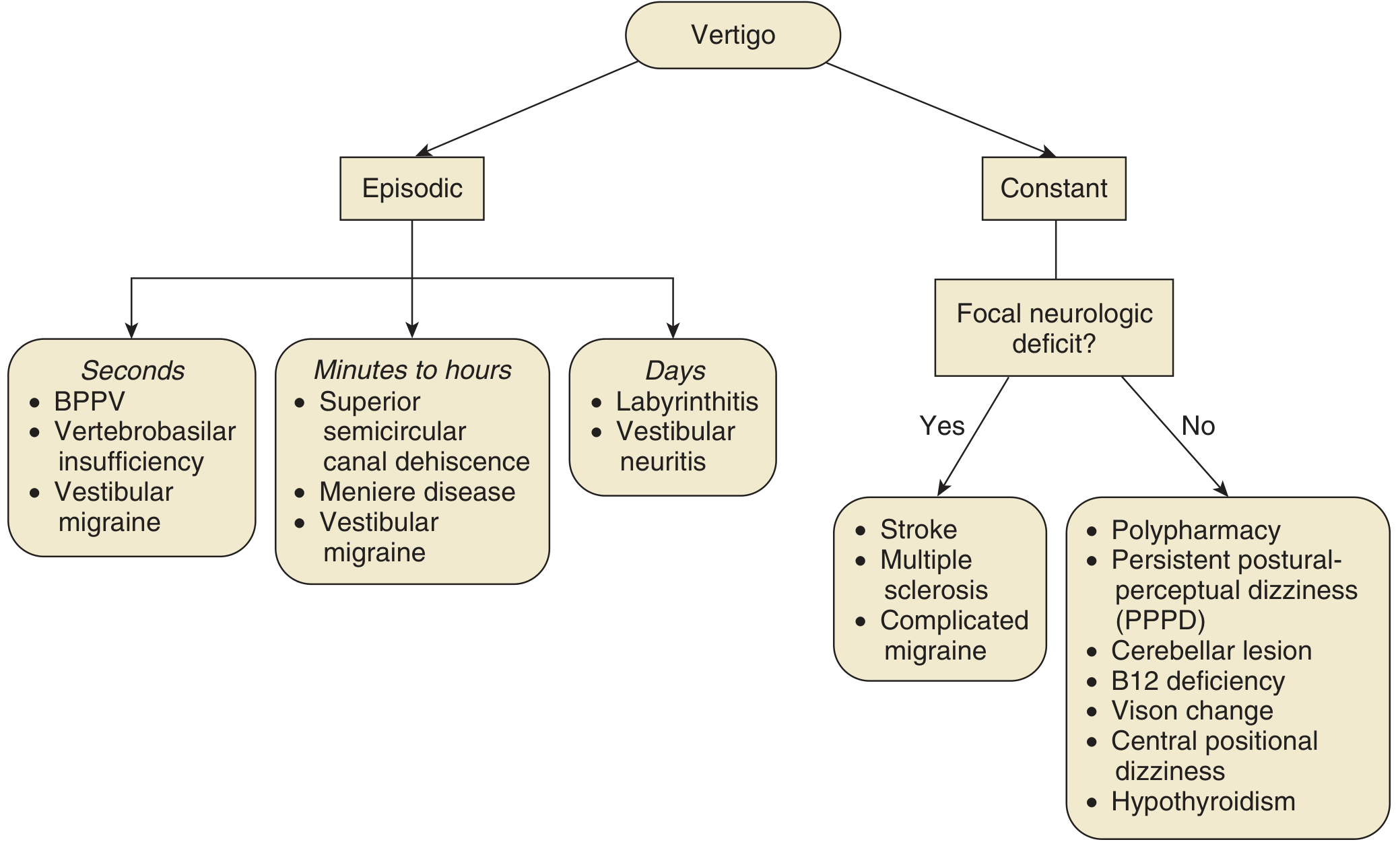
Differential diagnosis of vertigo by duration and associated features - Cummings Otolaryngology
Causes of Vertigo
A. Peripheral Causes (Inner Ear / Vestibular Nerve)
| Condition | Key Features | Pathophysiology |
|---|---|---|
| BPPV | Brief (<30 sec), positional, fatigable episodes | Otoliths displaced into semicircular canals (posterior > horizontal > anterior) |
| Vestibular neuritis | Sudden onset, severe, days-long; NO hearing loss | Viral/inflammatory damage to vestibular nerve |
| Labyrinthitis | Like vestibular neuritis + hearing loss | Inflammation of both vestibular and cochlear components |
| Meniere disease | Triad: episodic vertigo + tinnitus + fluctuating hearing loss | Endolymphatic hydrops (excessive endolymph) |
| Perilymphatic fistula | After Valsalva, trauma | Abnormal opening between middle and inner ear |
| Acoustic neuroma | Slowly progressive unilateral hearing loss, rare vertigo | Schwannoma of CN VIII |
| Acute otitis media | Ear pain, fever | Middle ear infection |
| Motion sickness | Triggered by movement | Sensory mismatch |
B. Central Causes (Brainstem / Cerebellum)
- Vertebrobasilar insufficiency (VBI) / posterior circulation TIA or stroke
- Cerebellar hemorrhage or infarction
- Migrainous (vestibular) vertigo
- Multiple sclerosis
- Temporal lobe epilepsy
- Subclavian steal syndrome
- Tumors
- Encephalitis, meningitis, brain abscess
- Postconcussive syndrome / temporal bone fracture
C. Systemic / Other Causes
- Ototoxic drugs: aminoglycosides, anticonvulsants, quinine, quinidine, minocycline, loop diuretics
- Cardiovascular: orthostatic hypotension, dysrhythmia
- Metabolic: anemia, dehydration, hypoglycemia, hypothyroidism, B12 deficiency
- Cervicogenic dizziness
- Persistent postural-perceptual dizziness (PPPD)
Peripheral vs. Central Vertigo: Key Distinguishing Features
| Feature | Peripheral | Central |
|---|---|---|
| Onset | Sudden, episodic | Gradual, often constant |
| Severity | Usually severe | Mild to moderate |
| Nausea/vomiting | Prominent | Less prominent |
| Nystagmus | Horizontal or rotatory; direction-fixed; fatigable | May be vertical; direction-changing; non-fatigable |
| Hearing loss | May be present | Usually absent |
| Neurological signs | Absent | Often present (diplopia, dysarthria, ataxia, weakness) |
| Loss of consciousness | Absent | Possible |
| Fixation suppression | Suppresses nystagmus | Does NOT suppress nystagmus |
| Falls | Falls toward affected side | Falls in any direction; severe gait ataxia |
History Taking
A thorough history provides 85% of the diagnostic information. Key elements include:
- Description of the sensation (spinning, floating, tilting?)
- Onset: acute or gradual
- Duration: seconds (BPPV), minutes-hours (Meniere, TIA), days (vestibular neuritis)
- Triggers: position change (BPPV), Valsalva (fistula), spontaneous (neuritis)
- Associated symptoms: hearing loss, tinnitus, headache, neurologic deficits
- Medications (ototoxic drugs)
- Cardiovascular risk factors (for TIA/stroke workup)
Physical Examination
Essential Tests
-
Dix-Hallpike Maneuver - gold standard for diagnosing BPPV
- Patient sits, head rotated 45°, rapidly lowered supine with head extended past table
- Positive result: latency of 5-20 sec, rotatory upbeat nystagmus toward the affected (down) ear, duration <30 seconds, fatigable on repetition
- Lack of fatigability or persistence of nystagmus suggests CNS cause
-
HINTS Examination (for Acute Vestibular Syndrome - constant vertigo):
- Head Impulse Test: positive (corrective saccade) = peripheral; negative = central (concerning)
- Nystagmus: unidirectional = peripheral; direction-changing = central
- Test of Skew: absent skew deviation = peripheral; present = central
- Note: HINTS should only be applied in patients with continuous (not episodic) vertigo - do NOT apply in BPPV
-
Orthostatic blood pressure - cardiovascular etiology
-
Weber and Rinne tuning fork tests - hearing lateralization
-
Romberg test and gait assessment (including tandem walking)
-
Full cranial nerve examination
-
Pneumatic otoscopy - elicits vertigo in perilymphatic fistula
Investigations
| Test | Indication |
|---|---|
| Audiogram | When hearing involvement suspected or unclear etiology |
| Electronystagmography (ENG) | Objective localization of vestibular lesion; includes caloric testing |
| MRI brain | Unilateral otologic symptoms, suspected central cause, acoustic neuroma, MS |
| CT brain | Urgent if cerebellar hemorrhage or infarct suspected |
| Blood glucose | Rule out hypoglycemia |
| CBC, electrolytes | Suspected anemia or dehydration |
| ECG | Suspected cardiac arrhythmia or ischemia |
| RPR, B12, folate | When systemic cause suspected |
| Drug screen / heavy metals | Appropriate toxicology workup |
MRI is the preferred imaging modality for posterior fossa lesions, acoustic neuroma, and MS. Routine CT or MRI is not indicated for straightforward peripheral vertigo such as BPPV. - Rosen's Emergency Medicine
Treatment
1. BPPV - Canalith Repositioning Maneuvers
Epley Maneuver (posterior canal BPPV) - most effective treatment:
- A series of four head positions, each held for 30 seconds
- Success rate >80% in single treatment session
- Brandt-Daroff exercises can be taught for home use
Semont Maneuver - alternative for posterior canal BPPV
Supine roll test / Barbecue roll - for horizontal canal BPPV
Patients can expect gradual resolution over 4-6 weeks with supportive therapy even without repositioning. - Textbook of Family Medicine
2. Vestibular Neuritis / Labyrinthitis
- Corticosteroids (methylprednisolone 100 mg/day tapering over 3 weeks) - to shorten duration of acute episode
- Vestibular suppressants (short-term use only, to control acute symptoms):
- Meclizine (Antivert) - directly inhibits vestibular-cerebellar pathways
- Dimenhydrinate (Dramamine) - motion sickness and acute vertigo
- Diazepam - for severe acute episodes
- Vestibular rehabilitation - essential for long-term recovery; exercises promote central compensation
- Labyrinthitis: add antibiotics if bacterial; antivirals for suspected viral etiology
3. Meniere Disease
- Low-sodium diet (<2000 mg/day), diuretics (hydrochlorothiazide, acetazolamide)
- Betahistine - widely used in Europe to reduce attack frequency
- Vestibular suppressants for acute attacks (meclizine, diazepam)
- Intratympanic corticosteroids - for refractory disease
- Intratympanic gentamicin - ablates vestibular function on affected side (last resort)
- Endolymphatic sac surgery - for severe medically refractory cases
4. Vestibular Migraine
- Acute: triptans, NSAIDs
- Prophylaxis: valproate, topiramate, beta-blockers, tricyclics
5. Pharmacological Vestibular Suppressants (General)
| Drug Class | Drug | Use |
|---|---|---|
| Antihistamines | Meclizine 12.5-25 mg q8h; Dimenhydrinate 50-100 mg q4-6h | Acute vertigo, motion sickness |
| Benzodiazepines | Diazepam 2-5 mg; Lorazepam 1-2 mg | Acute severe vertigo (short-term) |
| Phenothiazines | Prochlorperazine 5-10 mg IV/IM | Nausea/vomiting with vertigo |
| Anticholinergics | Scopolamine patch | Motion sickness |
| Calcium channel blocker | Flunarizine | Vestibular migraine prophylaxis |
Vestibular suppressants should be used SHORT-TERM only - prolonged use delays central compensation and functional recovery. - Rosen's Emergency Medicine
6. Vestibular Rehabilitation
Per the 2022 APTA Clinical Practice Guideline (PMID 34864777), vestibular rehabilitation is strongly recommended for peripheral vestibular hypofunction. It includes:
- Gaze stabilization exercises
- Habituation exercises
- Balance and gait training
7. Central Vertigo / Posterior Circulation Stroke
- Emergency management: airway, antiplatelet/anticoagulation therapy as appropriate
- Neurosurgery consult for cerebellar hemorrhage
- MRI for diagnosis; CT urgent if hemorrhage suspected
Red Flags - Always Suspect Central Cause
- New onset severe headache ("worst of my life")
- Diplopia, dysarthria, dysphagia
- Facial or limb numbness/weakness
- Persistent or direction-changing nystagmus
- Vertical nystagmus (always central)
- Inability to walk (severe truncal ataxia)
- Non-fatigable nystagmus on Dix-Hallpike
- Multiple strokes risk factors (age, HTN, DM, AF, prior stroke)
- Loss of consciousness
Sources
- Textbook of Family Medicine 9e - Chapter 18
- Rosen's Emergency Medicine - Chapter 15
- Cummings Otolaryngology Head and Neck Surgery - Chapter 137
- Shah VP et al. 2023 - Diagnostic accuracy of physical examination for acute vertigo/dizziness: GRACE-3 systematic review (PMID 36453134)
- Hall CD et al. 2022 - APTA Clinical Practice Guideline: Vestibular Rehabilitation for Peripheral Vestibular Hypofunction (PMID 34864777)
This is a shared conversation. Sign in to Orris to start your own chat.