Ecg all disease with figure
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching the Web
ECG all diseases patterns recognition guide with figures 2024
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Now I have comprehensive material. Let me compile a detailed, well-organized response with all ECG diseases and figures.
ECG Findings in All Major Diseases - with Figures
Here is a complete guide to ECG patterns across all major disease categories, sourced from Tintinalli's Emergency Medicine, Fuster and Hurst's The Heart, and Braunwald's Heart Disease.
How to Read an ECG - Quick Reference
Each small box = 0.04 sec (horizontal) and 0.1 mV (vertical). Normal values:
- PR interval: 120-200 ms
- QRS duration: <120 ms
- QTc: <440 ms (male), <460 ms (female)
- P wave: upright in I and II, inverted in aVR
1. Myocardial Infarction (STEMI)
ECG Criteria:
- ST-segment elevation in the territory of the affected artery
- Reciprocal ST-segment depression in opposite leads
- Later: Q waves develop, T waves invert
| Territory | Elevated Leads | Culprit Artery |
|---|---|---|
| Anteroseptal | V1, V2, (V3) | Distal LAD |
| Anterior | V1-V4 | LAD |
| Anterolateral | V1-V6, I, aVL | Proximal LAD |
| Lateral | I, aVL | Circumflex |
| Inferior | II, III, aVF | RCA (80%) |
| True Posterior | Tall R in V1-V2, R/S ≥1 | RCA or Cx |
| Right Ventricular | II, III, aVF + ST elevation in V3R-V6R | Proximal RCA |
(Tintinalli's Emergency Medicine, Table 49-4)
Anterior STEMI - ST elevation in I, V1, V2, V3 (distal LAD occlusion):
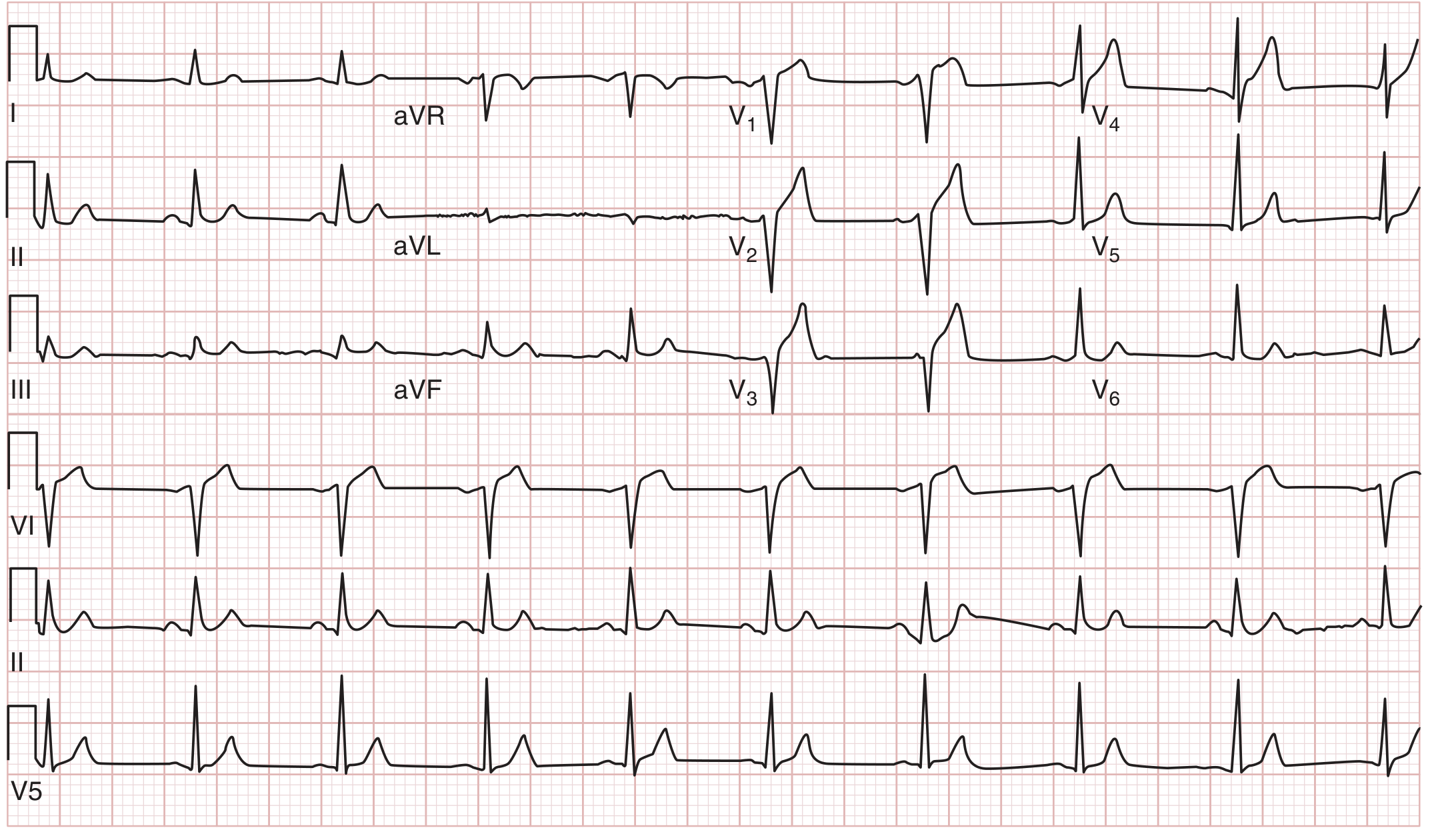
FIGURE: Anterior MI (distal LAD). ST elevation in I, V1, V2, V3 with absence of reciprocal ST depression in II, III, aVF. - Tintinalli's Emergency Medicine
Inferior + Right Ventricular STEMI - ST elevation in II, III, aVF with right-sided leads showing RV involvement:
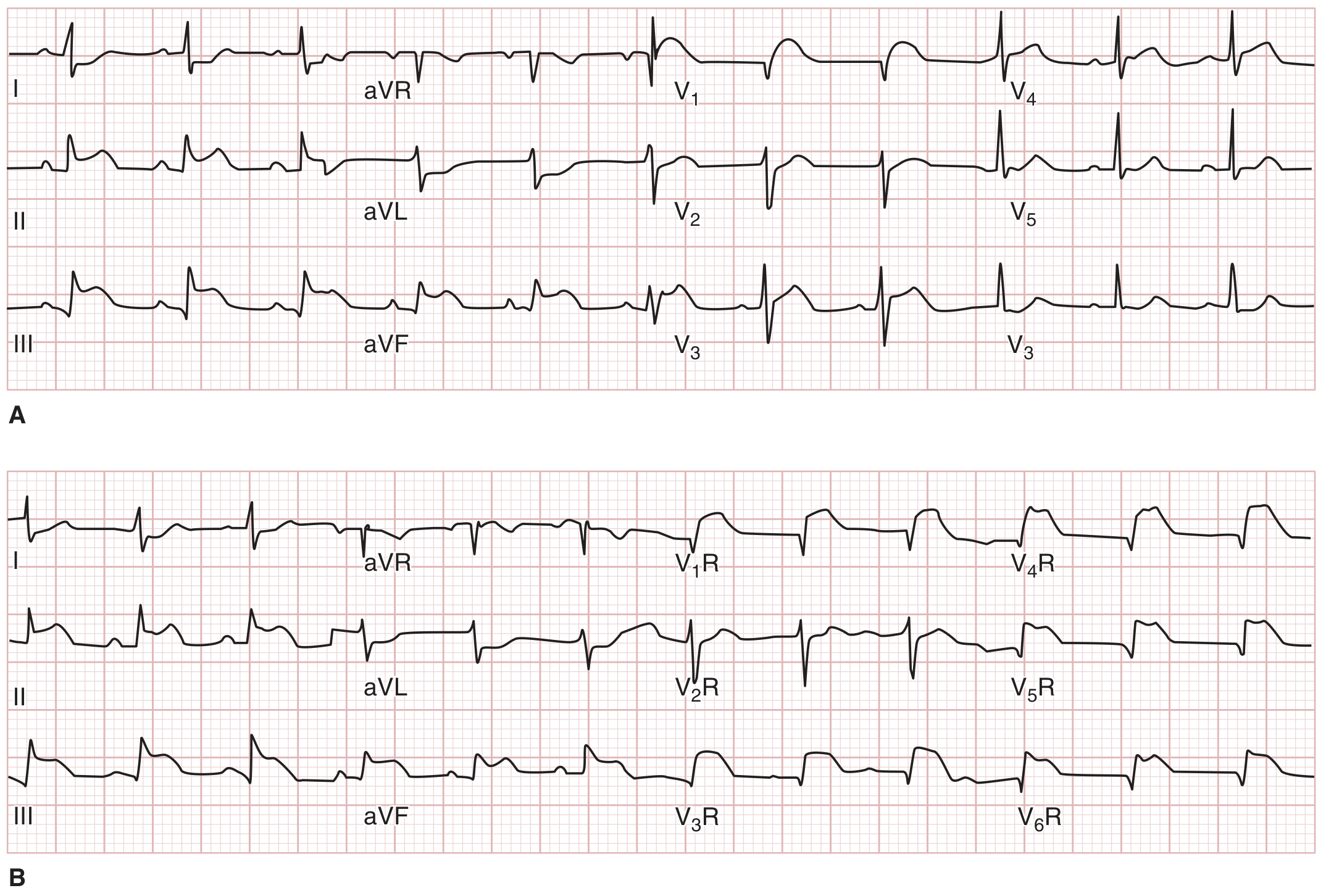
FIGURE: Inferior STEMI (A) with right ventricular leads (B) confirming RV infarction. ST elevation in V3R-V6R = RV MI. Always obtain right-sided leads with inferior STEMI. - Tintinalli's Emergency Medicine
Key ECG pitfalls with STEMI mimics (from Tintinalli's, Table 49-6):
- Early repolarization, LVH, pericarditis, myocarditis, LV aneurysm, hypothermia, LBBB, Takotsubo cardiomyopathy can all cause ST elevation without true MI
2. Left Bundle Branch Block (LBBB) in the Context of MI
New LBBB can be a STEMI equivalent. The Sgarbossa criteria help identify true MI in LBBB:
Concordant ST elevation (same direction as QRS) = strongly suggestive of AMI
Excessive discordant ST elevation (>5 mm opposite QRS) = weakly suggestive
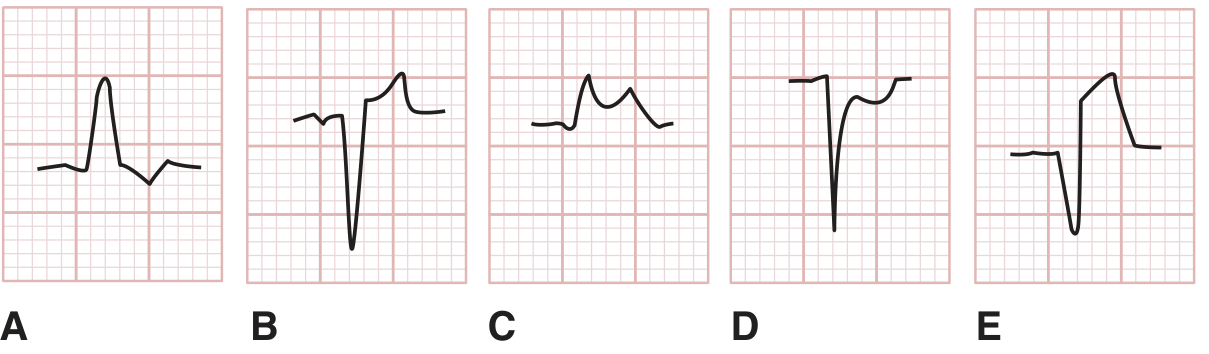
FIGURE: ST abnormalities in LBBB. A=discordant ST depression (normal), B=discordant ST elevation (normal), C=concordant ST elevation (strongly suggests AMI), D=concordant ST depression (suggests AMI), E=>5mm discordant ST elevation (weakly suggests AMI). - Tintinalli's Emergency Medicine
3. Wellens' Syndrome
Wellens' syndrome = critical LAD stenosis, seen during pain-free periods.
Two patterns in V2-V3:
- Type A (25%): Biphasic T waves
- Type B (75%): Deep symmetric T-wave inversion
Management: urgent cath - these patients are at high risk of anterior STEMI. Do NOT stress test.
4. Pulmonary Embolism (PE)
ECG in PE is non-specific but important. Changes result from acute RV dilatation.
Classic S1Q3T3 pattern (present in only ~10% of PE cases):
- S wave in lead I
- Q wave in lead III
- T-wave inversion in lead III
More common findings (in order of frequency):
- Sinus tachycardia (most common)
- T-wave inversion in V2-V3 (best predictor of high-risk PE and RV dysfunction)
- Incomplete or complete RBBB
- Right axis deviation
- Atrial fibrillation
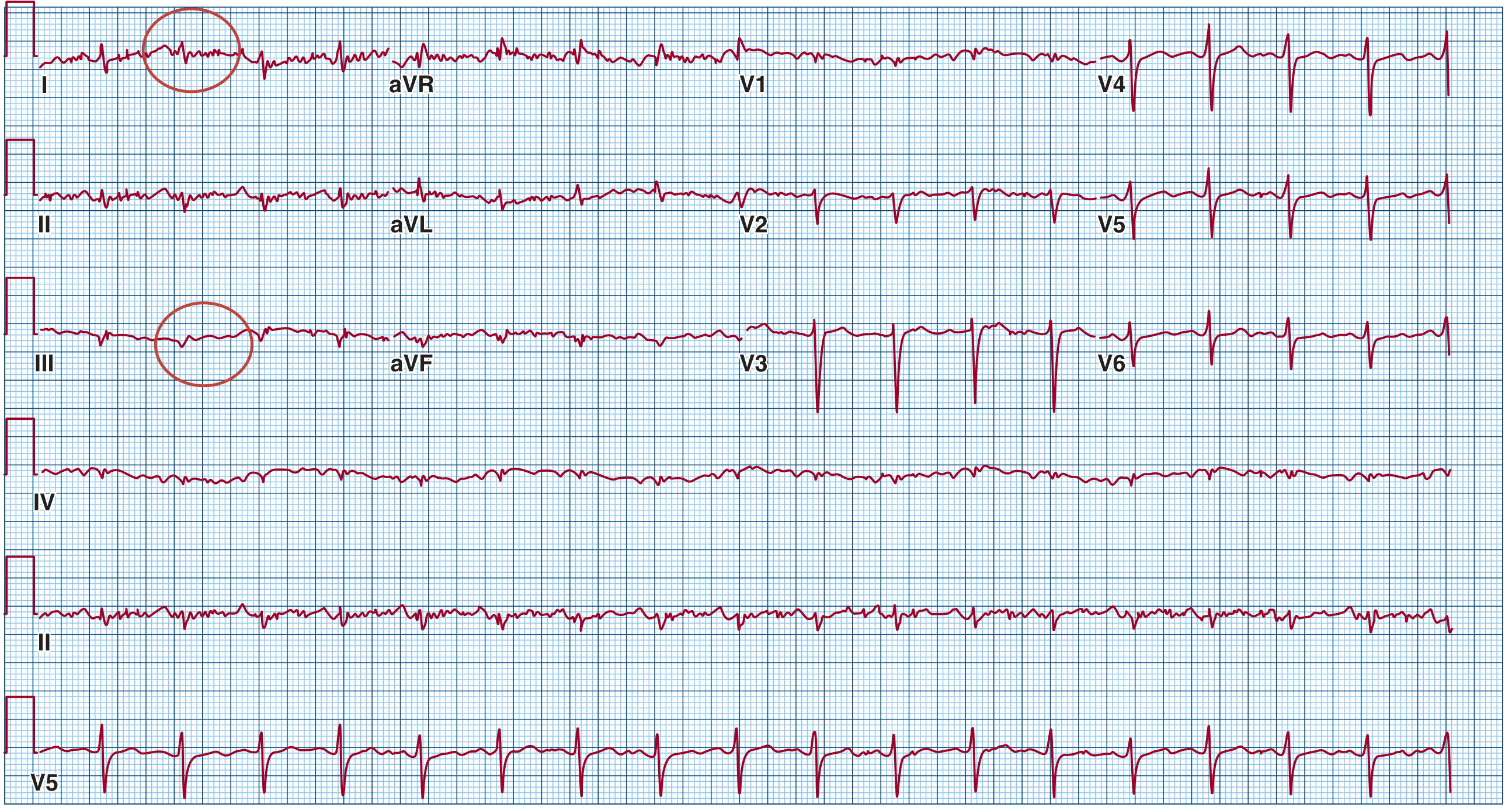
FIGURE: Twelve-lead ECG from a 60-year-old man with massive PE and cardiogenic shock. Note sinus tachycardia (116 bpm), right axis deviation, classic S1Q3T3 (circled), and flattened T-wave in V. - Fuster and Hurst's The Heart
5. Wolff-Parkinson-White (WPW) Syndrome
ECG Triad of WPW in sinus rhythm:
- PR interval < 120 ms (short PR)
- Delta wave (slurred upstroke at start of QRS)
- Widened QRS complex
Associated arrhythmias:
| Arrhythmia | QRS | Rate | Regularity |
|---|---|---|---|
| Orthodromic AVRT (65%) | Narrow | 160-220 | Regular |
| Antidromic AVRT (5-10%) | Wide | 160-220 | Regular |
| AF with WPW (25%) | Wide, bizarre | >200 | Irregular |
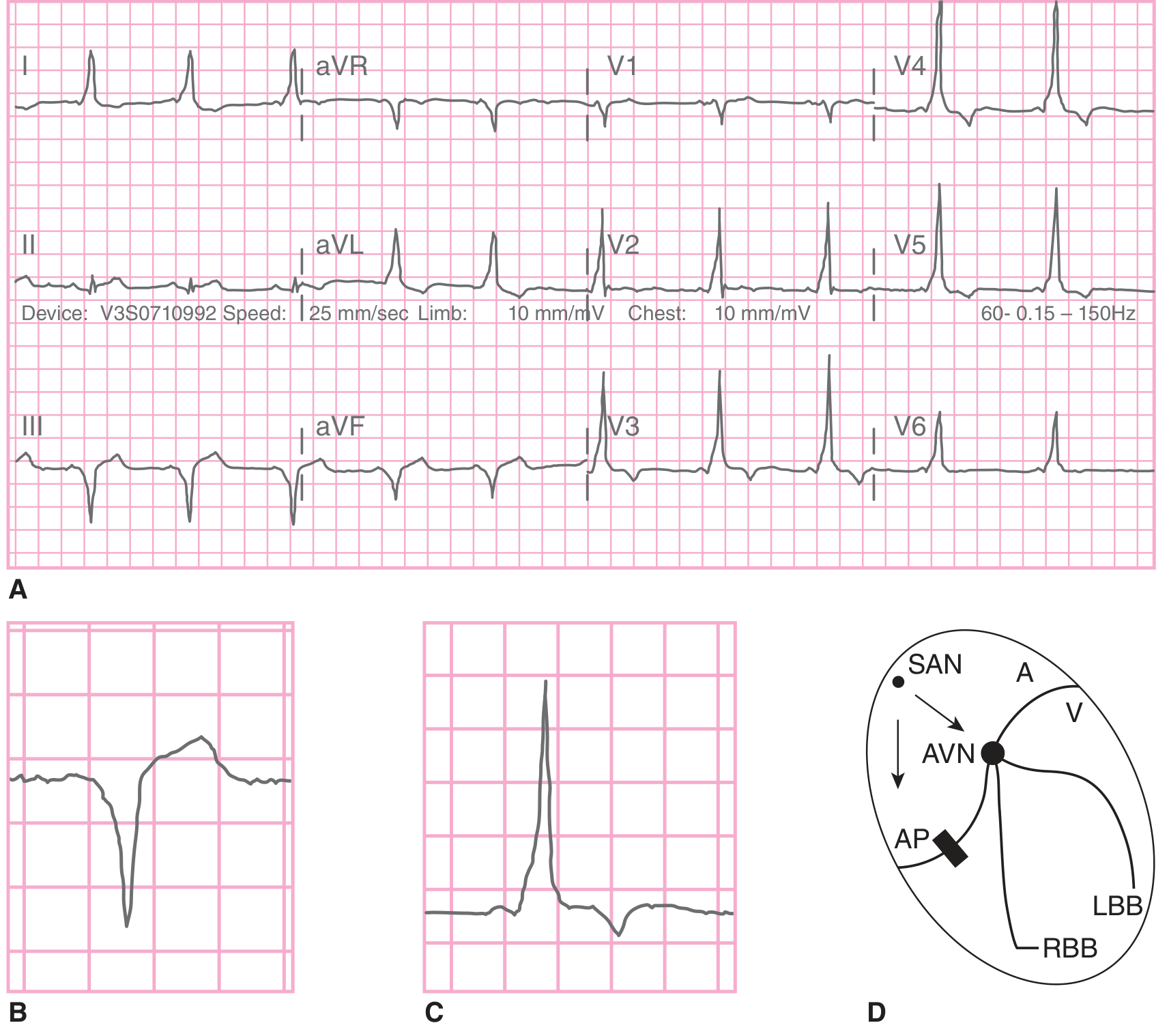
FIGURE: WPW syndrome. A=12-lead ECG in sinus rhythm with short PR, delta wave, wide QRS. B=negative delta (in lead with predominant negative deflection). C=positive delta. D=conduction diagram showing dual pathway via AVN and accessory pathway (AP). - Tintinalli's Emergency Medicine
Avoid in AF + WPW: AV nodal blockers (adenosine, verapamil, diltiazem, digoxin, beta-blockers) as they may precipitate ventricular fibrillation by blocking the AV node and forcing conduction exclusively through the fast accessory pathway.
6. Brugada Syndrome
Characteristic ECG pattern (leads V1-V3):
- Prominent J-wave
- Downsloping ST-segment elevation
- QRS resembles right bundle branch block
- This "type 1" (coved type) pattern is required for diagnosis
Associated with: polymorphic VT degenerating to VF, sudden cardiac death. Common in Southeast Asian males. Autosomal dominant (SCN5A loss-of-function mutation).
Triggers that unmask pattern: fever, sodium channel blockers, cocaine, alcohol.
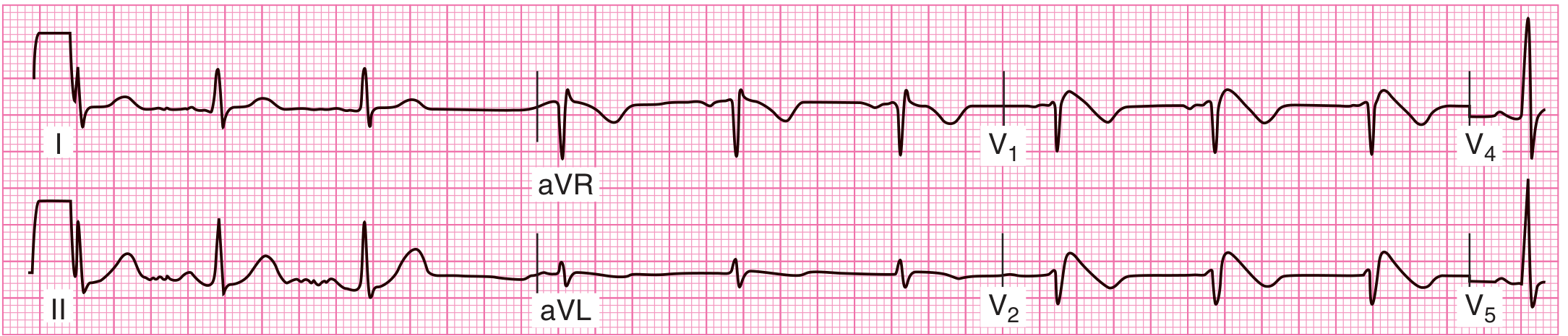
FIGURE: Brugada syndrome. Characteristic downsloping ("coved") ST-segment elevation in V1-V2, QRS resembling RBBB. - Tintinalli's Emergency Medicine
7. Long QT Syndrome
Diagnosis: Corrected QT (QTc) > 440 ms in males, > 460 ms in females
Bazett's formula: QTc = QTm / √(R-R interval in seconds)
Causes:
- Congenital (hereditary):
- Romano-Ward syndrome (autosomal dominant, no deafness)
- Jervell and Lange-Nielsen syndrome (autosomal recessive, with nerve deafness)
- Acquired: Hypokalemia, hypomagnesemia, hypocalcemia, drugs (antiarrhythmics, antipsychotics, macrolides, fluoroquinolones), CNS pathology
Risk: Torsades de pointes (polymorphic VT) → ventricular fibrillation → sudden death.
Management: Avoid QT-prolonging drugs, beta-blockers for prevention, ICD if syncope occurs despite beta-blockers.
8. Short QT Syndrome
Diagnosis: QTc < 340 ms (pathological)
Associations: Hypercalcemia, hyperkalemia, acidosis, genetic (autosomal dominant). ECG may also show early repolarization in inferolateral leads (65% of patients). Linked to AF, polymorphic VT, VF, and sudden cardiac death.
9. Early Repolarization Syndrome
ECG Criteria (most prominent in mid-to-lateral precordial leads):
- Prominent notch-like J wave on QRS downslope
- Upsloping ST-segment elevation
- Reciprocal ST-segment depression in aVR
Present in 1-2% of adults (higher in athletes, up to 100% in endurance athletes). Normalizes with exercise or rapid pacing.
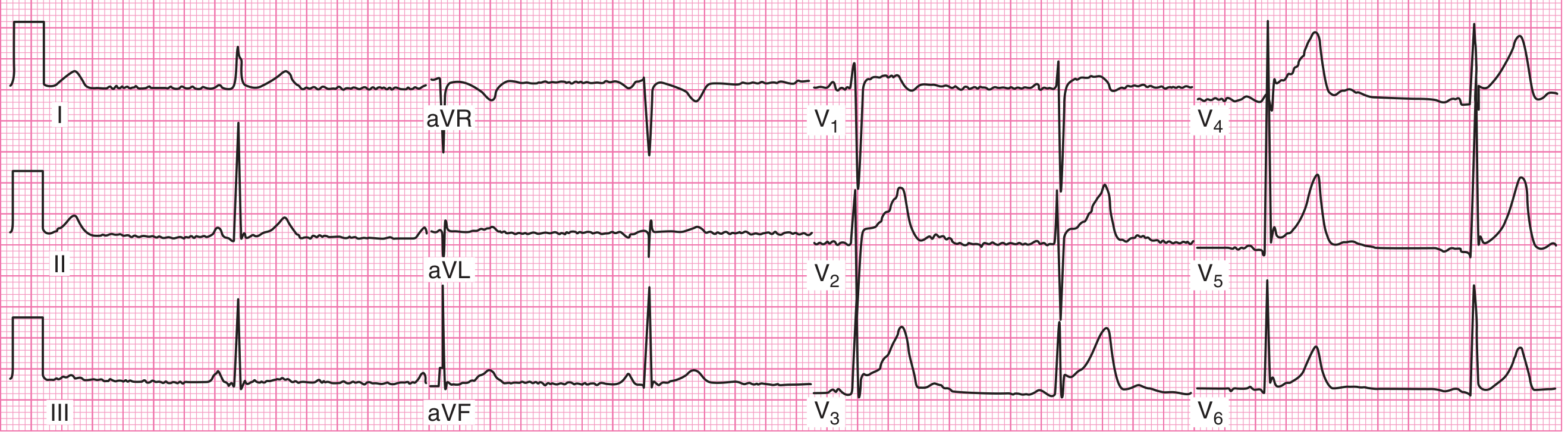
FIGURE: Early repolarization syndrome. Note the prominent notch-like J wave on the QRS downslope and upsloping ST segment, most visible in V2. - Tintinalli's Emergency Medicine
10. Hypertrophic Cardiomyopathy (HCM)
ECG findings (abnormal in majority of patients):
- Left ventricular hypertrophy pattern (high-voltage QRS)
- Lateral/inferior T-wave inversions (deep, symmetric)
- Pathological Q waves in lateral leads (I, aVL, V5-V6) - due to septal hypertrophy
- Apical variant: massive T-wave inversions in V4-V6 ("giant negative T waves")
- Preexcitation or AV block = red flag for HCM phenocopy
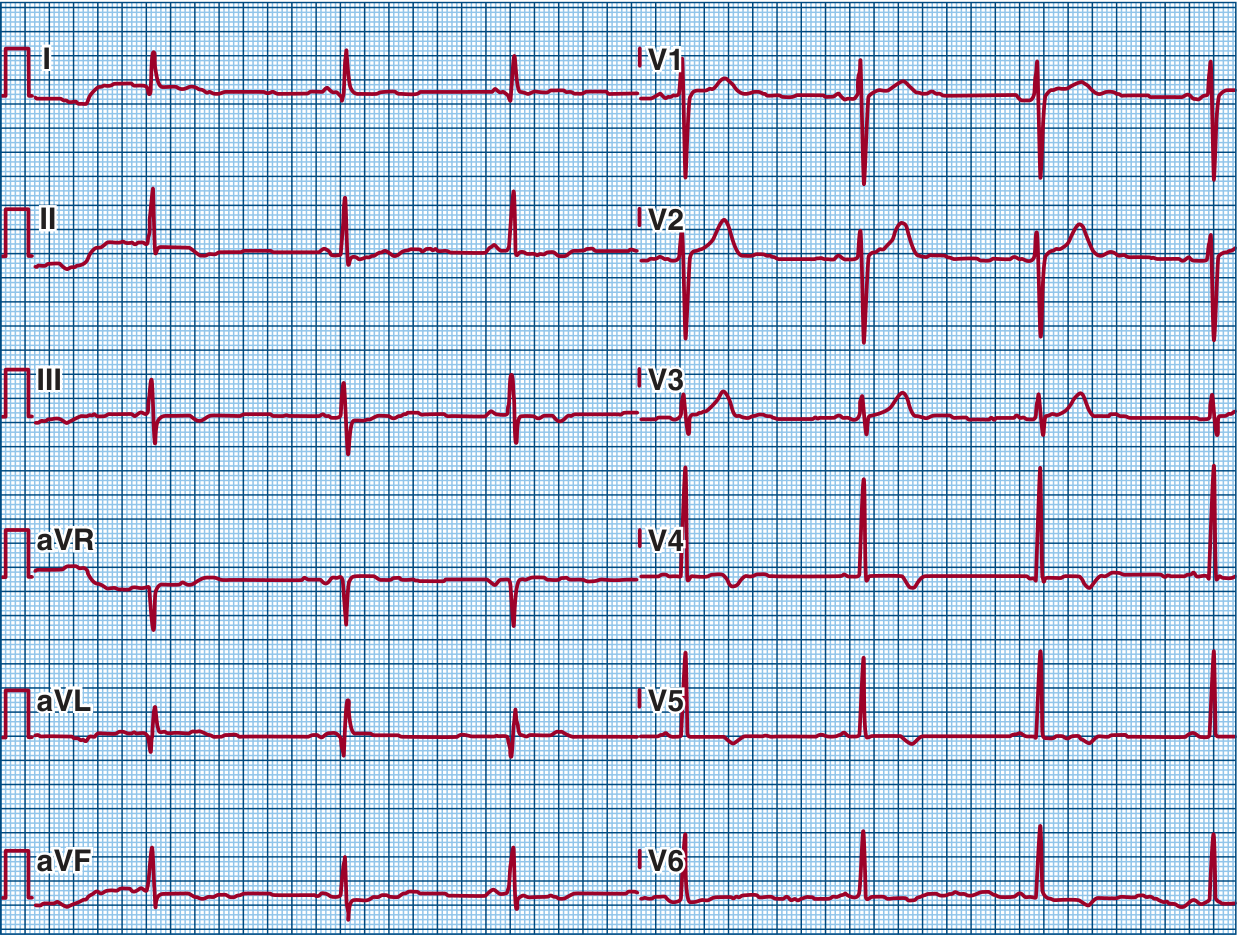
FIGURE: HCM - possible LVH, anterior and inferior negative T waves, lateral pathological Q waves. - Fuster and Hurst's The Heart
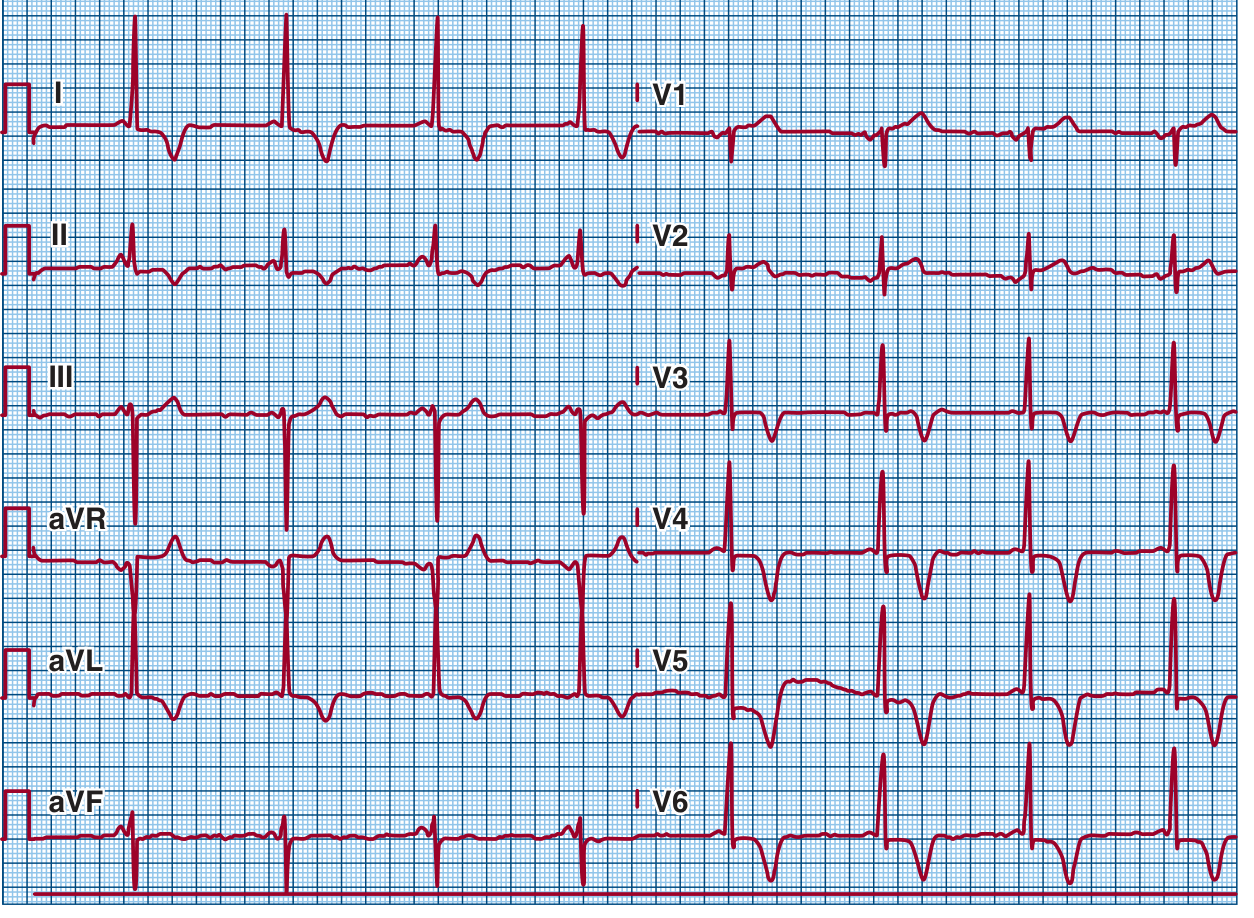
FIGURE: Apical HCM - LVH with massive deep symmetric negative T waves in anterolateral leads (V4-V6). This is the "apical variant" or Yamaguchi syndrome. - Fuster and Hurst's The Heart
11. Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC)
ECG findings:
- T-wave inversions in right precordial leads (V1-V3 or beyond) - most common
- Epsilon wave: small notch at end of QRS in V1-V3 (pathognomonic but present in <30%)
- Prolonged terminal QRS activation (>110 ms in V1)
- VT with left bundle branch block morphology (origin from RV)
- Right axis deviation
12. Atrial Fibrillation (AF)
ECG Hallmarks:
- Absent P waves - replaced by irregular fibrillatory baseline (f-waves), best seen in V1
- Irregularly irregular RR intervals
- Ventricular rate: 100-180/min if uncontrolled
Associated conditions visible on ECG:
- Ventricular pre-excitation (WPW with AF) - wide bizarre QRS, rate >200
- AF with LBBB or RBBB - wide complex irregular tachycardia
- AF with complete heart block - slow regular ventricular rhythm with AF background
13. Atrial Flutter
ECG Hallmarks:
- Sawtooth flutter waves at 300 bpm (typical/counterclockwise flutter)
- Usually with 2:1 AV block (ventricular rate ~150 bpm)
- Flutter waves most visible in II, III, aVF and V1
- Negative flutter waves in inferior leads, positive in V1 (typical flutter)
- Atypical (clockwise) flutter: positive in inferior leads, negative in V1
14. AV Blocks
| Degree | PR Interval | QRS | Key Feature |
|---|---|---|---|
| 1st degree | >200 ms, constant | Normal | Prolonged PR, all P waves conduct |
| 2nd degree Mobitz I (Wenckebach) | Progressively lengthens | Normal | PR lengthens until dropped beat, then resets |
| 2nd degree Mobitz II | Constant PR | May be wide | Sudden dropped beat without prior PR change |
| 3rd degree (complete) | No relationship | Wide (ventricular) or narrow (junctional) | P waves and QRS totally dissociated |
Clinical note: Mobitz II and 3rd degree block require pacemaker implantation. Mobitz I is usually benign (nodal).
15. Bundle Branch Blocks
Right Bundle Branch Block (RBBB):
- QRS > 120 ms
- RSR' pattern in V1 ("rabbit ears" or M-shaped)
- Wide S wave in I, V5, V6
- Can be normal variant or reflect organic heart disease (RV overload, PE)
Left Bundle Branch Block (LBBB):
- QRS > 120 ms
- Broad monophasic R in I, V5, V6 (no Q, no S)
- Deep QS or rS in V1
- Discordant ST-T changes
- New LBBB = STEMI equivalent until proven otherwise
16. Pericarditis
Classic ECG stages:
| Stage | Timing | ECG Finding |
|---|---|---|
| 1 | Days 1-2 | Diffuse concave ST elevation + PR depression (all leads except aVR/V1) |
| 2 | Days 3-7 | ST returns to baseline, T waves flatten |
| 3 | Days 7-14 | T-wave inversions (diffuse) |
| 4 | Weeks later | Normal or persistent T-wave inversions |
Key differentiator from MI: Diffuse ST elevation (all territories), PR depression, concave (saddle-shaped) ST morphology, no reciprocal changes.
17. Hyperkalemia
| K+ Level | ECG Changes |
|---|---|
| 5.5-6.5 mEq/L | Tall peaked ("tented") T waves in precordial leads |
| 6.5-7.5 mEq/L | PR prolongation, P-wave flattening/absence |
| 7.5-8.0 mEq/L | QRS widening |
| >8.0 mEq/L | Sine wave pattern, VF, cardiac arrest |
18. Hypokalemia
| K+ Level | ECG Changes |
|---|---|
| Mild-moderate | T-wave flattening, U-wave prominence |
| Severe | T-wave inversion, prominent U waves merging with T waves, apparent QT prolongation (actually QU prolongation), ST depression |
19. Hypercalcemia / Hypocalcemia
- Hypercalcemia: Short QT interval (QTc < 340 ms), short ST segment
- Hypocalcemia: Long QT interval (QTc > 460 ms), long ST segment (without T-wave prolongation)
20. Hypothermia
ECG findings:
- Osborne (J) waves: Positive deflection at the QRS-ST junction, most prominent in precordial leads - classic for hypothermia
- Bradycardia, prolonged PR, QRS, QT intervals
- Atrial fibrillation is common at < 32°C
- Ventricular fibrillation can occur at < 28°C
- Shivering artifact (muscle tremor noise on baseline)
21. Digoxin Effect vs. Toxicity
Digoxin effect (therapeutic):
- "Reverse tick" or "scooped" ST-segment depression
- T-wave inversion
- QT shortening
- PR prolongation
Digoxin toxicity:
- Virtually any arrhythmia, but classic patterns include:
- Bidirectional VT (alternating QRS axis beat-to-beat)
- Regularized AF (AF + complete AV block = Junctional tachycardia)
- PVCs, especially bigeminy
- High-degree AV block
22. Acute Right Heart Strain / Cor Pulmonale
ECG findings:
- S1Q3T3 pattern
- Right axis deviation (>90°)
- Incomplete or complete RBBB
- P-pulmonale (tall peaked P waves >2.5 mm in II)
- Clockwise rotation (persistent rS pattern across precordium)
- T-wave inversions in V1-V4
23. Left Ventricular Hypertrophy (LVH)
Sokolow-Lyon criteria: S in V1 + R in V5 or V6 > 35 mm
Cornell criteria: R in aVL + S in V3 > 28 mm (men), > 20 mm (women)
Strain pattern: ST depression and T-wave inversion in lateral leads (I, aVL, V5-V6)
24. Syncope - Key ECG Clues
The 2017 ACC/AHA/HRS guidelines give a Class I recommendation for ECG in all patients with syncope. Specific ECG findings that identify the cause:
| ECG Finding | Probable Cause |
|---|---|
| QT prolongation | Long QT syndrome |
| Short PR + delta wave | WPW syndrome |
| RBBB pattern + ST elevation in V1-V3 | Brugada syndrome |
| ST elevation / Q waves | Acute MI |
| High-grade AV block | Conduction disease |
| T-wave inversion in V1-V3 | ARVC |
25. Catecholaminergic Polymorphic Ventricular Tachycardia (CPVT)
Resting ECG is usually normal (distinguishes from other channelopathies). May show sinus bradycardia. Diagnosis requires exercise/stress testing to provoke bidirectional or polymorphic VT. Gene: RYR2 (ryanodine receptor mutation). Treatment: beta-blockers + ICD.
Summary Table - ECG Pattern by Disease
| Disease | Rate | Rhythm | PR | QRS | ST | T waves | Other |
|---|---|---|---|---|---|---|---|
| Inferior STEMI | Usually normal | Sinus | Normal | Normal | Elevation II,III,aVF | Hyperacute | Reciprocal changes I,aVL |
| Anterior STEMI | Varies | Sinus/AF | Normal | Normal | Elevation V1-V4 | Hyperacute | Q waves develop |
| PE | Tachy | Sinus | Normal | ±Wide | Normal | T inversion V1-V3 | S1Q3T3, RBBB |
| Pericarditis | Normal | Sinus | PR depression | Normal | Concave diffuse elevation | Inversion (late) | No reciprocal changes |
| LBBB | Normal | Sinus | Normal | Wide >120ms | Discordant | Discordant | RSR' absent |
| RBBB | Normal | Sinus | Normal | Wide >120ms | Discordant | Discordant | RSR' in V1 |
| WPW | Normal | Sinus/SVT | Short <120ms | Wide, delta | Discordant | Discordant | Delta wave |
| Brugada | Normal | Sinus | Normal | Widened | Coved in V1-V3 | Normal | RBBB-like |
| Long QT | Normal | Sinus | Normal | Normal | Normal | May be abnormal | QTc >440ms |
| HCM | Normal | Sinus | Normal | High voltage | Normal | Deep inversion V4-V6 | Pathological Q waves |
| AF | 100-180 | Irregularly irregular | None | Normal | Normal | Normal | No P waves, f-waves |
| Atrial flutter | 150 (2:1) | Regular | None | Normal | Normal | Normal | Sawtooth waves |
| Hyperkalemia | Slow | Sinus→VF | Prolonged | Wide/sine wave | Normal | Peaked tall T | PR→QRS→sine wave |
| Digoxin effect | Slow | Various | Long | Normal | Scooped depression | Inverted | QT short |
| Hypothermia | Slow | AF or bradycardia | Long | Wide | Normal | Normal | Osborne J wave |
Sources: Tintinalli's Emergency Medicine (9th ed.); Fuster and Hurst's The Heart (15th ed.); Braunwald's Heart Disease (2-Vol Set). ECG figures reproduced from these authoritative clinical textbooks.
This is a shared conversation. Sign in to Orris to start your own chat.