lft interpretation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compose the full answer.
Liver Function Tests (LFTs) - Interpretation
LFTs is actually a misnomer - most tests measure cell damage, not true liver function. True function is assessed by albumin and prothrombin time (PT/INR). The panel is best interpreted by recognizing the dominant pattern of abnormality.
The Standard LFT Panel
| Test | Normal Range | What It Measures |
|---|---|---|
| ALT (SGPT) | 7-56 U/L | Hepatocyte injury (liver-specific) |
| AST (SGOT) | 10-40 U/L | Hepatocyte injury (less specific - also muscle, heart, RBC) |
| Alkaline Phosphatase (ALP) | 40-130 U/L | Biliary epithelium, bone |
| GGT | 9-48 U/L | Biliary tract, hepatocytes |
| Bilirubin (total) | 0.1-1.2 mg/dL | Heme metabolism |
| Albumin | 3.5-5.0 g/dL | Hepatic synthesis (chronic function) |
| PT/INR | PT: 11-13 sec | Hepatic synthesis (acute function) |
| LDH | Variable | Hepatocyte necrosis (non-specific) |
| Ammonia | 15-45 µmol/L | Hepatic detoxification |
Step 1: Identify the Dominant Pattern
Pattern 1 - Hepatocellular (Parenchymal) Injury
Predominant finding: AST and ALT markedly elevated (>3× ULN, often much higher)
- ALT is more liver-specific than AST
- ALP is normal or mildly elevated (<3× ULN)
- Bilirubin may be elevated (both fractions)
- Albumin and PT usually normal unless >80% liver destroyed
Degree of elevation and causes:
| AST/ALT elevation | Likely cause |
|---|---|
| Mild (<3× ULN) | NAFLD, chronic viral hepatitis, medications |
| Moderate (3-20× ULN) | Acute viral hepatitis, autoimmune hepatitis |
| Severe (>20× - into thousands) | Ischemic hepatitis, acetaminophen toxicity, fulminant hepatitis |
Key ratio: AST:ALT >2:1 strongly suggests alcoholic liver disease (Schwartz's Principles of Surgery)
Pattern 2 - Cholestatic Pattern
Predominant finding: ALP elevated (>3× ULN), often with elevated GGT and direct bilirubin
- AST/ALT normal or mildly elevated (<3× ULN)
- Serum cholesterol increased (in chronic cholestasis)
- Pruritus may be present
- GGT confirms ALP is of hepatic origin (not bone)
Intrahepatic vs Extrahepatic cholestasis:
| Feature | Intrahepatic | Extrahepatic |
|---|---|---|
| Direct bilirubin | Elevated | Elevated |
| ALP | Elevated | Markedly elevated |
| Causes | PBC, PSC, drugs, pregnancy, sepsis | Stones, stricture, tumor, PSC |
ALP isoenzyme differentiation: If GGT and 5'-nucleotidase are normal alongside elevated ALP, the excess ALP is likely of bone origin, not hepatic.
Pattern 3 - Mixed Pattern
Both hepatocellular enzymes AND cholestatic markers elevated - seen in drug-induced liver injury (DILI), overlap syndromes.
Step 2: Assess Hepatic Synthetic Function
These are the true tests of liver function:
Albumin
- Half-life = 15-20 days → marker of chronic hepatic dysfunction
- Low in cirrhosis, chronic hepatitis (when >80% parenchyma lost)
- NOT low in acute hepatitis (because liver is not substantially destroyed)
- Confounders: malnutrition, nephrotic syndrome, protein-losing enteropathy
Prothrombin Time (PT) / INR
- Half-life of factors = hours to days → marker of acute hepatic function
- Most sensitive test for acute hepatic failure
- All clotting factors (except Factor VIII) are made in the liver
- Prolonged PT not responding to vitamin K = severe hepatocellular disease
- Confounders: warfarin use, vitamin K deficiency
Step 3: Bilirubin Fractionation
Total bilirubin = Direct (conjugated) + Indirect (unconjugated)
Unconjugated (Indirect) Hyperbilirubinemia
Caused by problems upstream of conjugation:
| Step Affected | Cause |
|---|---|
| Excess heme breakdown | Hemolysis, large hematoma resorption, ineffective erythropoiesis |
| Impaired hepatocyte uptake | Gilbert syndrome, rifampin, probenecid |
| Impaired conjugation | Crigler-Najjar syndrome, hypothyroidism |
- Urine: no bilirubin (unconjugated is not water-soluble)
- Gilbert syndrome: benign, isolated mild unconjugated hyperbilirubinemia
Conjugated (Direct) Hyperbilirubinemia
Caused by problems at or downstream of conjugation:
| Cause | Example |
|---|---|
| Impaired canalicular secretion | Hepatitis, sepsis, drugs (estrogens, cyclosporine), Dubin-Johnson, Rotor syndrome |
| Intrahepatic cholestasis | PBC, alcohol, pregnancy (ICP), PSC |
| Extrahepatic obstruction | Choledocholithiasis, cholangiocarcinoma, pancreatic head carcinoma |
- Urine: bilirubinuria present (conjugated bilirubin is water-soluble)
- Conjugated hyperbilirubinemia = when >30% of total bilirubin is conjugated
Step 4: Classic Disease Patterns (Summary)
| Condition | AST/ALT | ALP | Bilirubin | Albumin | PT | Ammonia |
|---|---|---|---|---|---|---|
| Acute hepatitis | ↑↑↑ | ↑ (mild) | ↑ (both) | Normal | Normal | Normal |
| Cirrhosis | Normal/↓ or mildly ↑ | ↑ | ↑ (both) | ↓↓ | Prolonged | ↑ |
| Biliary obstruction | Normal/↑ (mild) | ↑↑↑ | ↑ (direct) | Normal | Normal | Normal |
| Space-occupying lesion (met/HCC) | Normal | ↑↑ | Normal | Normal | Normal | Normal |
| Fulminant hepatic failure | ↑↑↑↑ (>10,000) | ↑ | ↑ | ↓↓ | Prolonged | ↑↑ |
| Passive congestion (cardiac) | ↑ (mild) | ↑ (mild) | ↑ | Normal | Normal | Normal |
| Alcoholic liver disease | ↑↑ (AST:ALT >2:1) | ↑ | ↑ | ↓ | Prolonged | Variable |
Step 5: Key Ancillary Tests
- GGT: Confirms hepatic origin of elevated ALP; elevated 2-3× ULN in heavy drinkers; elevated in 70% of chronic alcoholics; elevated by drugs (phenytoin, valproate, barbiturates, methotrexate, warfarin)
- 5'-Nucleotidase: Confirms biliary origin; highest in cholestatic conditions
- Ammonia: Elevated only when >80% of liver tissue is destroyed; important in hepatic encephalopathy; pre-analytical errors are common (must be chilled on ice, tested immediately - levels rise ~20% in first hour; hemolysis and smoking falsely elevate)
- LDH: Rises in hepatocyte necrosis but very non-specific; isolated ALP + LDH elevation suggests space-occupying lesion
Pitfalls to Remember
- Normal LFTs don't exclude liver disease - cirrhosis can have near-normal transaminases
- ALP may be elevated physiologically - childhood growth, pregnancy; separate reference ranges needed for children
- Fasting matters - intestinal ALP can elevate total ALP by 30% for up to 12 hours post-meal (in Lewis-positive group B/O secretors)
- AST is non-specific - elevated in MI, rhabdomyolysis, hemolysis; always compare with ALT
- Albumin half-life is long - not useful for detecting acute liver failure
- INR is best for acute synthetic function assessment (hours to days for clotting factor turnover)
- Wilson's disease classically shows low ALP despite significant liver disease
Sources: Schwartz's Principles of Surgery 11th Ed. | Henry's Clinical Diagnosis and Management by Laboratory Methods | Quick Compendium of Clinical Pathology 5th Ed. | Harrison's Principles of Internal Medicine 22E (2025)
How do I interpret an abnormal AST:ALT ratio?
Finding Sources
Searching PubMed
AST ALT ratio liver disease diagnosis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Now I have comprehensive, multi-source data to write a detailed answer.
The AST:ALT Ratio (De Ritis Ratio) - Full Interpretation Guide
The AST:ALT ratio was first described by Fernando De Ritis in 1957 and remains one of the most practical single numbers in hepatology. Understanding it requires knowing why the two enzymes behave differently.
Why the Ratio Exists: Biochemical Basis
| Feature | AST | ALT |
|---|---|---|
| Subcellular location | ~80% mitochondrial, 20% cytoplasmic | Exclusively cytoplasmic |
| Tissue distribution | Liver, cardiac muscle, skeletal muscle, kidney, brain, lung, pancreas | Primarily liver and kidney (liver-specific) |
| Specificity for liver | Less specific | More specific |
| Other factors | Strenuous exercise raises it | Level rises linearly with BMI; more dependent on vitamin B6 |
Because ALT is liver-specific and entirely cytoplasmic, it reflects hepatocyte membrane damage well. AST, with its mitochondrial pool and multi-organ distribution, rises disproportionately when there is mitochondrial injury (alcohol, ischemia) or extrahepatic muscle damage.
Normal Reference Point
In most liver diseases: ALT > AST (ratio <1)
This is the baseline expectation. When you see AST exceeding ALT, something specific is happening. The key thresholds are:
| Ratio | Interpretation |
|---|---|
| <1 (ALT>AST) | Most viral hepatitis, NAFLD/MASLD, drug-induced (non-alcohol), mild elevations |
| >1 (AST>ALT) | Raising suspicion - cirrhosis developing, muscle disease, thyroid disease |
| ≥2:1 | Strongly suggestive of alcoholic liver disease; also seen in cirrhosis, Wilson disease |
| ≥3:1 | Characteristic of alcoholic hepatitis specifically |
| >3:1 (acute, then falls to 1:1) | Acute rhabdomyolysis (AST half-life is shorter - normalizes faster) |
Clinical Scenarios in Detail
1. AST:ALT ≥ 2:1 - Alcoholic Liver Disease
The ratio is >2:1 in 70-80% of patients with alcoholic liver disease, and >3 is more specific (mean ratio ~2.6 in ALD vs ~0.9 in non-alcoholic causes).
Two mechanisms explain this:
- Vitamin B6 (pyridoxal-5-phosphate) deficiency - ALT is more dependent on B6 as a cofactor than AST. Malnourished alcoholic patients are commonly B6-deficient, selectively suppressing ALT.
- Direct mitochondrial injury by alcohol - Ethanol and acetaldehyde damage mitochondria, releasing the large mitochondrial pool of AST (which makes up ~80% of total cellular AST) into circulation disproportionately.
Important caveat: The ratio is useful but AST is rarely >300-400 U/L in alcoholic hepatitis - if you see AST/ALT in the thousands with a high ratio, think ischemia or acetaminophen, not alcohol.
2. AST:ALT >1 in Cirrhosis (Any Cause)
As cirrhosis develops from chronic viral hepatitis or NAFLD (where ratio was initially <1), the ratio rises above 1. This has been studied specifically in hepatitis C:
- Specificity for cirrhosis: 94-100%
- Sensitivity for cirrhosis: 44-75% (so it misses many cases)
The mechanism is impaired hepatic sinusoidal uptake of AST due to disrupted portal blood flow in cirrhosis - AST accumulates in blood rather than being cleared.
3. AST:ALT >1 in Wilson Disease
Wilson disease is the third classic cause of ratio reversal (alongside alcoholic liver disease and cirrhosis). The mechanism is linked to mitochondrial copper accumulation causing mitochondrial AST release, similar to how alcohol causes it.
Additional clue in Wilson: ALP is often paradoxically low or normal despite significant liver injury - a unique pattern not seen in other diseases.
4. Ratio <1 (ALT > AST) - Viral Hepatitis / NAFLD
In acute viral hepatitis, NAFLD, and most drug-induced liver injury (non-alcoholic), the cytoplasmic ALT predominates because injury is predominantly membrane-mediated rather than mitochondrial. The ratio typically stays below 1.
In chronic hepatitis C specifically, ALT may even be normal at some time points despite elevated AST - so a single measurement can be misleading.
5. Extrahepatic Causes of High AST:ALT Ratio
Not all AST>ALT means liver disease:
| Condition | Ratio Pattern | Key Distinguishing Feature |
|---|---|---|
| Rhabdomyolysis (acute) | Initially >3:1, falls to ~1:1 rapidly | AST half-life shorter than ALT, so ratio normalizes quickly; CK markedly elevated |
| Chronic myopathy | Close to 1:1 | Check CK, aldolase |
| Macro-AST | AST persistently elevated, no disease | Rare - AST bound to immunoglobulin, prolonged half-life; no clinical consequence |
| Hypothyroidism | AST mildly elevated (often AST>ALT) | TSH elevated; resolves with thyroid replacement |
| Acute MI | AST elevated (cardiac source), ALT spared | Troponin markedly elevated; LDH1 > LDH2 (flipped ratio) |
Time Course Matters: A Critical Point
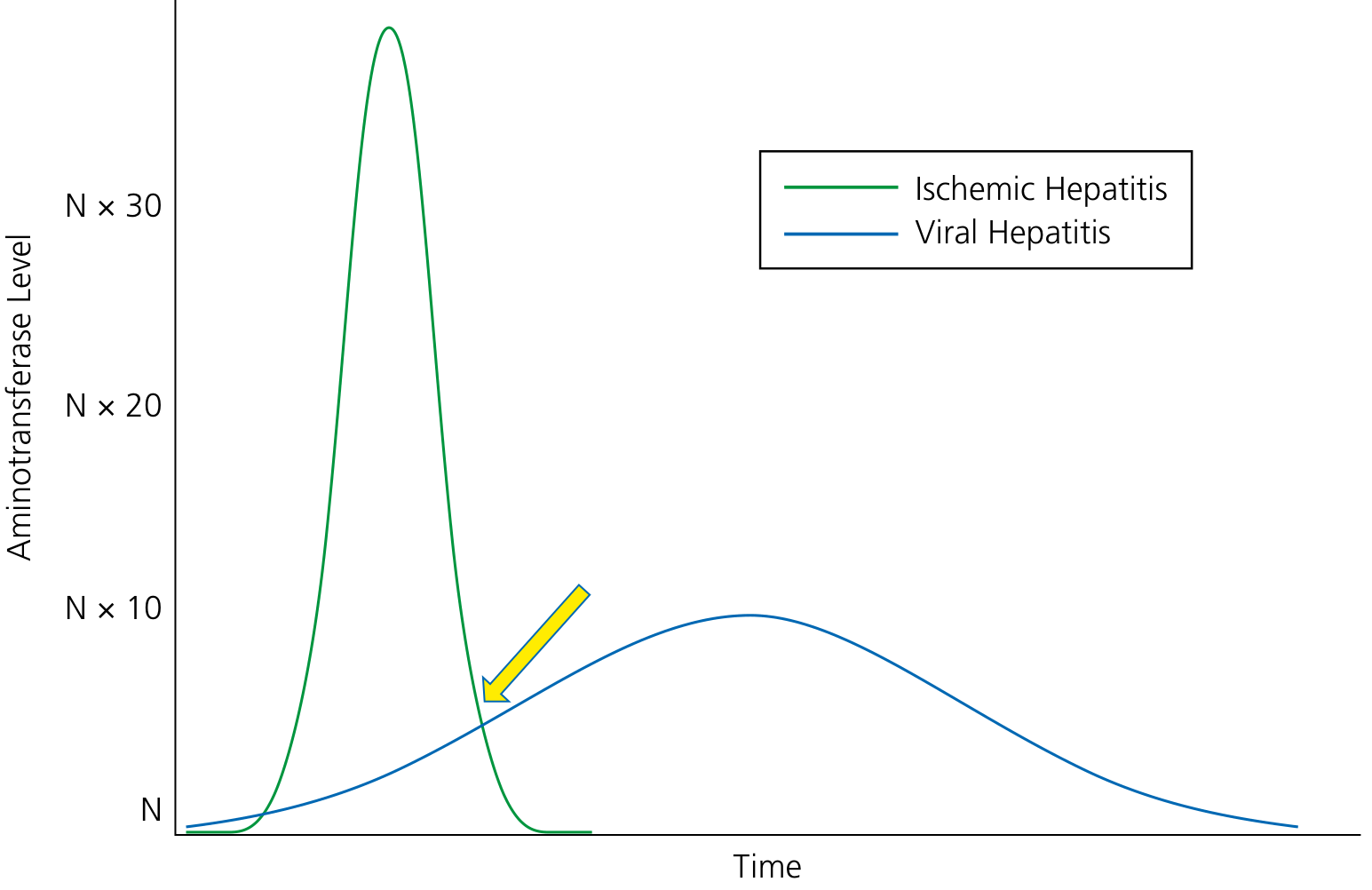
As shown above, a single snapshot can be misleading. Ischemic hepatitis produces a dramatically sharp spike (>30× normal) that falls rapidly, while viral hepatitis rises more gradually. Two patients checked at the yellow arrow point would have identical aminotransferase levels but completely different diagnoses - trending over time is essential.
Practical Algorithm: When You See an Abnormal Ratio
AST:ALT ratio abnormal
|
├── Ratio >2:1
│ ├── Alcohol history? → Alcoholic hepatitis/ALD (confirm with GGT, MCV, CDT)
│ ├── No alcohol + young patient? → Consider Wilson disease (check ceruloplasmin, ALP often low)
│ └── Background chronic liver disease? → Cirrhosis (high specificity, check imaging/fibroscan)
│
├── Ratio >1 but <2
│ ├── Muscle involvement? → Check CK, aldolase
│ ├── Cardiac? → Troponin, ECG
│ ├── Thyroid? → TSH
│ └── Early cirrhosis? → Reassess if chronic liver disease known
│
└── Ratio <1 (ALT>AST) - expected pattern
├── Acute viral hepatitis
├── NAFLD/MASLD
├── Drug-induced (non-alcoholic)
└── Autoimmune hepatitis
Limitations to Remember
- The ratio alone cannot diagnose ALD - must be interpreted with history, GGT, CDT (carbohydrate-deficient transferrin), MCV
- Absolute levels matter too - very high ratios with low absolute values (e.g. AST 60, ALT 20) are less meaningful than moderate ratios with high values
- Hemolysis falsely elevates AST (AST is present in RBCs) without affecting ALT
- Strenuous exercise can elevate AST alone, creating a false high ratio
- The ratio does not reflect disease severity - it only suggests etiology
Sources: Quick Compendium of Clinical Pathology 5th Ed. | Yamada's Textbook of Gastroenterology 7th Ed. | Sleisenger & Fordtran's GI and Liver Disease | Henry's Clinical Diagnosis and Management by Laboratory Methods | Kaplan & Sadock's Comprehensive Textbook of Psychiatry
This is a shared conversation. Sign in to Orris to start your own chat.