Post acne scarrring and hyperpigmentatio
Reading File
Finding Sources
Searching PubMed
"acne scars" AND "treatment"
Searching the Web
post acne scarring hyperpigmentation treatment 2025 guidelines
Finding Sources
Finding Sources
Reading Web Page
https://www.frontiersin.org/journals/medicine/articles/10.33…
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Here is a comprehensive clinical overview of post-acne scarring and hyperpigmentation.
Post-Acne Scarring and Hyperpigmentation
Overview
Almost every acne lesion leaves some transient mark after resolution. In darker skin types (Fitzpatrick IV-VI), post-inflammatory hyperpigmentation (PIH) may persist for months after active lesions clear. In some individuals, permanent structural scarring develops. Both sequelae are distinct entities requiring different management strategies.
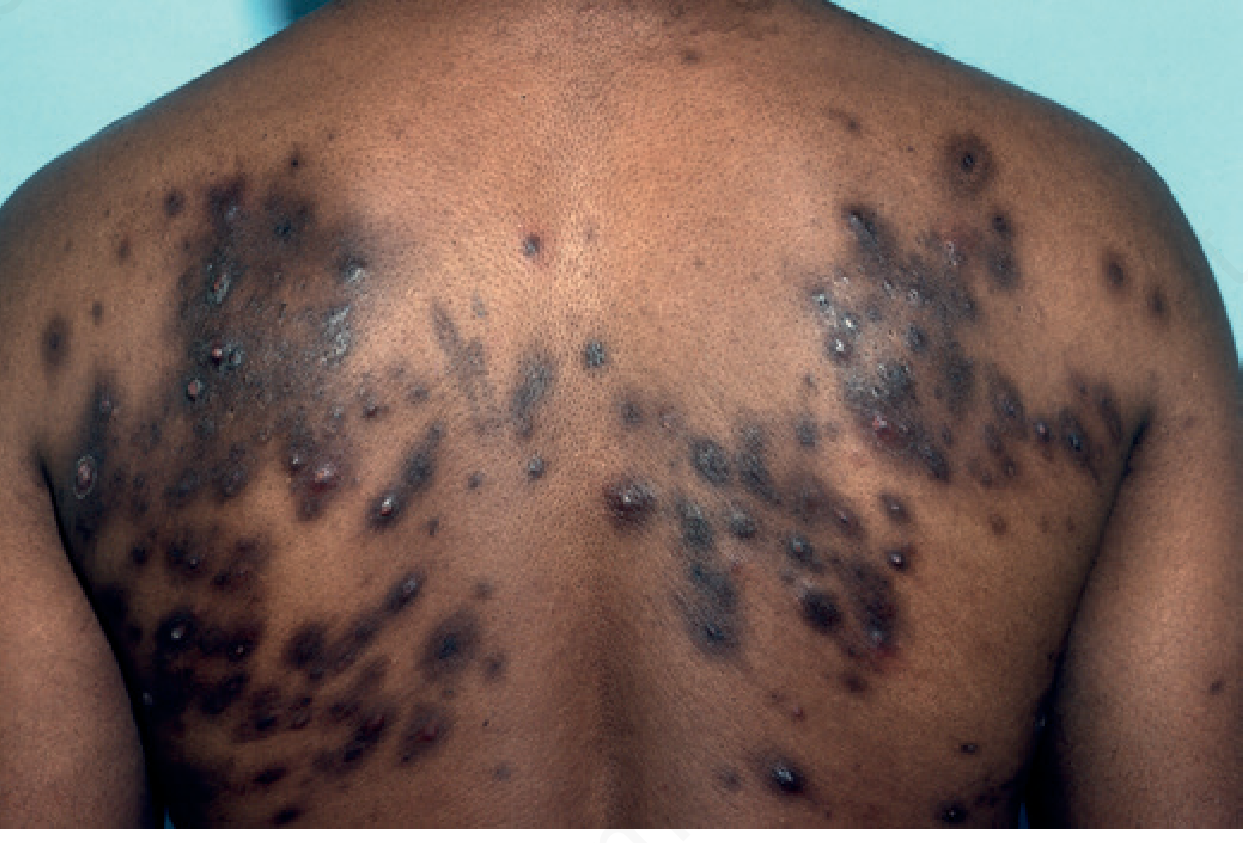
Severe truncal acne with prominent hyperpigmentation - Andrews' Diseases of the Skin
Part 1: Post-Inflammatory Hyperpigmentation (PIH)
Pathophysiology
PIH arises through two distinct mechanisms (Andrews' Diseases of the Skin):
- Epidermal hyperpigmentation - increased melanocyte activity producing excess melanin in the epidermis (responds better to treatment)
- Dermal melanosis - melanin "dropout" from the epidermis into the dermis, where it is taken up by melanophages (much harder to treat, may last years)
Wood's lamp examination distinguishes these: epidermal pigment is accentuated under UV light; dermal melanin is not.
PIH is more common and more persistent in Fitzpatrick skin types IV, V, and VI. It is also more likely after laser procedures done in premenstrual women.
Natural History
PIH will often resolve on its own once the underlying acne is controlled and no new lesions are forming. The key driver of persistence is ongoing active acne producing new lesions in areas that have normalized.
Topical Treatment of PIH
| Agent | Mechanism | Notes |
|---|---|---|
| Hydroquinone (HQ) | Inhibits tyrosinase; degrades melanosomes; generates ROS that destroy melanocytes | OTC: 1.5-2%; Rx: 3-4%. Best for epidermal PIH. Adverse effects: contact dermatitis, ochronosis |
| Tretinoin | Enhances HQ penetration; accelerates epidermal turnover | Potentiates HQ effect when used in combination |
| Kligman's formula | Triple combination: HQ 5% + tretinoin 0.1% + dexamethasone 0.1% | Classic standard for stubborn epidermal hyperpigmentation |
| Tri-Luma cream | HQ 4% + tretinoin 0.05% + fluocinolone 0.01% | Prescription only; OTC HQ 2% has modest effect |
| Azelaic acid | Tyrosinase inhibitor; also has comedolytic, antimicrobial, anti-inflammatory properties | Particularly useful in acne-PIH given multi-tasking profile |
| Tranexamic acid | Inhibits plasminogen activation; mitigates UV-induced melanogenesis | Topical 2-5%, intradermal 4 mg/mL, or oral 250-325 mg BID (off-label for PIH/melasma) |
| Glycolic acid peels | Adjunctive; accelerate epidermal turnover | Best as add-on to topical regimen in refractory epidermal PIH |
| Sunscreen/photoprotection | Blocks UV-driven melanogenesis | Non-negotiable component of any PIH regimen |
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics; Andrews' Diseases of the Skin
Important caveat: Topical depigmenting agents have limited efficacy on dermal PIH. Laser treatments and chemical peels for PIH must be performed with caution in darker skin types - results are unpredictable and worsening of pigmentation is a real risk.
Part 2: Post-Acne Scarring
Classification of Acne Scars
Acne scars are either atrophic (by far the most common) or hypertrophic/keloidal. Atrophic scars are classified by morphology (Fitzpatrick's Dermatology):
| Scar Type | Description | Size | Treatment Implications |
|---|---|---|---|
| Ice pick | Narrow, deep, V-shaped; tapers to a point in dermis | <2 mm | Hard to treat; TCA CROSS technique, punch excision |
| Boxcar | Wide, sharply demarcated, flat base; does not taper | 1.5-4 mm | Fractional laser, subscision, TCA CROSS |
| Rolling | Shallow, wide, undulating appearance | >4-5 mm | Subcision works well; fractional laser |
| Perifollicular elastolysis | Soft atrophic papules, upper trunk | Varies | Less studied |
| Hypertrophic/keloid | Raised firm scar; keloids extend beyond original lesion | Varies | Intralesional corticosteroids, fluorouracil, pressure, laser |
Treatment of Acne Scars
Multiple modalities exist. Combination approaches tailored to scar morphology outperform any single treatment.
Chemical Peels
- Superficial peels (salicylic acid, Jessner's solution, glycolic acid): for superficial scars and concurrent PIH
- Medium-depth peels (TCA 30-40%): penetrate to papillary dermis; effective for medium-depth boxcar and rolling scars
- TCA CROSS technique (70% TCA focal application): highly effective for ice pick and deep boxcar scars
- Deep peels (phenol, TCA 50%): reticular dermis; higher complication risk including PIH
Energy-Based Devices
| Device | Mechanism | Best For | Skin Type Caution |
|---|---|---|---|
| Ablative fractional CO2 | Micro-ablative columns; ~90% efficacy | Deep atrophic scars | High PIH risk in Fitzpatrick III-VI |
| Er:YAG laser | More superficial ablation, faster healing | Moderate scars | Somewhat safer in darker skin vs CO2 |
| Non-ablative fractional (1550 nm) | Thermal zones without surface ablation | Mild-moderate scars | Lower PIH risk |
| Picosecond lasers | Ultrashort pulses; laser-induced optical breakdown | Pigmentary disorders, scar revision | Reduced PIH risk vs fractional CO2; 75% show significant scar volume reduction |
| Radiofrequency microneedling (RFMN) | RF energy delivered via microneedles | Atrophic scars | Lower PIH risk; good for all skin types |
A 2026 meta-analysis (PMID 41821146) found fractional CO2 laser and microneedling radiofrequency are comparably effective for post-acne scarring, with no significant difference in outcomes between RCTs.
Microneedling (Transcutaneous Collagen Induction)
Microneedling modulates local gene expression and promotes collagen synthesis. Compared to fractional lasers, it requires longer treatment intervals but has a significantly lower incidence of post-procedural hyperpigmentation - or none at all - in Fitzpatrick IV-VI skin types. This makes it preferred in darker-skinned patients (Frontiers in Medicine, Zhang et al. 2025).
Surgical and Injectable Approaches
- Subcision: Needle inserted under scar to release fibrous tethering bands; particularly effective for rolling scars
- Punch excision/grafting: For ice pick scars; followed by dermabrasion or laser smoothing
- Dermal fillers (hyaluronic acid, PLLA, etc.): Volume restoration under depressed scars; temporary to semi-permanent
- Fat transfer: Autologous option for broader atrophic areas
- Intralesional corticosteroids (triamcinolone 2.5 mg/mL or diluted): For hypertrophic scars and keloids; inject <0.1 mL directly into center to avoid atrophy/hypopigmentation
- Intralesional fluorouracil: Alternative or adjunct to steroids for hypertrophic scars
Key Clinical Principles
- Control active acne first - treating scars while acne remains active is futile; new lesions replace healed areas
- Skin type drives modality selection - ablative lasers carry high PIH risk in darker skin (Fitzpatrick III-VI); prefer microneedling, RFMN, or non-ablative approaches
- Combination therapy outperforms monotherapy - e.g., subcision + fractional laser + topical retinoid
- PIH vs. true scar - PIH is a flat discoloration that will fade; true scars involve structural tissue changes and need procedural intervention
- Sun protection is mandatory - UV exposure perpetuates melanogenesis; SPF 30+ daily is non-negotiable in any PIH/scar regimen
- Isotretinoin timing - the EuroGuiDerm 2025 guideline now recommends that superficial procedural treatments can begin earlier than the traditionally cited 6-month post-isotretinoin window, with informed consent
Recent Evidence (2024-2026)
- A 2024 network meta-analysis (PMID 39110247) confirms microneedling combined with adjunctive treatments (PRP, vitamin C) outperforms microneedling alone for acne scars
- A 2025 systematic review (PMID 40515775) demonstrates comparable efficacy of ablative vs. non-ablative lasers overall, but non-ablative devices have a better safety profile in darker skin
- Er:Glass vs. CO2 lasers for atrophic acne scars: a 2026 meta-analysis (PMID 41364211) found both are effective; Er:Glass may have fewer side effects
- Picosecond lasers show comparable efficacy to fractional CO2 with reduced PIH risk, making them an emerging preferred option in phototype III-VI patients
Sources: Andrews' Diseases of the Skin (9780323547536); Fitzpatrick's Dermatology (9780071837781); Goodman & Gilman's Pharmacological Basis of Therapeutics (9781264258079); Zhang et al., Frontiers in Medicine 2025; EuroGuiDerm Acne Guideline Update 2025.
Is kojic acid good for PIH
Finding Sources
Searching PubMed
"kojic acid" AND "hyperpigmentation"
Reading File
Reading Article
PMID: 38433524
Finding Sources
Searching the Web
kojic acid post inflammatory hyperpigmentation efficacy evidence 2024 2025
Reading File
Yes - kojic acid is a useful agent for PIH, but with some important nuances. Here is a clear breakdown:
Kojic Acid for PIH
How It Works
Kojic acid is a fungal metabolite (from species of Aspergillus, Acetobacter, and Penicillium) that depigments skin by chelating the copper ion at the active site of tyrosinase, directly blocking melanin synthesis. This is a distinct mechanism from hydroquinone (which inhibits tyrosinase indirectly and destroys melanosomes) - though the end result is similar.
It is listed in Fitzpatrick's Dermatology's official table of lightening agents alongside hydroquinone, retinoids, azelaic acid, arbutin, and tranexamic acid.
Is It Effective?
Short answer: yes, particularly for epidermal PIH - but the evidence base is more robust for melasma than for PIH specifically.
| What the evidence says | Detail |
|---|---|
| Efficacy confirmed for melasma | Multiple RCTs in Caucasian and Asian patients show 2% KA + hydroquinone combination improves melasma effectively |
| PIH-specific data is limited | Direct RCTs specifically for post-acne PIH are sparse; evidence is largely extrapolated from melasma and general hyperpigmentation studies |
| Combination > monotherapy | KA combined with glycolic acid, hydroquinone, or niacinamide outperforms KA alone |
| 2025 RCT data | A split-face pilot RCT (Tantanasrigul et al., 2025) found 5% alpha-arbutin + 2% KA cream comparable to triple combination cream (HQ + tretinoin + steroid) for melasma, with lower recurrence (p = 0.004) |
| 2024 Bayesian network meta-analysis (PMID 38433524) | Ranked 14 depigmenting agents - hydroquinone 4% ranked 2nd overall at the late timepoint (D40); KA 1% was included as a reference comparator, suggesting it performs but is not the top-tier agent |
Practical Points
- Concentration: 1-4% in topical products. The 2% concentration is most commonly used.
- Use in combination: Most effective when paired with glycolic acid (enhances penetration) or hydroquinone (additive tyrosinase inhibition). Chemical peels containing kojic acid are also used.
- Start early: Mechanistically, KA blocks new melanin synthesis - it works best when started as soon as PIH begins forming, before pigment accumulates significantly.
- Sun protection is mandatory: KA can increase UV sensitivity; without SPF 30+, it partially counteracts itself.
- Stability problem: KA is chemically unstable and oxidizes in formulations, turning yellow-brown. This is a real limitation - product quality and storage matter.
- Side effects: Mildly irritating at 2-4%; contact dermatitis occurs in some users (a notable limitation vs. azelaic acid which is better tolerated) - Pfenninger & Fowler's Procedures for Primary Care
Where It Sits vs. Other Agents
| Agent | Strength for PIH | Key Advantage |
|---|---|---|
| Hydroquinone 4% | Strongest evidence, gold standard | Best head-to-head data |
| Kojic acid 2% | Good; best used in combination | Natural origin, HQ-free option |
| Azelaic acid 15-20% | Good; RCT shows efficacy for post-acne PIH | Also treats active acne, better tolerated |
| Tretinoin | Moderate alone; potentiates others | Accelerates epidermal turnover |
| Tranexamic acid | Emerging strong data | Also works on dermal component |
| Niacinamide | Mild; good tolerability | OTC, very safe |
Bottom Line
Kojic acid is a legitimate and useful option for PIH, especially as part of a combination regimen or as an alternative for patients who cannot tolerate hydroquinone. The main caveats are: the direct PIH evidence lags behind melasma evidence, it works best on epidermal (not dermal) pigment, formulation instability is a real-world issue, and contact sensitization occurs in a subset of patients. For post-acne PIH in particular, combining it with a retinoid and glycolic acid - plus strict sun protection - gives the best results.
This is a shared conversation. Sign in to Orris to start your own chat.