Why is there increased alp in hypocalcemia
Reading File
Finding Sources
Finding Sources
Searching PubMed
alkaline phosphatase hypocalcemia hyperparathyroidism mechanism
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
I now have solid textbook evidence. Here is the complete, well-sourced answer:
Why Is ALP Elevated in Hypocalcemia?
The relationship between elevated alkaline phosphatase (ALP) and hypocalcemia is not direct - rather, ALP rises because of the underlying causes and compensatory mechanisms triggered by low calcium. There are two main pathways:
1. Secondary Hyperparathyroidism - The Central Mechanism
When serum calcium falls (from any cause), the parathyroid glands respond by secreting more PTH - this is secondary hyperparathyroidism (SHPT). PTH then:
- Stimulates osteoblasts directly, causing them to proliferate and become more active
- Osteoblasts are the primary source of bone-specific ALP - they use it to generate inorganic phosphate for hydroxyapatite mineralization
- Over time, sustained PTH also activates osteoclasts (via RANKL from osteoblasts), increasing overall bone turnover
- The net result is markedly elevated ALP as a marker of high bone formation/remodeling activity
"PTH stimulates osteoblast activity, and therefore PINP, osteocalcin, and other markers of bone formation increase rapidly... Activation of osteoblasts over time results in RANKL production, which stimulates osteoclast activity."
- Firestein & Kelley's Textbook of Rheumatology
2. The Underlying Disease Drives ALP Directly
The cause of hypocalcemia matters - and in most common causes, ALP is elevated for additional reasons:
| Cause of Hypocalcemia | Why ALP is Elevated |
|---|---|
| Vitamin D deficiency / Osteomalacia | Impaired bone mineralization triggers osteoblast overactivity; ALP accumulates because the enzyme cannot complete its function in unmineralized osteoid |
| Chronic Renal Failure (CKD-MBD) | Both impaired vitamin D activation AND secondary hyperparathyroidism drive osteoblast stimulation simultaneously |
| Rickets (children) | Defective mineralization at growth plates with massive osteoblast proliferation |
"In vitamin D deficiency osteomalacia, serum calcium and phosphate are low, alkaline phosphatase and PTH are elevated, renal function is normal, and 25-OH-D3 is low." - Goldman-Cecil Medicine
"In chronic renal failure, which is the most common cause of hypocalcemia, phosphate is high; alkaline phosphatase, creatinine, and PTH are elevated." - Goldman-Cecil Medicine
"Increased serum alkaline phosphatase activity is classically associated with osteomalacia due to vitamin D deficiency." - Goldman-Cecil Medicine
Important Exception: Hypoparathyroidism
In hypoparathyroidism (low PTH is the cause of low calcium), ALP is typically normal. This is because there is no secondary hyperparathyroidism driving bone turnover. Goldman-Cecil notes that in hypoparathyroidism, "alkaline phosphatase activity is normal." This contrast is diagnostically useful - a normal ALP with hypocalcemia points toward hypoparathyroidism rather than vitamin D deficiency or CKD.
Similarly, in the rare condition hypophosphatasia, ALP is paradoxically low despite hypocalcemia, because the defect is in the ALP enzyme itself.
Summary
The pathway is:
Low Ca²+ → ↑ PTH (secondary hyperparathyroidism) → ↑ Osteoblast activity → ↑ Bone-specific ALP released into circulation
Combined with the direct effect of the underlying disease (vitamin D deficiency, CKD) further stimulating bone remodeling, ALP rises as a marker of high bone turnover. The clinical pattern of hypocalcemia + high ALP + high PTH is the classic fingerprint of vitamin D deficiency osteomalacia or renal osteodystrophy.
What is the mechanism of ALP reduction by bisphosphonates?
Finding Sources
Finding Sources
Searching PubMed
bisphosphonate mechanism osteoclast bone remodeling ALP
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Excellent - I have everything needed. Here is the complete answer:
Mechanism of ALP Reduction by Bisphosphonates
This is a two-step process: bisphosphonates first target osteoclasts at the molecular level, and ALP falls as a downstream consequence of reduced bone turnover.
Step 1 - Direct Molecular Target: The Mevalonate Pathway (Nitrogen-Containing Bisphosphonates)
Potent nitrogen-containing bisphosphonates (alendronate, risedronate, ibandronate, pamidronate, zoledronate) are selectively taken up by osteoclasts and inhibit the enzyme farnesyl pyrophosphate synthase (FPPS) in the mevalonate pathway:
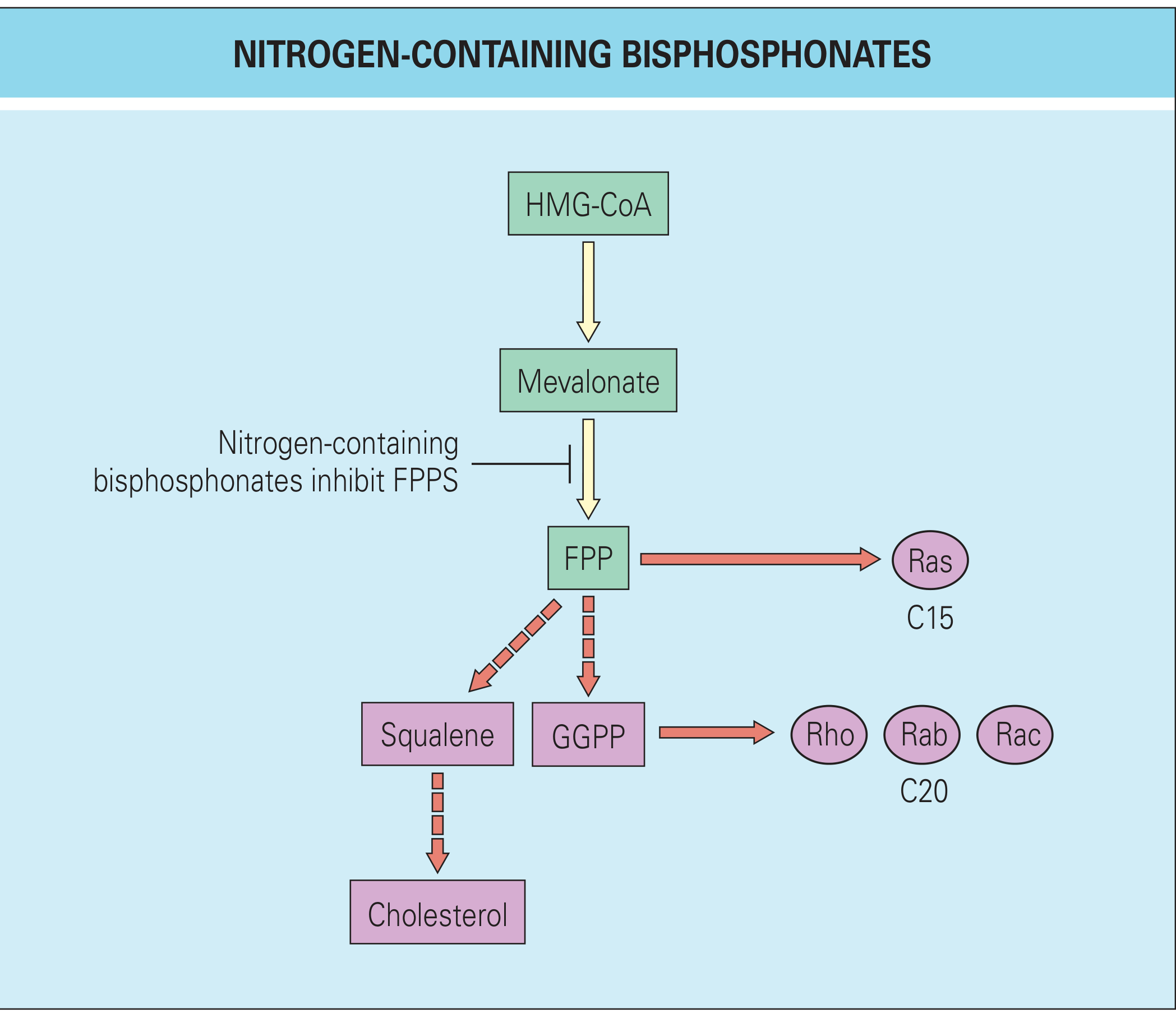
The cascade:
- FPPS inhibition blocks conversion of mevalonate to farnesyl pyrophosphate (FPP) and geranylgeranyl pyrophosphate (GGPP)
- FPP and GGPP are the lipid anchors required for protein prenylation - the attachment of isoprenoid groups to small GTPases (Ras, Rho, Rab, Rac)
- Without prenylation, these GTPases cannot attach to cell membranes
- Loss of membrane-bound GTPases disrupts critical osteoclast functions:
- Osteoclast recruitment and differentiation
- Formation of the ruffled border (the resorption organelle)
- Acid and protease secretion into the resorption lacuna
- Triggers osteoclast apoptosis
"Nitrogen-containing bisphosphonates interfere with the mevalonate pathway by inhibiting the enzyme farnesyl pyrophosphate. This prevents protein prenylation and the attachment of a lipid anchor in the membrane, which disrupts signaling pathways in osteoclasts and inhibits osteoclast recruitment, differentiation, formation of the ruffled border, and acid production, and induces apoptosis." - Rheumatology (Elsevier, 2022)
Non-nitrogen bisphosphonates (etidronate, clodronate) work differently - they are incorporated into non-hydrolyzable ATP analogues that accumulate and are directly toxic to osteoclasts.
Step 2 - ALP Falls via Bone Remodeling Coupling
ALP (bone-specific isoform) is produced by osteoblasts, not osteoclasts. So why does inhibiting osteoclasts lower ALP?
Because bone resorption and formation are tightly coupled through the bone remodeling unit (BMU):
Normal remodeling cycle:
Osteoclast resorption → releases TGF-β, IGF-1, BMP from matrix
↓
Signals recruit and activate osteoblasts (coupling factors)
↓
Osteoblasts form new bone → release ALP into circulation
When bisphosphonates suppress osteoclasts:
- Resorption decreases within 1-2 months
- Coupling factors (TGF-β, IGF, BMPs) released from resorbed matrix fall
- Osteoblast recruitment and activity fall in parallel
- ALP (a bone formation marker) decreases as osteoblast activity decreases
"The decrease in bone resorption with bisphosphonate therapy occurs in the first 1 to 2 months of treatment. Because of the coupling of formation and resorption, inhibition of resorption results in a decrease in bone formation over time." - Rheumatology (Elsevier, 2022)
This is also why, in a study of alendronate, patients with >30% reduction in bone ALP had the greatest reduction in vertebral and non-vertebral fracture risk - ALP drop is a direct surrogate for successful remodeling suppression (Firestein & Kelley's Textbook of Rheumatology).
Clinical Context: ALP as a Monitoring Tool
- In Paget's disease of bone, bisphosphonates are specifically used to normalize the markedly elevated ALP, and treatment response is tracked by ALP normalization
- In osteoporosis, a fall in ALP (and other bone turnover markers like PINP) within 3-6 months confirms adequate drug response
- The transient bone pain/flu-like reaction after IV bisphosphonates (especially zoledronate) can cause a brief spike in ALP before suppression occurs
Summary
| Step | Event |
|---|---|
| Bisphosphonate binds bone → taken up by osteoclasts | FPPS enzyme inhibited in mevalonate pathway |
| FPP/GGPP depleted | Small GTPases (Ras, Rho, Rab, Rac) lose prenylation |
| GTPases cannot anchor to membrane | Ruffled border lost, acid secretion fails, apoptosis triggered |
| Osteoclast activity suppressed | Coupling factors from resorbed matrix fall |
| Osteoblast recruitment reduced | Less bone-ALP released into circulation |
| Net result | Serum ALP falls |
This is a shared conversation. Sign in to Orris to start your own chat.