Capnography
Reading File
Finding Sources
Searching PubMed
capnography clinical monitoring
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
I now have comprehensive material to write a thorough, well-illustrated response. Let me compose the full answer.
Capnography
Capnography is the continuous, non-invasive measurement and graphical display of carbon dioxide (CO2) concentration in exhaled gas, breath by breath. The numeric value at the end of exhalation is called the end-tidal CO2 (ETCO2 or PetCO2). The graphical waveform is the capnogram.
1. Physiological Basis
CO2 is produced by cellular metabolism, transported via venous blood to the lungs, diffuses rapidly across the alveolar membrane, and is expelled during exhalation. Because CO2 diffuses so readily, alveolar PCO2 (PACO2) essentially equals arterial PCO2 (PaCO2). End-tidal CO2 measured from exhaled gas is therefore a close surrogate for PaCO2.
Normal PaCO2 - PetCO2 gradient: < 5 mm Hg
This small gradient exists because end-tidal gas is slightly diluted by CO2-free gas from non-perfused alveoli (alveolar dead space). The gradient widens in conditions of:
- Increased alveolar dead space (pulmonary embolism, low cardiac output, pulmonary hypertension)
- Pulmonary overdistension
- Obstructive airway disease (air trapping, incomplete exhalation)
Normal PetCO2: 35-45 mm Hg (mirrors normal PaCO2 of 35-45 mm Hg)
- Morgan and Mikhail's Clinical Anesthesiology, 7e
- Miller's Anesthesia, 10e
2. Technology: How It Works
Measurement Methods
| Method | Description | Advantage | Disadvantage |
|---|---|---|---|
| Mainstream (non-aspirating) | Infrared sensor placed directly in-line with the airway circuit | No sampling delay; accurate | Heavier sensor on airway; requires intubation or tight mask |
| Sidestream (aspirating) | Small pump aspirates a continuous gas sample from the circuit or cannula | Can be used in non-intubated patients via nasal cannula | Slight time delay; risk of water condensation/blockage |
| Colorimetric | pH-sensitive dye changes color (purple→yellow) with CO2 | Cheap, no power needed; rapid ETT confirmation | Qualitative only; false positives from carbonated beverages or gastric acid |
Display Types
- Time-based capnography: CO2 concentration vs. time (most common)
- Volumetric capnography: CO2 concentration vs. exhaled volume - enables direct dead space calculations and can guide PEEP titration and assess bronchodilator response
3. The Normal Capnogram Waveform
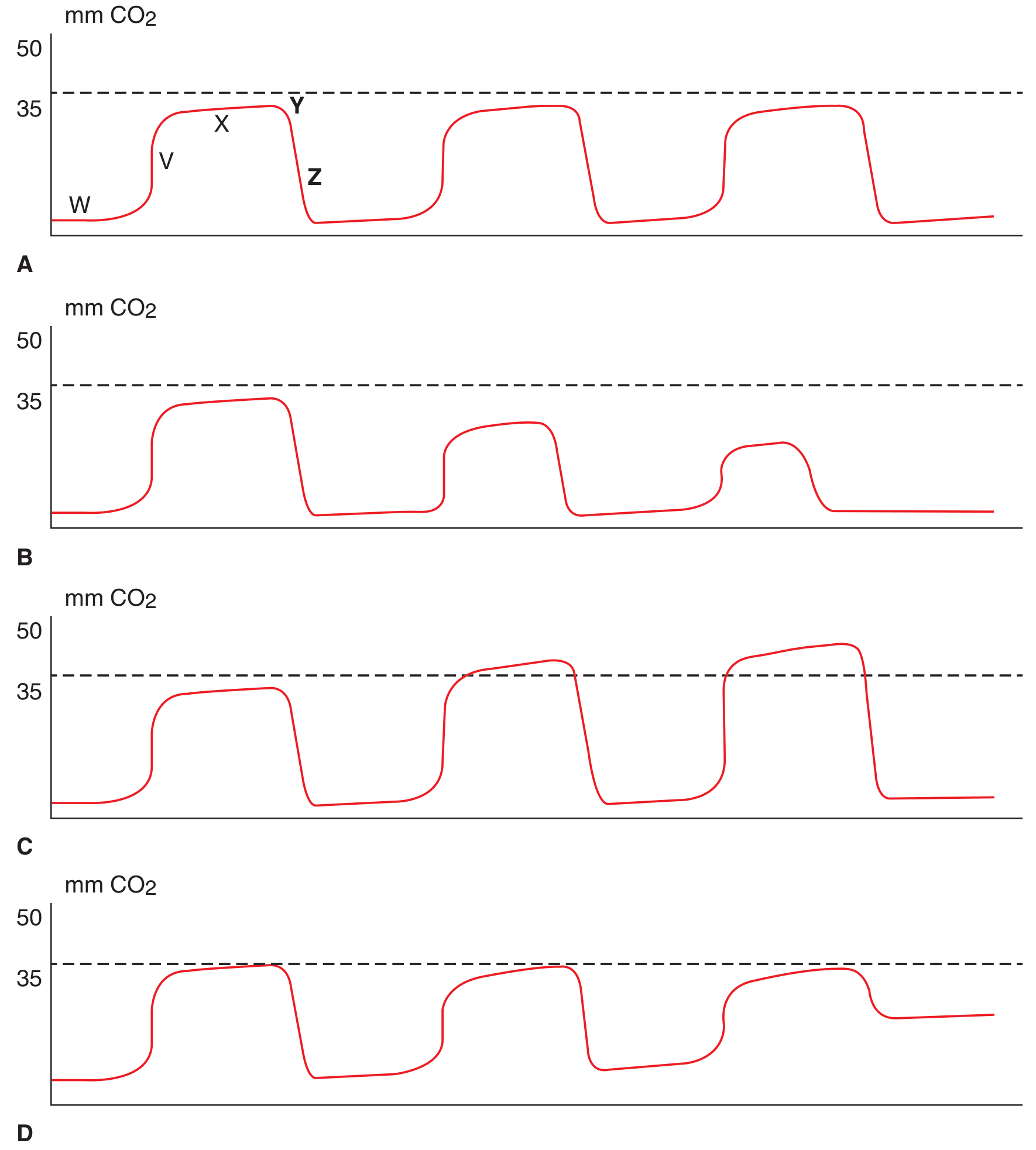
Capnogram A: Normal. B: Apnea (serially decreasing amplitudes). C: Hypoventilation (rising plateau). D: Rebreathing/air trapping (elevated baseline).
The normal capnogram has 5 phases:
| Phase | Label | Description |
|---|---|---|
| Inspiratory baseline | W | CO2 = 0 (fresh gas inhaled) |
| Expiratory upstroke | V | Dead space gas clearing; rapid CO2 rise |
| Expiratory plateau (alveolar plateau) | X | Alveolar gas; CO2 levels out |
| End-tidal point | Y | Peak CO2 at end of exhalation = PetCO2 |
| Inspiratory downstroke | Z | Rapid fall back to zero as fresh gas enters |
A rising upslope or "shark fin" shape to the exhalation phase indicates obstructive airway disease (asthma, COPD) - incomplete, uneven emptying of alveoli.
- Tintinalli's Emergency Medicine, p. 122
4. Abnormal Capnogram Patterns
| Pattern | Appearance | Clinical Cause |
|---|---|---|
| Apnea | Flat line at zero | Apnea, esophageal intubation, circuit disconnection |
| Hypoventilation | Rising plateau and rising PetCO2 | Opioid effect, CNS depression, sedation |
| Hyperventilation | Falling PetCO2 | Anxiety, pain, mechanical over-ventilation |
| Elevated baseline | Baseline does not return to zero | CO2 rebreathing, exhausted soda lime, stuck inspiratory valve |
| Shark fin / prolonged upstroke | No plateau; slowly sloping expiration | Bronchospasm, COPD, kinked ETT |
| Sudden drop to zero | Waveform disappears | ETT dislodgement, circuit disconnect, cardiac arrest |
| Sudden decrease (not zero) | PetCO2 falls abruptly | Pulmonary embolism (sudden dead space increase), cardiac arrest |
| Gradual decline | Slow decrease over time | Hyperventilation, hypothermia, decreasing cardiac output |
| Sudden rise | Acute CO2 increase | Tourniquet release, sodium bicarbonate administration, malignant hyperthermia |
Alveolar dead space fraction (AVDSf):
AVDSf = (PaCO2 - PetCO2) / PaCO2
Elevated AVDSf correlates with severity of acute hypoxemic respiratory failure and mortality in pediatric patients. - Miller's Anesthesia, 10e
5. Clinical Applications
5a. Endotracheal Tube (ETT) Confirmation
Continuous waveform capnography is the gold standard for confirming endotracheal - not esophageal - intubation. A sustained, consistent waveform across multiple breaths confirms tracheal placement.
- Colorimetric detectors are adequate but can give false positives after carbonated beverages or gastric acid contamination.
- Waveform capnography is superior to colorimetric devices and is the preferred method.
- Tintinalli's Emergency Medicine; Barash's Clinical Anesthesia, 9e
5b. Procedural Sedation and Analgesia (PSA)
Capnography detects hypoventilation and apnea before pulse oximetry, especially when supplemental oxygen is being given (which delays oxyhemoglobin desaturation).
Key evidence:
- Respiratory depression was 17.6x more likely to be detected with capnography vs. standard monitoring alone (meta-analysis by Waugh et al.)
- 100% of apneic episodes >20 seconds during MAC were missed by providers but caught by capnography (Soto et al.)
- Pulse oximetry detected only ~50% of apnea/disordered breathing episodes detected by capnography during upper endoscopy - hypoxemia followed apnea by an average of 45.6 seconds
ACEP gives capnography a Level B recommendation as an adjunct during PSA in the ED. - Roberts & Hedges' Clinical Procedures in Emergency Medicine; Barash's Clinical Anesthesia, 9e
5c. Cardiac Arrest / CPR Monitoring
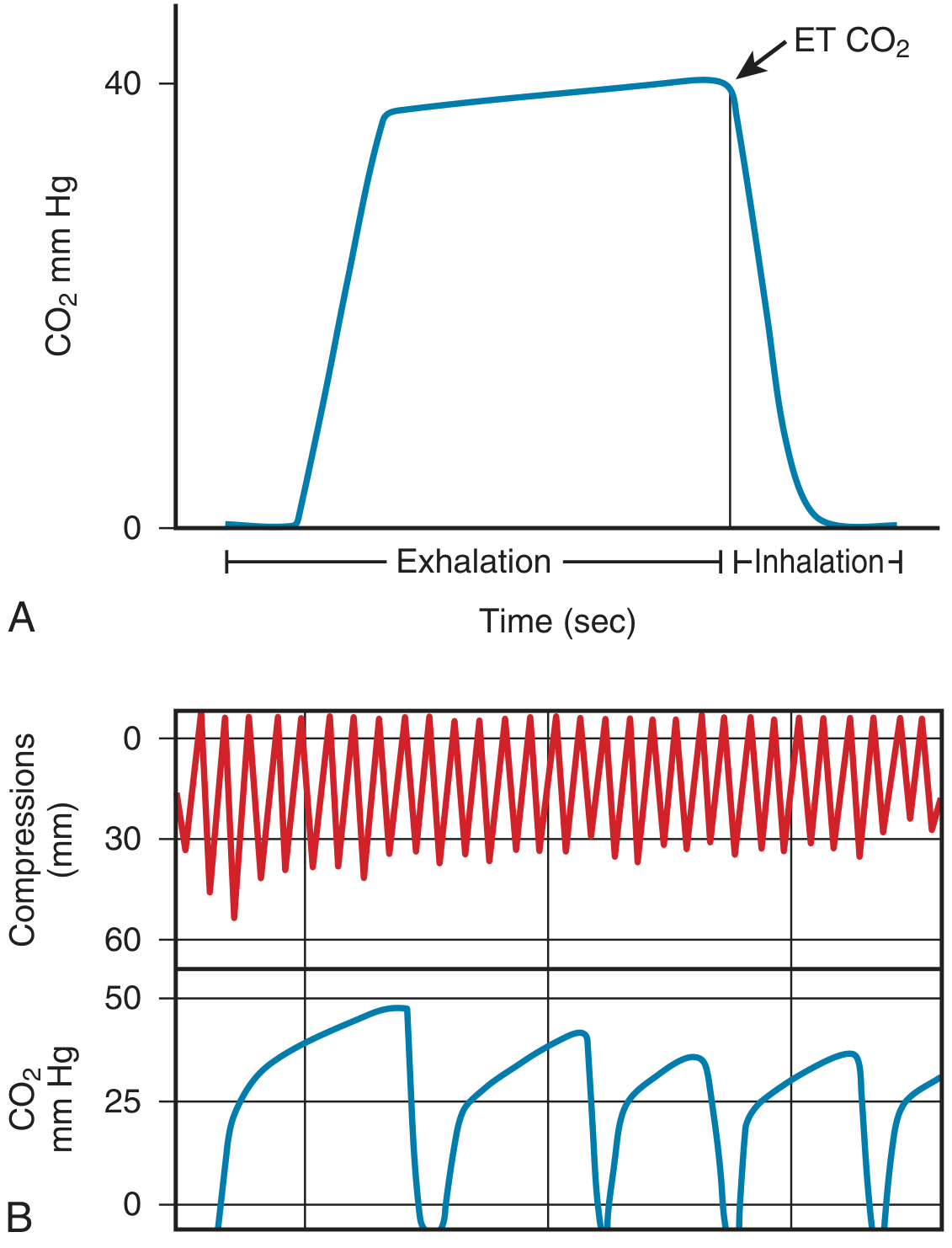
Panel A: Normal single-breath waveform. Panel B: PETCO2 during CPR - note the declining trend over time reflecting CPR fatigue.
During cardiac arrest, PetCO2 correlates with cardiac output under low-flow states:
- At arrest onset: PetCO2 falls abruptly (no pulmonary perfusion)
- During effective CPR: PetCO2 rises as compressions generate forward flow; correlates with coronary perfusion pressure and compression efficacy
- At ROSC: Sudden, sustained rise in PetCO2 to physiologic levels (often the earliest sign of ROSC)
- For termination of resuscitation: A persistently low PetCO2 after 20 minutes of ACLS may support decision to terminate efforts
The 2015 (and current) resuscitation guidelines recommend continuous waveform capnography for all intubated patients during CPR. - Roberts & Hedges' Clinical Procedures in Emergency Medicine
5d. Monitoring Ventilation Adequacy
- Continuous non-invasive estimation of PaCO2 during mechanical ventilation
- Detects inadvertent hyperventilation or hypoventilation
- In patients receiving supplemental oxygen, SpO2 may remain normal despite significant hypoventilation - capnography reveals this early
5e. Pulmonary Embolism
- Acute PE causes sudden dead space increase → abrupt fall in PetCO2 (widened a-ET gradient)
- Not diagnostic alone, but clinically useful as an alert signal
5f. Malignant Hyperthermia (MH)
- Early and sensitive indicator - rapidly rising PetCO2 during volatile anesthetic exposure, even before fever or rigidity
- Capnography is specifically recommended as part of MH monitoring protocol
5g. Detecting Rebreathing / Equipment Failure
- Elevated baseline (CO2 does not return to zero) indicates rebreathing from:
- Exhausted CO2 absorber (soda lime)
- Stuck or malfunctioning inspiratory valve
- Insufficient fresh gas flow in circle system
5h. Non-Intubated Patients
Sidestream capnography adapted for:
- Nasal cannulas with integrated sampling port
- Modified face masks with IV catheter sampling lines
- Useful during moderate/deep sedation, sleep studies
6. Limitations
-
PetCO2 underestimates PaCO2 - the gradient widens in obstructive lung disease, pulmonary embolism, low cardiac output, and high dead space states
-
Studies of accuracy vs. ABG are mixed in ED populations - particularly unreliable in undifferentiated dyspnea, COPD exacerbations, and critically ill patients
-
Sidestream sampling is susceptible to water vapor condensation and secretion obstruction
-
Less accurate at high respiratory rates (time-based capnography) due to incomplete alveolar gas sampling
-
Colorimetric detectors are qualitative only and have false-positive/negative risks
-
Tintinalli's Emergency Medicine, p. 122
7. Summary Table: Key Uses
| Application | What to Look For |
|---|---|
| ETT confirmation | Sustained waveform x6 breaths |
| Sedation monitoring | Rising PetCO2 or flat line (apnea) |
| CPR quality | PetCO2 >10-20 mmHg = adequate compressions; rise = ROSC |
| Malignant hyperthermia | Unexplained rising PetCO2 |
| Bronchospasm | Shark fin waveform |
| Rebreathing | Elevated baseline |
| Pulmonary embolism | Sudden drop in PetCO2 |
| Termination of resuscitation | PetCO2 persistently <10 mmHg after 20 min ACLS |
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide (p. 122)
- Roberts and Hedges' Clinical Procedures in Emergency Medicine (Chapters 17, 33)
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e
- Morgan and Mikhail's Clinical Anesthesiology, 7e
- Miller's Anesthesia, 10e
Vaporizers
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive material across Miller's Anesthesia and Barash's Clinical Anesthesia. Let me compile the full answer.
Vaporizers
A vaporizer is a device on the anesthesia machine that converts liquid volatile anesthetic into vapor and delivers it at a precise, clinically useful concentration to the patient's breathing circuit. Because the saturated vapor pressure (SVP) of volatile agents far exceeds clinically safe concentrations, the key engineering challenge is accurate dilution and temperature compensation.
1. Basic Physics
Saturated Vapor Pressure (SVP)
Each volatile agent exerts a characteristic SVP at a given temperature - the maximum partial pressure of vapor that can exist above the liquid. SVP is independent of barometric pressure, but rises with temperature.
| Agent | SVP at 20°C (mm Hg) | Boiling Point (°C) | MAC (%) |
|---|---|---|---|
| Halothane | 244 | 50.2 | 0.75 |
| Isoflurane | 238 | 48.5 | 1.15 |
| Enflurane | 172 | 56.5 | 1.68 |
| Sevoflurane | 160 | 58.5 | 1.85 |
| Desflurane | 669 | 22.8 | 6.0 |
Desflurane's SVP of 669 mm Hg and boiling point of 22.8°C make it nearly unique - it would boil at normal OR temperatures, making a standard variable bypass vaporizer impossible to use for this agent.
Why Dilution Is Needed
Even sevoflurane at 20°C has SVP of ~160 mm Hg - that is 21% concentration at sea level. Clinical sevoflurane is used at 1-3%, so the saturated vapor from the vaporizing chamber must be heavily diluted.
2. Classification of Vaporizers
By Circuit Position
| Type | Description | Use |
|---|---|---|
| Out-of-circuit | Located outside the breathing circuit; precise output added via fresh gas line | Virtually all modern clinical vaporizers |
| In-circuit | Located within the breathing circuit; patient's own breathing draws vapor through | Draw-over systems; resource-limited settings, ICU sedation |
By Operating Principle
- Variable bypass (plenum) vaporizers
- Dual-circuit (heated/pressurized) vaporizers - for desflurane
- Cassette vaporizers (e.g., Aladin)
- Injection vaporizers
3. Variable Bypass Vaporizer (The Standard)
This is the type used for halothane, isoflurane, enflurane, and sevoflurane. Also called a plenum-type vaporizer.
Components
- Fresh gas inlet
- Concentration control dial - sets the splitting ratio
- Bypass chamber - carries the majority of fresh gas that bypasses the liquid agent
- Vaporizing chamber - contains liquid anesthetic + wicks/baffles
- Temperature-compensating device (bimetallic strip or expansion element)
- Fresh gas outlet
- Agent-specific keyed filling assembly
Operating Principle
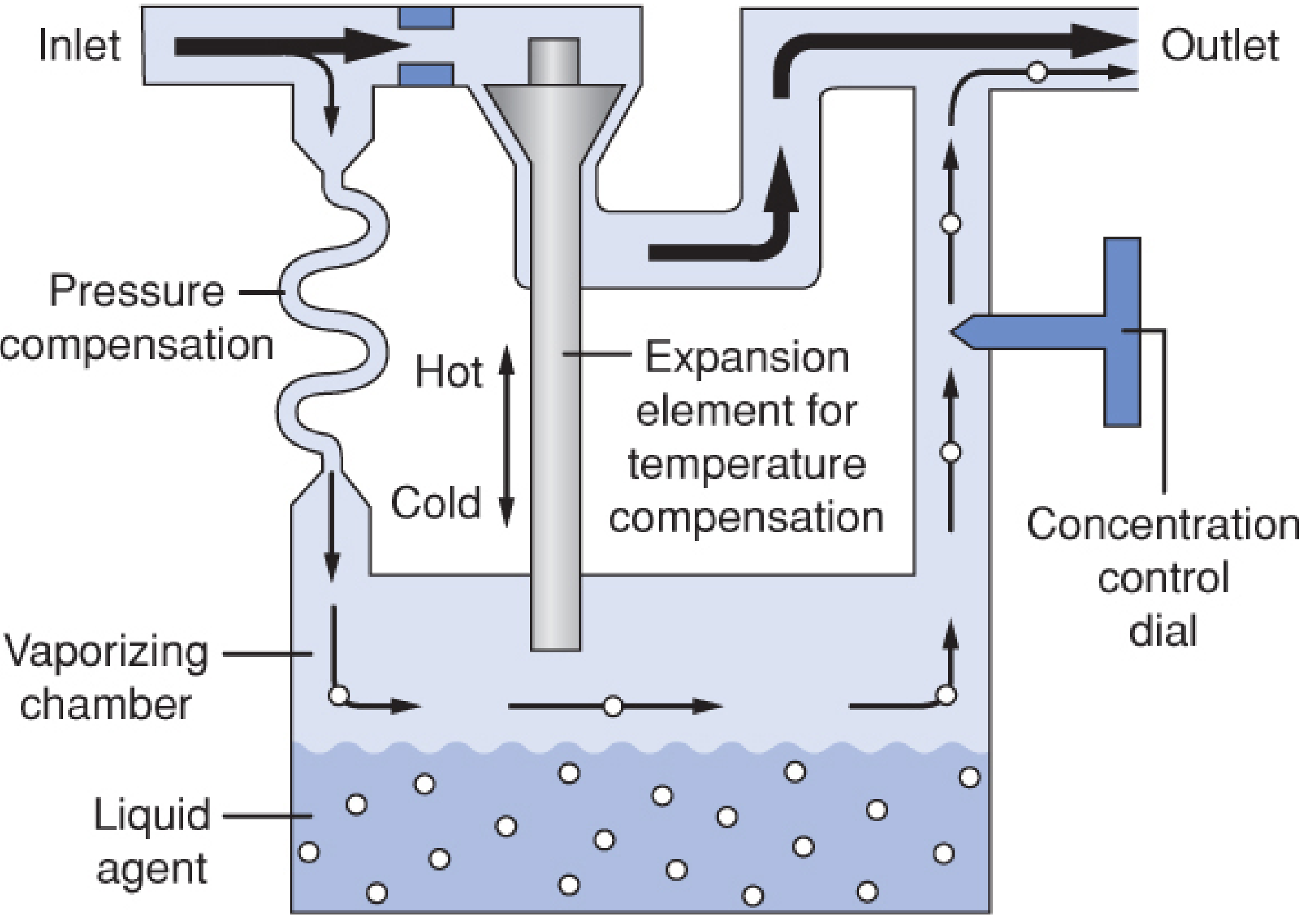
Key components: liquid agent in vaporizing chamber (bottom), expansion element for temperature compensation (center), pressure compensation coil (left), concentration control dial (right), bypass chamber (top).
Fresh gas from the flowmeters enters the vaporizer inlet and is split:
- Most of the gas goes through the bypass chamber - it never contacts liquid anesthetic
- A small fraction is directed into the vaporizing chamber, where it flows over wicks and baffles, picks up anesthetic vapor (approaching saturation), and exits as a concentrated vapor-laden stream
- The two streams recombine at the vaporizer outlet, yielding the dialed concentration
Splitting ratio = the ratio of bypass flow to vaporizing chamber flow; it is agent-specific and dial-setting-specific, set by the concentration control dial.
Example splitting ratios at 20°C for 1% output:
- Isoflurane: ~45:1 (bypass:vaporizing chamber)
- Sevoflurane: ~13:1
- Halothane: ~4.5:1
The wicks increase surface area for vaporization. The vaporizing chamber becomes partially (not fully) saturated due to constant fresh gas inflow; full saturation is assumed conceptually for calculation.
Temperature Compensation
As vaporization occurs, the liquid agent cools (evaporative heat loss), reducing SVP and potentially decreasing output. Temperature-compensating mechanisms counteract this:
- Bimetallic strip (GE Tec series): Two metals with different thermal expansion coefficients are bonded together. As temperature falls, the strip bends and diverts more gas through the vaporizing chamber (increasing output). As temperature rises, it bends the other way, diverting more gas to the bypass.
- Expansion element / bellows (Dräger Vapor 2000): A wax-filled or gas-filled element expands with heat, mechanically adjusting the bypass valve.
The vaporizer body is made from materials with high specific heat and high thermal conductivity to minimize temperature fluctuations.
4. Factors Affecting Vaporizer Output
Fresh Gas Flow (FGF) Rate
Output is less than dial setting at both extremes:
- Very low flows (<250 mL/min): Insufficient turbulence in vaporizing chamber; heavy vapor molecules are not adequately swept upward
- Very high flows (>15 L/min): Incomplete mixing; failure to saturate carrier gas; altered resistance characteristics
Output is most accurate at intermediate flow rates (0.5-10 L/min). - Barash's Clinical Anesthesia, 9e
Temperature
Contemporary temperature-compensated vaporizers maintain nearly linear output across a wide temperature range. Without compensation, output would fall as the liquid cools during prolonged use.
Intermittent Back Pressure ("Pumping Effect")
Positive-pressure ventilation or oxygen flush valve use creates retrograde pressure waves that can push gas backward into the vaporizing chamber, causing higher-than-expected output. This is:
- More pronounced at: low FGF, low dial settings, low liquid levels, rapid respiratory rates, high peak pressures
- Minimized in: modern variable bypass vaporizers (outlet check valve design)
Carrier Gas Composition
- Nitrous oxide (N2O) in the carrier gas can initially cause lower output vs. oxygen alone, because N2O is more soluble in the liquid anesthetic, temporarily "absorbing" into it
- Helium-based carriers affect viscosity and flow resistance, potentially altering output
Altitude / Barometric Pressure
- Variable bypass vaporizers: As altitude increases and barometric pressure falls, SVP (which is pressure-independent) stays constant, so the volume percent (v/v%) of anesthetic in the vaporizing chamber rises. However, because the partial pressure of anesthetic determines anesthetic depth (not volume percent), the clinical effect is minimal - no dial adjustment is needed for variable bypass vaporizers at altitude.
- Mathematically: the increased volume percent is offset by the lower barometric pressure, and partial pressure output is nearly unchanged.
- Barash's Clinical Anesthesia, 9e; Miller's Anesthesia, 10e
5. Desflurane Vaporizer (Tec 6 / D-Vapor)
Because desflurane cannot be used in a standard variable bypass vaporizer (SVP 669 mm Hg, boiling point 22.8°C), a purpose-built electrically heated, pressurized vaporizer was developed.
Why standard vaporizers fail for desflurane:
- SVP so high that dilution would require impossibly large bypass flows (~12 L/min to achieve 6%)
- Rapid evaporation would cause extreme cooling - uncompensatable with standard temperature mechanisms
- Boiling point near room temperature - agent would boil in the vaporizing chamber, making output uncontrollable
Tec 6 / Dual-Circuit Design
The Tec 6 is more accurately described as a dual-gas blender than a vaporizer:
- The desflurane sump is electrically heated to 39°C, generating vapor at 1300 mm Hg pressure
- A shut-off valve is either fully closed (dial OFF) or fully open (dial ON)
- A pressure-regulating valve downregulates desflurane vapor pressure to match fresh gas circuit pressure
- The operator controls output concentration via the concentration control valve (R2) - a variable restrictor
- Fresh gas and desflurane vapor run in two independent parallel circuits that combine at the outlet
Altitude effect on Tec 6: Unlike variable bypass vaporizers, the Tec 6 maintains a constant volume percent (not partial pressure) output regardless of ambient pressure. At altitude, partial pressure of desflurane falls proportionally:
Required dial setting = Normal dial setting × (760 mm Hg / ambient pressure)
So at 10,000 ft (~500 mm Hg), the dial must be increased by ~52% to maintain equivalent anesthetic depth. - Barash's Clinical Anesthesia, 9e
6. Cassette Vaporizer (GE Aladin)
The Aladin system (used on GE Aisys/Avance Carestations) is a single electronically controlled vaporizer that handles all five agents (halothane, isoflurane, enflurane, sevoflurane, desflurane) using interchangeable cassettes.
Key features:
-
Agent-specific, color-coded and magnetically coded cassettes (workstation auto-identifies the agent)
-
Functionally similar to variable bypass: bypass chamber + vaporizing chamber with fixed restrictor
-
Heart of the system: electronically controlled flow valve at the vaporizing chamber outlet, regulated by a CPU
-
CPU receives input from: concentration dial, pressure sensor, temperature sensor, bypass flow sensor, vaporizing chamber flow sensor, and flowmeter gas composition data
-
A one-way check valve at the vaporizing chamber inlet prevents retrograde flow - essential when delivering high-pressure desflurane vapor
-
Barash's Clinical Anesthesia, 9e
7. Injection Vaporizers
Some newer anesthesia platforms (e.g., Dräger Zeus, GE Aisys CS2 with certain configurations) use an injection-based system: liquid anesthetic is injected directly into the gas stream in metered doses, controlled electronically. This eliminates the traditional vaporizing chamber entirely.
8. Safety Features
| Feature | Purpose |
|---|---|
| Agent-specific keyed fillers | Prevent filling with wrong agent (color-coded, shape-coded) |
| Filler port at maximum safe level | Prevents overfilling |
| Interlock system | Prevents two vaporizers operating simultaneously |
| Removable mounts | Allow rapid exchange; also enable removal if MH is suspected |
| Outlet check valve (some machines) | Prevents backflow into vaporizer during IPPV |
| Tipping indicator | Liquid agent in the bypass channel after tipping causes overdose |
Misfilling Hazard
If a vaporizer (calibrated for isoflurane or sevoflurane) is accidentally filled with desflurane, a severe overdose results because desflurane's SVP (669 mm Hg) is far higher than the other agents. Agent-specific fillers reduce but do not eliminate this risk. Breathing circuit gas analysis is the last line of defense. - Miller's Anesthesia, 10e
9. Wash-In and Circuit Equilibration
Anesthetic delivery from the vaporizer (in L/min of gaseous drug) is approximated by:
V delivered = F_del × FGF × time
Where F_del = fractional concentration set on dial, FGF = fresh gas flow.
Circuit equilibration follows a single exponential function:
P_circ(t) = P_circ(0) + (P_del - P_circ(0)) × (1 - e^(-FGF/V_circ × t))
-
Time constant (τ) = V_circ / FGF
-
Doubling FGF halves wash-in time; doubling circuit volume doubles it
-
To wash anesthetic out, delivered partial pressure must be less than circuit partial pressure
-
Miller's Anesthesia, 10e
10. Quick Reference Summary
| Feature | Variable Bypass | Tec 6 (Desflurane) | Aladin Cassette |
|---|---|---|---|
| Agent(s) | Halothane, iso, enf, sevo | Desflurane only | All 5 agents |
| Heating | Passive (thermal mass) | Active (39°C electric) | Passive |
| Temperature comp. | Bimetallic strip / expansion element | Heated sump | Electronic |
| Altitude behavior | Partial pressure stable; no dial change needed | Vol% stable; dial adjustment needed | Agent-dependent |
| Key safety risk | Misfilling, pumping effect | Requires power; heater failure alarm | Electronic failure |
Sources:
- Miller's Anesthesia, 10e (Chapters 18, 20)
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e (Chapter 25)
This is a shared conversation. Sign in to Orris to start your own chat.