Why Ife facial muscles are more affected lmn than u m n legions
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a complete, well-sourced explanation.
Why Facial Muscles Are More Affected in LMN Than UMN Lesions
The key to understanding this lies in the dual (bilateral) cortical innervation of the facial nucleus in the pons.
The Anatomy of CN VII's Corticobulbar Control
The facial nucleus (CN VII) in the pons has two distinct parts:
| Part of Facial Nucleus | UMN Input | Controls |
|---|---|---|
| Rostral (upper) | Bilateral - from both contralateral AND ipsilateral motor cortex | Forehead, orbicularis oculi (upper face) |
| Caudal (lower) | Unilateral - only from contralateral motor cortex | Lower face (mouth, cheek, platysma) |
As stated in Bradley and Daroff's Neurology in Clinical Practice: "Supranuclear innervation is bilateral to the rostral portion of the nucleus, which innervates the upper facial muscles, but unilateral to the caudal portion, which innervates the lower facial muscles."
What Happens in a UMN Lesion (e.g., Stroke)
A stroke damages the upper motor neuron on one side of the brain (e.g., right hemisphere). The result:
- Lower face - loses its only source of UMN input (from the now-damaged right cortex). Weakness results.
- Upper face (forehead) - still receives intact UMN input from the unaffected left hemisphere. Forehead is SPARED.
So in a UMN lesion, only the contralateral lower face is weak. The upper face (forehead wrinkling, eye closure) is preserved or only mildly affected. This is "central-type" or "upper facial sparing" palsy.
What Happens in an LMN Lesion (e.g., Bell's Palsy)
A lower motor neuron lesion damages CN VII at or distal to the facial nucleus in the pons. Now the nerve fibers carrying signals to all ipsilateral facial muscles are cut off - regardless of which cortex the signal came from.
- Upper face: The bilateral UMN inputs are irrelevant - the final common pathway (CN VII fiber itself) is gone. Forehead weak.
- Lower face: Same - the nerve is damaged. Lower face weak.
Result: Entire ipsilateral face is paralyzed - upper and lower, including forehead. This is "peripheral-type" palsy.
As Rosen's Emergency Medicine explains: "The bilateral innervation of forehead musculature by upper motor neurons leads to a key distinguishing characteristic: upper motor neuron lesions spare the forehead while lower motor neuron lesions typically cause weakness affecting the entire ipsilateral face."
Visual Summary (Figure 12.13 - Neuroanatomy Through Clinical Cases)
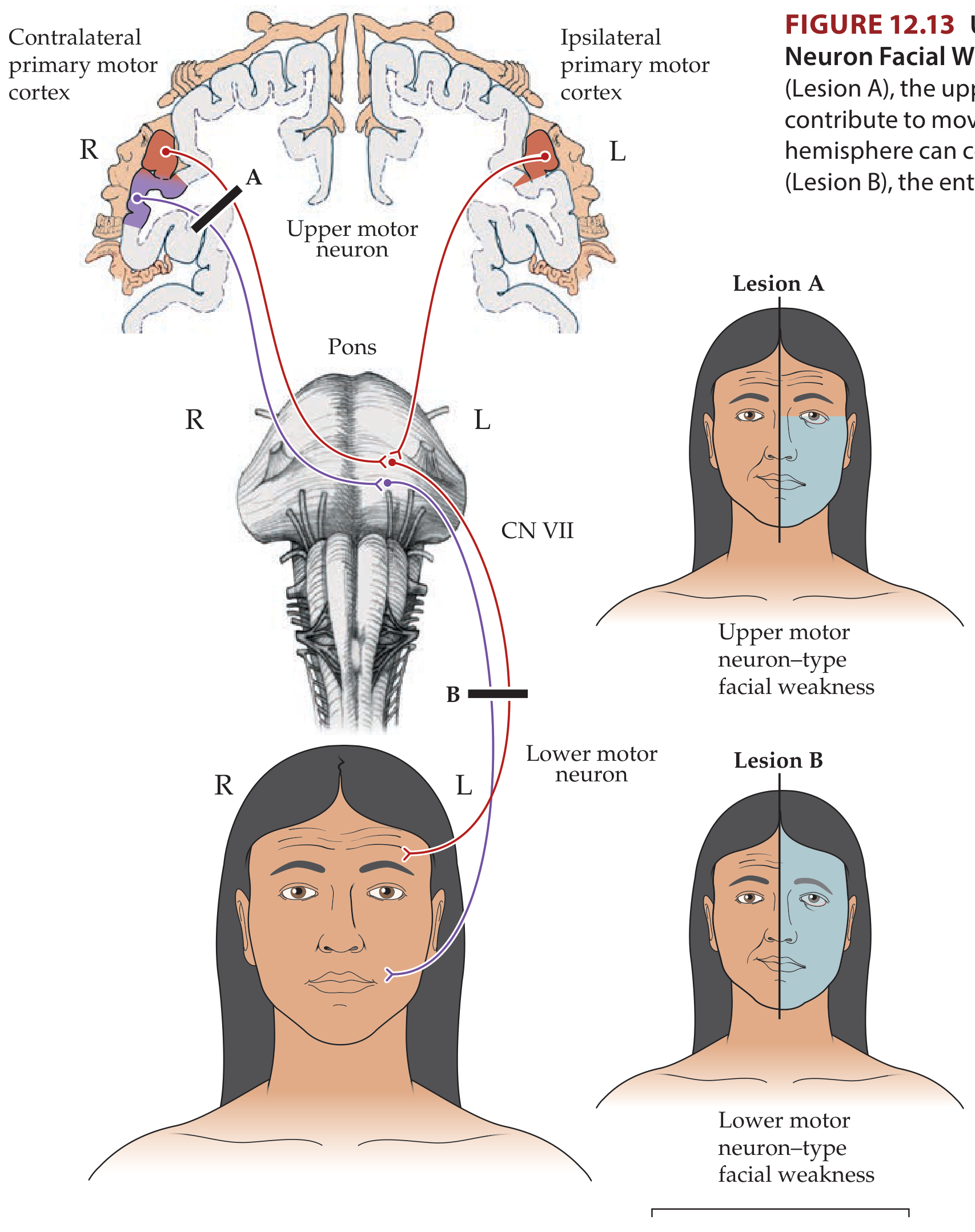
- Lesion A (UMN): Only the lower contralateral face is affected (blue = weak). Forehead normal.
- Lesion B (LMN): Entire ipsilateral face is affected including forehead.
Clinical Pearl - How to Distinguish UMN vs LMN Facial Palsy at the Bedside
| Feature | UMN Lesion | LMN Lesion |
|---|---|---|
| Forehead | Spared | Involved |
| Eye closure | Mild weakness or normal | Weak, lagophthalmos |
| Distribution | Contralateral lower face only | Entire ipsilateral face |
| Associated signs | Arm/leg weakness, aphasia, sensory loss | Hyperacusis, dry eye, taste loss |
| Common causes | Stroke, brain tumour | Bell's palsy, Ramsay Hunt, trauma |
Summary in One Sentence
Facial muscles are more completely affected in LMN lesions because the final common pathway (CN VII nerve itself) is destroyed, bypassing the protective bilateral cortical backup that normally preserves upper facial function in UMN lesions.
- Neuroanatomy Through Clinical Cases, 3rd Ed. (KCC 12.3)
- Bradley and Daroff's Neurology in Clinical Practice (Ch. 104)
- Rosen's Emergency Medicine (Ch. 91)
Make a study guide comparing all cranial nerve palsy patterns (CN V, IX, X, XII)
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Running Command
Writing File
Running Command
Running Command
Your study guide is ready:
CN Palsy Study Guide
PDF Document · PDF
Here is what is inside:
Page 1 - Overview Table
- All 12 CNs with type, exit foramen, and key function in one glance
- Classic mnemonic: Oh Oh Oh To Touch And Feel Very Good Velvet, Ah Heaven
Pages 2-13 - One section per CN (I through XII) each covering:
- Nucleus/origin and exit point
- Palsy features with clinical detail
- Causes (color-coded by CN)
- UMN vs LMN distinction highlighted in amber
- Clinical pearl box for each nerve
Final pages:
- Named syndromes table - Vernet, Collet-Sicard, Villaret, Tapia, Gradenigo, Cavernous sinus, SOF, Orbital apex, Wallenberg, Foster Kennedy
- Motor deviation quick reference - jaw/face/uvula/tongue/SCM - which way each deviates in LMN vs UMN
- Sensory testing summary - how to test CN I, II, V, VII, VIII, IX, X at the bedside
Sources: Neuroanatomy Through Clinical Cases 3e, Bradley & Daroff's Neurology, Rosen's Emergency Medicine, Localization in Clinical Neurology 8e
Why is mylohyoid known as safety muscle?
Finding Sources
Searching the Web
mylohyoid "safety muscle" floor of mouth anatomy clinical significance
Finding Sources
Reading Web Page
mylohyoid safety muscle floor of mouth clinical significance
Reading File
I now have all the material needed for a complete answer. Here it is:
The Mylohyoid - "Safety Muscle of the Floor of the Mouth"
Anatomy First
The mylohyoid is a flat, paired, sheet-like muscle that runs from the mylohyoid line of the mandible to the mylohyoid raphe and body of the hyoid bone. Together, the two sides form a muscular diaphragm - the actual floor of the oral cavity.
- Above it (sublingual space): tongue, sublingual gland, deep part of submandibular gland, lingual nerve, hypoglossal nerve (CN XII), lingual artery
- Below it (submandibular space): superficial lobe of submandibular gland, lymph nodes, facial vessels
- The two spaces communicate around the free posterior border of mylohyoid - a critical anatomical gap
Innervation: Nerve to mylohyoid (branch of inferior alveolar nerve, CN V3)
Why It Is Called the "Safety Muscle"
The mylohyoid acts as a physical barrier and structural guardian in four key ways:
1. It supports the tongue and prevents it falling back
When intact, the mylohyoid diaphragm supports the tongue from below. If it is weakened or breached, the tongue can drop posteriorly and inferiorly, directly threatening the airway. This support function is why it is considered "safe" to have - without it, even basic posture of the tongue becomes unsafe.
2. It is the barrier between the sublingual and submandibular spaces
The mylohyoid physically separates these two spaces. An intact mylohyoid contains infections in one compartment. Once it is breached - by a spreading odontogenic abscess, trauma, or surgery - infection crosses freely between spaces and can then spread into the parapharyngeal and retropharyngeal spaces, reaching the mediastinum.
This is the direct basis for Ludwig's angina - as Scott-Brown's Otorhinolaryngology explains:
"Ludwig's angina is a life-threatening airway complication of submandibular space infection, characterized by rapid onset of cellulitis of the floor of mouth tissues, causing swelling, induration and tongue elevation resulting in a compromised airway."
3. It confines swelling in a "safe" direction when intact
When the mylohyoid is intact but space infection occurs, the deep fascia and mylohyoid attachments limit distension to a cephalic (upward) and medial direction - pushing the tongue up. While uncomfortable, this is more manageable than uncontrolled inferior spread into the neck. The muscle's fascial envelope essentially directs the infection to stay relatively localised.
4. Breach = Plunging ranula / herniation
A ranula (mucous cyst of the sublingual gland) normally stays in the floor of the mouth above the mylohyoid. When the mylohyoid is penetrated - either due to a defect, trauma, or pressure - the ranula herniates through it and presents as a neck mass. This is called a plunging ranula, and demonstrates that the moment mylohyoid integrity is lost, oral cavity contents escape into the neck.
Summary Table
| Property | What the Mylohyoid Does | What Happens When Breached |
|---|---|---|
| Structural floor | Supports tongue from below | Tongue drops - airway at risk |
| Space divider | Keeps sublingual & submandibular spaces separate | Infection spreads freely between spaces |
| Swelling containment | Directs swelling upward/medially | Swelling spreads into neck and mediastinum |
| Organ containment | Keeps salivary gland cysts above | Plunging ranula herniates into neck |
Clinical Relevance
| Condition | Mylohyoid Role |
|---|---|
| Ludwig's angina | Infection crosses free posterior border of mylohyoid - floor of mouth cellulitis - airway emergency |
| Plunging ranula | Sublingual gland cyst herniates through mylohyoid into neck |
| Dental implants (lingual) | Implant perforation of mylohyoid can injure sublingual artery - life-threatening haematoma of floor of mouth |
| Periapical abscess (lower molars) | Root apices sit BELOW mylohyoid line - infection goes directly to submandibular space, not sublingual |
| Mandibular dentures | Mylohyoid ridge is the posterior lingual limit for denture extension |
The name "safety muscle" thus carries a double meaning: it keeps the airway and oral structures safe when intact, and its loss of integrity signals an immediately unsafe situation.
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Ch. 35 - Submandibular Space)
- Grainger & Allison's Diagnostic Radiology (Floor of Mouth Anatomy)
- Truong et al., 2022 - "Mylohyoid Muscle Revisited: Anatomic Features with Clinical Implications" (Int J Morphol)
Upper limb exam guide
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Writing File
Running Command
Running Command
Your guide is ready:
Upper Limb Anatomy Guide
PDF Document · PDF
Here is what is inside across 7 sections:
Section 1 - Brachial Plexus
- Full structure table: Roots → Trunks → Divisions → Cords → Branches (mnemonic: Real Teenagers Drink Cold Beer)
- All cord branches with roots and supply (long thoracic, suprascapular, axillary, thoracodorsal, etc.)
Section 2 - Muscles by Region
- Shoulder (deltoid, rotator cuff SITS + more) with origin, insertion, action, nerve, root
- Arm (biceps, brachialis, triceps, anconeus)
- Forearm anterior - all 9 muscles by layer (superficial to deep)
- Forearm posterior - all 10 extensor muscles by layer
- Hand: thenar, hypothenar, lumbricals, interossei (with PAD/DAB mnemonic)
Section 3 - Dermatomes + Cutaneous Nerves
- Root-by-root table C3–T2 with test point and peripheral nerve
- Autonomous zones for each named nerve (median = index tip, ulnar = little finger tip, radial = 1st web space)
Section 4 - Reflexes
- Biceps (C5/6), brachioradialis (C5/6), triceps (C6/7), Hoffmann's (UMN sign)
- Inversion of reflexes explained (C5/C6 spondylotic myelopathy pattern)
Section 5 - Nerve Injury Patterns
- Radial, median, ulnar, musculocutaneous, axillary - each with course, level-by-level deficits, clinical signs, pearl box
Section 6 - Brachial Plexus Injuries
- Erb's (C5/6), Klumpke's (C8/T1), middle trunk (C7), total plexus palsy - mechanism, posture, sensory loss
Section 7 - Hand Deformity Quick Reference
- Wrist drop, claw hand, ape hand, benediction hand, waiter's tip - nerve, level, appearance, mechanism
Sources: Gray's Anatomy for Students, Bradley & Daroff's Neurology, Das Manual on Clinical Surgery, Neuroanatomy Through Clinical Cases 3e
This is a shared conversation. Sign in to Orris to start your own chat.