What's the difference between hernia and hydrocele
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Here is a thorough comparison based on authoritative surgical textbooks (Bailey and Love's Surgery, Roberts and Hedges' Emergency Medicine, THIEME Atlas of Anatomy):
Hernia vs Hydrocele
Definition
| Feature | Hernia | Hydrocele |
|---|---|---|
| What it is | Protrusion of a viscus (organ/tissue) through an abnormal defect in the abdominal wall | Abnormal collection of serous fluid in part of the processus vaginalis, usually the tunica vaginalis around the testis |
| Contents | Bowel, omentum, or other abdominal organs | Clear serous fluid only |
| Location | Groin (inguinal), femoral region, umbilicus, abdominal wall, or scrotum | Scrotum (around the testis or along the spermatic cord) |
Anatomy & Embryology
Both conditions share a common embryological root - the processus vaginalis, a peritoneal diverticulum that descends with the testis through the inguinal canal around the 28th week of gestation.
- In a hernia: the processus vaginalis remains widely patent, allowing bowel or omentum to push through.
- In a hydrocele: the processus vaginalis allows only peritoneal fluid to trickle into the scrotal sac (communicating type), OR fluid accumulates locally due to imbalanced production/absorption (non-communicating type).
This is why indirect inguinal hernia and communicating hydrocele can coexist and are closely related.
Types
Hernia types:
- Indirect inguinal (most common) - passes through the deep inguinal ring, lateral to inferior epigastric vessels; congenital origin
- Direct inguinal - pushes through the posterior wall of the inguinal canal, medial to inferior epigastric vessels; acquired, due to muscle weakness
- Femoral - below the inguinal ligament; more common in women
- Umbilical, incisional, epigastric - other sites
- Reducible / Incarcerated / Strangulated - by clinical state (strangulated is a surgical emergency)
Hydrocele types (see diagram below):
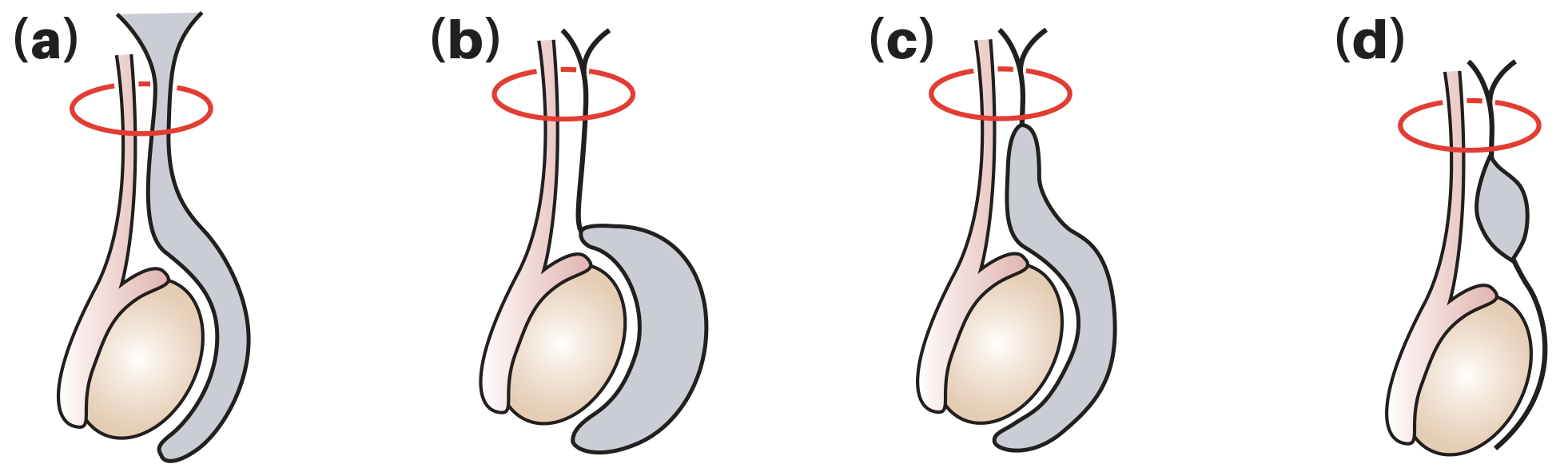
- (a) Communicating (congenital) - processus vaginalis stays patent; fluid flows freely from peritoneum to scrotum
- (b) Non-communicating (vaginal) - closed processus; fluid accumulates around the testis (most common in adults)
- (c) Infantile - mid-portion of processus patent
- (d) Hydrocele of the cord - isolated fluid collection along the spermatic cord
Clinical Comparison
| Feature | Hernia | Hydrocele |
|---|---|---|
| Swelling | Groin ± scrotum | Scrotum only |
| Get above it | Cannot get above the swelling in the groin | Can get above it in most cases |
| Transillumination | Does NOT transilluminate (bowel/omentum blocks light) | Transilluminates brightly (fluid is clear) |
| Cough impulse | Present (swelling increases with cough/Valsalva) | Absent (unless communicating type in children) |
| Reducibility | Often reducible (can push contents back into abdomen) | Not reducible |
| Consistency | Soft, gurgling (bowel); firm if incarcerated | Smooth, tense, fluctuant |
| Testis palpable | Testis usually palpable separately | Testis often not palpable (surrounded by fluid) |
| Pain | Can be painless; severe pain = strangulation (emergency) | Usually painless; acute pain suggests secondary cause (torsion, infection, trauma) |
Causes & Risk Factors
| Hernia | Hydrocele | |
|---|---|---|
| Congenital | Patent processus vaginalis | Patent processus vaginalis |
| Acquired | Muscle weakness, aging, raised intra-abdominal pressure, previous surgery | Idiopathic (primary); secondary to infection, trauma, torsion, tumour, radiotherapy |
| Tropical | - | Filariasis (Wuchereria bancrofti) - accounts for up to 80% of hydroceles in endemic areas |
| Age group | All ages; indirect more in young, direct more in elderly | Newborns (usually resolve by 18 months) and men >40 years |
Complications
Hernia:
- Incarceration (contents stuck, not reducible)
- Strangulation (compromised blood supply) - surgical emergency; leads to bowel ischemia/necrosis
Hydrocele:
- Pressure effects if very large
- If secondary to testicular tumour - malignant seeding if punctured (do NOT aspirate if tumour suspected)
- Filarial elephantiasis in endemic areas
Treatment
| Hernia | Hydrocele | |
|---|---|---|
| Conservative | Watchful waiting for small asymptomatic hernias | Usually resolves spontaneously in infants under 18 months |
| Surgery | Herniorrhaphy (mesh repair); laparoscopic or open | Jaboulay/Lord procedure (excision/plication of sac); surgery is mainstay in adults |
| Aspiration | Not applicable | Possible but high recurrence rate; avoided if tumour suspected |
Quick Memory Trick
- Hernia = "stuff coming through a hole" - bowel or fat pushing out through a fascial defect
- Hydrocele = "water around the testis" - fluid-filled sac, transilluminates, soft and fluctuant
Sources: Bailey and Love's Short Practice of Surgery, 28th ed., pp. 1581 & 1586; Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 816; THIEME General Anatomy and Musculoskeletal System Atlas, p. 248
Thank you so much
You're welcome! Feel free to ask anytime you have more questions. Good luck with your studies! 😊
This is a shared conversation. Sign in to Orris to start your own chat.