1/ gout ACR criteria for diagnosis, anti-inflammatories (NSAID, colchicine, steroid) indication, doses, monitoring, duration of therapy, ULT first line choices and monitoring. I have mcq and short exam in hospital explain it as a mentor
GOUT - Complete Exam Guide (ACR Criteria, Anti-inflammatories, ULT)
PART 1: DIAGNOSIS
Gold Standard
Exam tip: If they ask the single best test - it's synovial fluid analysis showing negatively birefringent needle-shaped crystals.
2015 ACR/EULAR Classification Criteria (Score ≥8 = Gout)
| Domain | Category | Points |
|---|---|---|
| Joint involvement | Ankle or midfoot (not 1st MTP) | 1 |
| 1st MTP joint (podagra) | 2 | |
| Symptom characteristics (3 features: erythema, tenderness, difficulty walking) | 1 feature | 1 |
| 2 features | 2 | |
| 3 features | 3 | |
| Time course (rapid peak <24h, resolution ≤14 days, complete resolution between flares) | 1 typical episode | 1 |
| Recurrent typical episodes | 2 | |
| Clinical evidence of tophi | Present | 4 |
| Serum urate (measured away from flare) | <4 mg/dL | -4 |
| 4-<6 mg/dL | 0 | |
| 6-<8 mg/dL | 2 | |
| 8-<10 mg/dL | 3 | |
| ≥10 mg/dL | 4 | |
| Synovial fluid analysis | MSU crystals negative | -2 |
| Imaging (US: double contour sign; DECT: urate deposition) | Present in symptomatic joint | 4 |
| Gout-related erosion on X-ray | 4 |
Exam tip: These criteria are for classification (research enrollment), not purely for clinical diagnosis. In practice, the clinical presentation + hyperuricemia + response to treatment is often sufficient. The criteria are commonly tested in MCQs.
2010 Diagnostic Decision Rule (for MCQ)
| Item | Points |
|---|---|
| Male sex | 2 |
| Previous patient-reported arthritis attack | 2 |
| Onset within 1 day | 0.5 |
| Joint redness | 1 |
| Involvement of 1st MTP joint | 2.5 |
| Hypertension or cardiovascular disease | 1.5 |
| Serum urate >5.88 mg/dL | 3.5 |
- Score ≤4: Gout very unlikely
- Score >4 and <8: Indeterminate - do synovial fluid analysis
- Score ≥8: Gout highly likely - treat
PART 2: ANTI-INFLAMMATORY THERAPY
When to Treat a Flare
A. COLCHICINE
- Acute gout flare (first-line)
- Prophylaxis when starting ULT
- Preferred when NSAIDs are contraindicated (e.g., CKD, peptic ulcer disease)
- 1.2 mg immediately, then 0.6 mg one hour later (1.8 mg total)
- Continue anti-inflammatory therapy until flare resolves
- Must be given within 12-36 hours of flare onset
- EULAR alternative: 1 mg loading dose, then 0.5 mg 1 hour later on day 1; maximum 3x 0.5 mg tablets per 24 hours
Exam tip: The old high-dose regimen (0.5 mg every hour until diarrhea) is no longer recommended. Low-dose is equally effective and far better tolerated.
- 0.6 mg once or twice daily (US) or 0.5 mg once or twice daily (outside US)
- Start 1-2 weeks before starting ULT
- Continue for minimum 3-6 months after achieving serum urate target (ACR: 3-6 months; EULAR: 6 months); longer if tophi present
- eGFR <45 mL/min: reduce prophylactic dose by 50%
- ESRD (dialysis): 0.5-0.6 mg once or twice per week (not daily)
- Avoid with strong CYP3A4 inhibitors (clarithromycin, protease inhibitors) or P-gp inhibitors (cyclosporine, tacrolimus, ketoconazole) - use alternative agent
- GI symptoms (diarrhea, nausea - most common side effect)
- Renal and liver function (before starting, periodically)
- CBC (myelosuppression with overdose)
- CK (colchicine myopathy - proximal muscle weakness + elevated CK)
- Drug interactions (CYP3A4, P-gp)
- Severe renal or hepatobiliary impairment
- Concurrent strong CYP3A4/P-gp inhibitors
- Narrow therapeutic index - overdose can be lethal
B. NSAIDs
- Acute gout flare (first-line, especially in younger patients without GI/renal/cardiovascular contraindications)
- Short-term prophylaxis if colchicine not tolerated
- Indomethacin: 50 mg TID x 2-3 days, then taper (most commonly cited in textbooks/exams)
- Naproxen: 500 mg BID
- Ibuprofen: 400-800 mg TID/QID
- Any full-dose NSAID is acceptable
- Renal function (serum creatinine, BUN) - NSAIDs reduce renal perfusion
- Blood pressure
- GI symptoms - add PPI for gastroprotection in high-risk patients
- Edema, fluid retention (relevant in heart failure)
- CKD (eGFR <30) - risk of acute kidney injury
- Active peptic ulcer disease
- Heart failure, cardiovascular disease
- Anticoagulant use (relative)
- Elderly (use with caution - higher GI and renal risk)
C. GLUCOCORTICOIDS
- Acute gout flare when both colchicine AND NSAIDs are contraindicated or poorly tolerated
- Polyarticular gout (steroids are especially effective here)
- Renal impairment patients (safest option)
- Patients on anticoagulation
- Oral prednisone: 30-50 mg/day as initial dose, gradually taper over 7-14 days as the attack resolves
- Intra-articular triamcinolone (or methylprednisolone): Excellent for monoarticular gout - effective, well-tolerated, minimal systemic effects
- Intramuscular triamcinolone: 40-60 mg as a single dose; useful when oral route not feasible or polyarticular gout
- Blood glucose (especially in diabetics - steroids cause hyperglycemia)
- Blood pressure
- Fluid retention / edema
- GI symptoms (add PPI)
- Signs of infection (steroids are immunosuppressive - must rule out septic arthritis before injecting)
Critical exam point: Always rule out septic arthritis before giving intra-articular steroids. MSU crystals do NOT exclude concurrent infection.
Comparing the Three (Quick MCQ Reference)
| Feature | Colchicine | NSAIDs | Glucocorticoids |
|---|---|---|---|
| CKD/renal impairment | Dose-reduce | Avoid | Preferred |
| Peptic ulcer/GI disease | Use | Avoid | Use (with PPI) |
| Heart failure | Use | Avoid | Caution |
| Polyarticular flare | Use | Use | Excellent |
| Diabetes | Use | Use | Caution (hyperglycemia) |
| Anticoagulants | Use | Avoid | Use |
PART 3: URATE-LOWERING THERAPY (ULT)
When to Start ULT (Indications)
- ≥2 gout flares per year
- Any tophi (subcutaneous or imaging-confirmed)
- Uric acid nephrolithiasis (kidney stones)
- Chronic gouty arthritis
- Gout with stage 3+ CKD (eGFR <45)
- First gout flare with serum urate >9 mg/dL
- First flare in a patient with CKD, urolithiasis, or certain comorbidities
Exam tip: Do NOT start ULT during an active flare - wait until the flare has fully resolved (or alternatively, if the patient is already on ULT, do NOT stop it during a flare).
- <6 mg/dL for most patients (below the saturation point of 6.8 mg/dL)
- <5 mg/dL for patients with tophi or severe/recurrent disease
First-Line ULT: Allopurinol
- eGFR ≥60: Start 100 mg/day
- eGFR <60: Start 50 mg/day
- Titrate by 100 mg (or 50 mg in CKD) every 2-4 weeks until serum urate target is achieved
- Maximum dose: 800 mg/day (though most patients achieve target at 300-400 mg/day)
Key principle: Start low, go slow. The starting dose reduces the risk of both hypersensitivity and flare precipitation.
- Serum urate: Check every 2-4 weeks during titration; then every 6 months once at target
- Renal function (creatinine/eGFR): Baseline and periodically - guides dose adjustment
- LFTs: Baseline (hepatitis can occur)
- CBC: Baseline (rarely causes myelosuppression)
- Skin: Watch for rash - even a mild rash should prompt holding the drug (can progress to AHS)
- HLA-B*5801 screening before starting in high-risk ethnicities: Han Chinese, Korean, Thai (Southeast Asian), Black patients, Pacific Islanders. If positive, use febuxostat instead.
- Allopurinol Hypersensitivity Syndrome (AHS): Severe rash (SJS/TEN), eosinophilia, fever, hepatitis, acute kidney injury. Risk factors: CKD, high starting dose (>100 mg/day in CKD), diuretic use, HLA-B*5801, within first 8 weeks of use. Rare (<1/1000) but potentially fatal.
- Mild rash: ~2% of users
Second-Line ULT: Febuxostat
- No dose adjustment needed in mild-moderate CKD (hepatically metabolized)
- Alternative for patients with HLA-B*5801 or allopurinol hypersensitivity
- Does NOT interact with azathioprine/6-MP the same way
- Cardiovascular events: The CARES trial showed a higher rate of cardiovascular death with febuxostat vs. allopurinol in patients with established CVD. Therefore, febuxostat is reserved for patients who fail or cannot tolerate allopurinol - it is NOT preferred over allopurinol as first-line in patients with cardiovascular disease.
- Monitor LFTs
- Serum urate every 2-4 weeks during titration
Third-Line / Additional Options
- Mechanism: Blocks renal tubular urate reabsorption (URAT1 inhibitor)
- Indicated when XOI is contraindicated or fails, in patients with normal-good renal function
- Dose: 500 mg BID, titrate to max 2-3 g/day
- Contraindicated: eGFR <30 mL/min, uric acid nephrolithiasis (increases urinary urate excretion - worsens stones)
- Adequate hydration and urine alkalinization required
- Drug interactions: Reduces excretion of many drugs (NSAIDs, methotrexate, penicillin)
- Recombinant uricase - converts urate to allantoin (more soluble)
- For refractory tophaceous gout unresponsive to oral ULT
- IV infusion every 2 weeks
- Monitor serum urate before each infusion - if urate rises above 6 mg/dL, stop (indicates antibody formation and loss of efficacy, and infusion reactions risk rises markedly)
Anti-inflammatory Prophylaxis While Starting ULT
- First-line prophylaxis: Low-dose colchicine (0.5-0.6 mg once or twice daily)
- Alternative: Low-dose NSAID if colchicine contraindicated
- Last resort: Low-dose prednisone
- ACR 2020: 3-6 months after achieving serum urate target; continue longer if flares persist
- EULAR 2016: 6 months minimum
- If tophi or severe disease: continue until tophi resolve and no further flares
PART 4: MONITORING SUMMARY TABLE (Exam Favorite)
| Drug | What to Monitor | When |
|---|---|---|
| Colchicine | GI symptoms, renal function, LFTs, CBC, CK, drug interactions | Baseline; periodically |
| NSAIDs | Renal function (Cr/BUN), BP, GI symptoms | Baseline; after 1-2 weeks of use |
| Steroids | Blood glucose, BP, edema, infection, GI | During use |
| Allopurinol | Serum urate, creatinine/eGFR, LFTs, CBC, skin rash; HLA-B*5801 in high-risk | Q2-4 weeks titrating; Q6 months at target |
| Febuxostat | Serum urate, LFTs, cardiovascular events | Q2-4 weeks titrating; Q6 months at target |
| Probenecid | Serum urate, renal function, urinary urate, urine output | Periodically; ensure adequate hydration |
HIGH-YIELD EXAM POINTS (Quick Recall)
- Gold standard diagnosis = MSU crystals in synovial fluid (negatively birefringent, needle-shaped)
- ACR criteria score ≥8 = classified as gout (if no crystals confirmed)
- First-line acute flare treatment = colchicine OR NSAIDs OR steroids (all equal)
- Colchicine dose = 1.2 mg then 0.6 mg one hour later (low-dose, within 12-36 h)
- Do NOT start ULT during an active flare; do NOT stop it if already on it
- Always give prophylaxis when starting ULT (colchicine preferred)
- Allopurinol = first-line ULT; start low (100 mg), titrate to target
- Serum urate target = <6 mg/dL (most patients), <5 mg/dL (tophi/severe)
- HLA-B*5801 screen before allopurinol in Han Chinese, Korean, Thai, Black patients
- Febuxostat = second-line; avoid as first-line in CVD patients (higher CV mortality vs allopurinol per CARES trial)
- Probenecid contraindicated in nephrolithiasis and eGFR <30
- Steroid preferred in CKD when colchicine and NSAIDs are both risky
- Allopurinol + azathioprine = dangerous combination (azathioprine toxicity) - reduce AZA dose by 75% or avoid
2/ osteoarthritis pain relief with NSAIDs, indication, doses, monitoring, duration of therapy, Xray findings (description)
OSTEOARTHRITIS - Complete Exam Guide
Pain Relief with NSAIDs, Indications, Doses, Monitoring, Duration, X-ray Findings
PART 1: QUICK ORIENTATION
- Hands: DIP joints (Heberden nodes), PIP joints (Bouchard nodes), 1st carpometacarpal (thumb base)
- Knees (medial compartment most common)
- Hips (superior joint space)
- 1st MTP joint (foot)
- Lumbar/cervical spine (facet joints, disc spaces)
Exam tip: OA affects DIP joints. RA spares DIP joints. This is a classic MCQ distinction. Heberden nodes (DIP) = OA. Bouchard nodes (PIP) = can occur in both OA and RA, but in OA they are bony hard, in RA they are soft/boggy.
PART 2: X-RAY FINDINGS (DESCRIPTION)
The 5 Classic Radiographic Features
- Represents cartilage loss (cartilage is not visible on X-ray; what you see is the space it occupies)
- In OA, JSN is asymmetric/focal - occurs in areas of maximal stress, not uniform across the joint
- This asymmetry is a key distinguishing feature from RA (where JSN is symmetric/diffuse)
- Example: Knee OA - medial compartment narrowing more than lateral; Hip OA - superior joint space narrowing
- Pathognomonic of OA - the "hypertrophic" aspect of the disease
- New bone formation at joint margins (marginal osteophytes)
- Can also form within the subchondral bone at the joint line
- Comprise trabecular bone; may appear on one or both sides of the joint
- At the hip: osteophytes form a rim around the femoral head/neck junction
- At finger joints: form the basis of Heberden and Bouchard nodes
- Increased osteoblastic activity in the bone immediately beneath the cartilage
- Appears as increased white (dense) bone on X-ray beneath the narrowed joint space
- Reflects attempted repair response
- Round/oval lucencies within the subchondral bone
- Form when synovial fluid is forced through damaged cartilage into the bone under pressure
- Appear as dark (lucent) areas surrounded by sclerotic rim
- Fragments of cartilage/bone shed into the joint may persist as intra-articular loose bodies
- May become revascularized and grow within the joint
- Ligamentous laxity leads to malalignment, varus/valgus deformity, and subluxation
Exam mnemonic: LOSS-D = Loss of joint space (asymmetric), Osteophytes, Sclerosis (subchondral), Subchondral cysts, Deformity/loose bodies
X-ray by Joint (Exam High-Yield)
| Joint | Key X-ray Feature |
|---|---|
| Knee | Medial compartment JSN (most common) → varus deformity; weight-bearing X-ray is most sensitive |
| Hip | Superior joint space narrowing (most common pattern) |
| Hand (DIP/PIP) | Marginal osteophytes forming Heberden/Bouchard nodes; JSN at interphalangeal joints |
| Thumb base (CMC) | JSN + osteophytes at 1st carpometacarpal joint; "shelf" osteophyte |
| Spine | Disc space narrowing + marginal osteophytes (syndesmophytes) at vertebral body margins |
The OA Hip X-ray (Classic Exam Image)
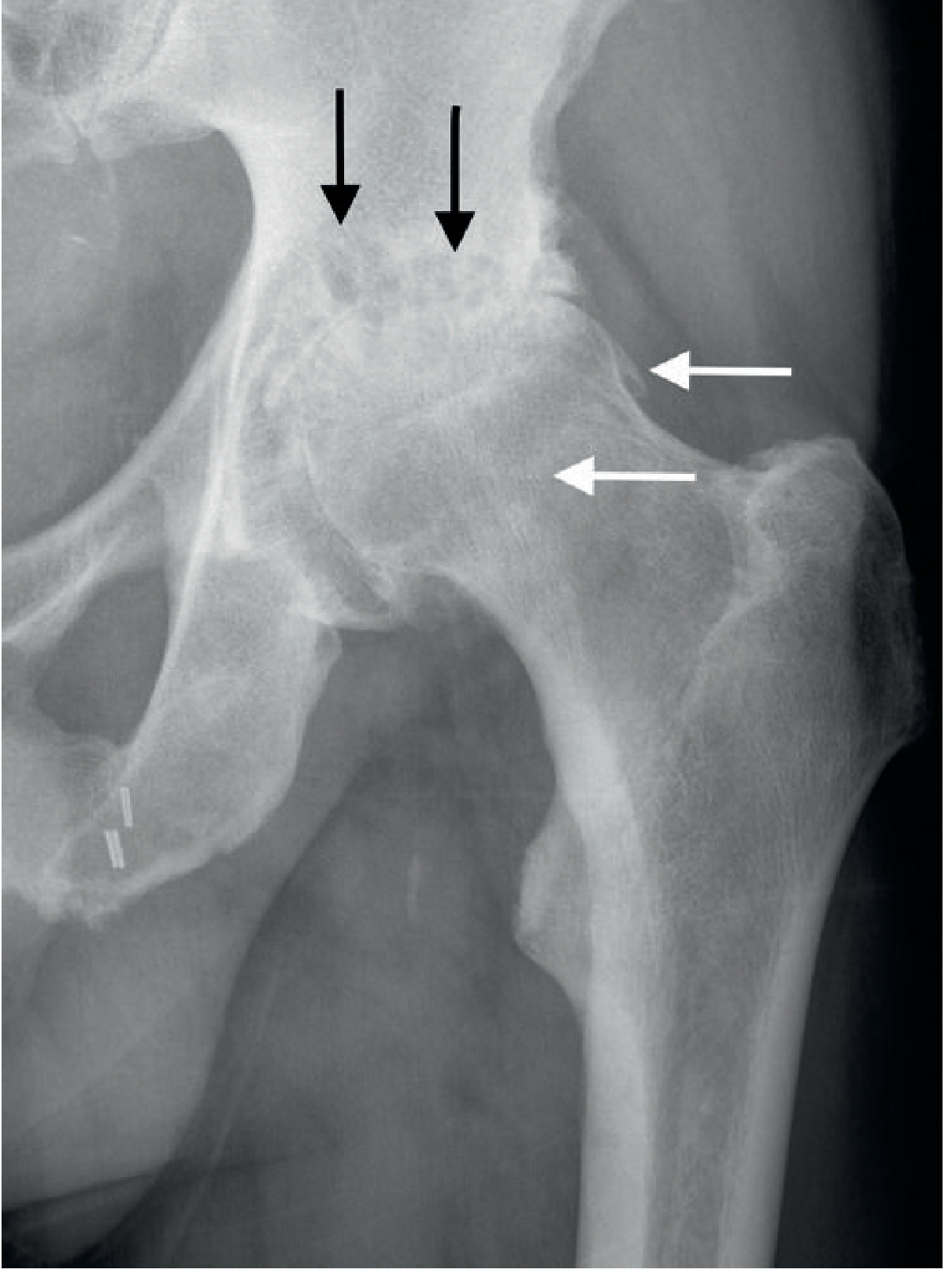
Important exam point: Pain poorly correlates with X-ray severity. A patient with terrible X-ray changes may report mild symptoms, and vice versa. Always treat the patient, not the image.
PART 3: PHARMACOLOGIC PAIN RELIEF - THE ANALGESIC LADDER IN OA
Step 1 (Always First): Non-pharmacologic
Step 2: Acetaminophen (Paracetamol)
- First pharmacologic agent per many guidelines (ACR, EULAR, OARSI) for mild-moderate pain
- Dose: 500-1000 mg every 6-8 hours; maximum 3-4 g/day (2 g/day in elderly or liver disease)
- Advantages: safe in renal disease, cardiovascular disease, elderly
- Limitations: inferior to NSAIDs for inflammation; limited by liver toxicity at high doses; recent evidence questions its efficacy in knee/hip OA
Step 3: Topical Therapy
- Topical diclofenac (gel or patch): preferred for localized OA (hands, knees) especially in elderly and patients with GI/renal/CV risk; systemic absorption is much lower than oral
- Topical capsaicin: useful adjunct, especially for hand OA
- Topical NSAIDs are preferred over oral NSAIDs in patients with comorbidities
PART 4: NSAIDs IN OSTEOARTHRITIS
Indications for NSAIDs in OA
- Acetaminophen and/or topical agents provide inadequate pain relief
- Moderate-to-severe OA pain with significant inflammatory component (swelling, warmth, morning stiffness)
- Patient needs functional improvement for daily activities
- No major contraindications exist
Exam principle: NSAIDs address both the inflammatory and nociceptive components of OA pain. Acetaminophen only addresses the nociceptive component. NSAIDs are more effective than acetaminophen for OA but carry more risks.
Commonly Used NSAIDs and Doses
| Drug | Dose | Frequency | Notes |
|---|---|---|---|
| Ibuprofen | 400-800 mg | TID-QID (max 3200 mg/day) | Most commonly used; best safety profile at lower doses |
| Naproxen | 250-500 mg | BID (max 1000-1250 mg/day) | Longer half-life (twice daily); preferred in elderly (less CV risk vs. ibuprofen?) |
| Diclofenac | 50 mg | BID-TID (max 150 mg/day) | Also available as topical gel (1% or 3%) |
| Meloxicam | 7.5-15 mg | Once daily | Preferential COX-2 selectivity; less GI risk |
| Celecoxib (COX-2 inhibitor) | 100-200 mg | Once or twice daily | Better GI safety; cardiovascular risk similar to non-selective NSAIDs; preferred in patients with GI risk |
| Indomethacin | 25-50 mg | TID (max 150-200 mg/day) | More potent but more side effects; generally avoided long-term in OA |
| Nabumetone | 1000-2000 mg | Once daily or divided | Prodrug; lower GI risk |
Exam tip: All NSAIDs are considered roughly equivalent in efficacy for OA. Drug choice is driven by side effect profile, patient comorbidities, and cost, not by superior analgesic efficacy.
COX-2 Selective Inhibitors (e.g., Celecoxib)
- Preferred when GI risk is high (history of peptic ulcer, elderly, on corticosteroids or anticoagulants)
- Same cardiovascular risk as non-selective NSAIDs - NOT safer for the heart
- Contraindicated in sulfonamide allergy (celecoxib has a sulfonamide moiety)
Topical NSAIDs (Preferred in Specific Situations)
- Topical diclofenac gel (Voltaren): apply to the affected joint 3-4 times daily
- Recommended for elderly patients and those with GI, renal, or cardiovascular comorbidities
- Systemic side effects much lower but still possible with extensive use
PART 5: NSAID CONTRAINDICATIONS AND WHEN TO AVOID
| Condition | NSAID Concern | Alternative |
|---|---|---|
| CKD (eGFR <30) | Reduce renal perfusion, cause AKI, worsen CKD | Acetaminophen, opioids (cautiously) |
| Heart failure | Sodium/water retention, worsen HF | Acetaminophen, topical NSAIDs |
| Cardiovascular disease | Increased MI and stroke risk (especially diclofenac, COX-2 inhibitors) | Naproxen (least CV risk of oral NSAIDs) |
| Active peptic ulcer / GI bleeding | COX-1 inhibition reduces gastric mucosal protection | Topical NSAIDs, acetaminophen |
| Anticoagulants (warfarin) | Bleeding risk (COX-1 inhibition + displacement) | Acetaminophen, topical NSAIDs |
| Aspirin therapy | Ibuprofen competes with aspirin binding site (blocks cardioprotection) | Celecoxib, naproxen, or take aspirin 2h before ibuprofen |
| Third trimester pregnancy | Premature closure of ductus arteriosus | Acetaminophen |
| Elderly (>65) | GI bleeding, renal impairment, fluid retention, falls | Topical NSAIDs; if oral needed, use lowest dose + PPI |
PART 6: GI PROTECTION WITH NSAIDs
- Age >65
- History of peptic ulcer disease or GI bleeding
- Concurrent corticosteroid use
- Concurrent anticoagulant use
- Concurrent antiplatelet agent use
- High-dose or prolonged NSAID use
Exam point: PPI (omeprazole, lansoprazole, pantoprazole) is the preferred gastroprotective agent with NSAIDs. H2 blockers are less effective for NSAID-related gastroprotection.
PART 7: MONITORING DURING NSAID THERAPY
What to Monitor and When
| Parameter | Why | When to Check |
|---|---|---|
| Renal function (Creatinine/eGFR) | NSAIDs reduce renal prostaglandins → decrease renal blood flow → AKI, hyperkalemia, fluid retention | Baseline; 1-2 weeks after starting; every 3-6 months on long-term therapy |
| Blood pressure | Sodium/water retention causes HTN; blunts antihypertensive effect | Baseline; within 1-2 weeks; each visit |
| GI symptoms | Peptic ulcer, GI bleeding (upper more than lower) | Every visit; stool occult blood if indicated |
| CBC | Anemia (chronic GI blood loss); rarely, blood dyscrasias | Baseline; annually on long-term therapy |
| LFTs | NSAIDs can cause hepatotoxicity (rare but possible, especially diclofenac) | Baseline; periodically |
| Edema | Fluid retention; watch in HF or hypoalbuminemia | Each visit |
| Cardiovascular events | MI, stroke risk | Clinical assessment each visit; minimize duration |
Mnemonic for NSAID monitoring: "REGAL" = Renal function, Edema/BP, GI symptoms, ALT/LFTs, Lab CBC
PART 8: DURATION OF NSAID THERAPY
Principles:
- Intermittent (as-needed) use is preferred over continuous daily dosing when pain is episodic or activity-related
- Continuous use is justified only when pain is persistent and inadequately controlled by as-needed dosing
- Reassess every 1-3 months: Is the lowest effective dose being used? Can the dose be reduced or stopped?
- Step down to topical therapy or acetaminophen once pain improves
- No fixed maximum duration in guidelines - but long-term use requires active monitoring and documented benefit vs. risk reassessment
- In elderly patients: try to limit to <2-4 weeks at a time unless benefit clearly outweighs risk
Exam key point: Unlike antibiotics, there is no fixed "course" for NSAIDs in OA. The principle is "use the minimum necessary." The exam may ask: when do you stop? Answer: when pain is controlled or comorbidities make continued use unsafe, and reassess regularly.
PART 9: BEYOND NSAIDs - THE FULL PHARMACOLOGIC LADDER
| Step | Agent | When |
|---|---|---|
| 1 | Non-pharmacologic (exercise, weight loss, PT) | Always first |
| 2 | Acetaminophen | Mild pain, no inflammation |
| 3 | Topical NSAIDs / topical diclofenac | Localized OA, elderly, GI/renal risk |
| 4 | Oral NSAIDs ± PPI | Moderate-severe pain, inflammatory component |
| 5 | Intra-articular corticosteroid injection | Acute flare with effusion; one joint |
| 6 | Intra-articular hyaluronic acid (viscosupplementation) | Controversial; ACR gives conditional recommendation against in knee OA |
| 7 | Duloxetine (SNR inhibitor) | Central sensitization, inadequate NSAID response |
| 8 | Tramadol (weak opioid) | Severe pain, contraindications to all above |
| 9 | Joint replacement surgery | End-stage OA, failed conservative management |
PART 10: HIGH-YIELD MCQ SUMMARY
- X-ray classic triad of OA: Joint space narrowing (asymmetric) + osteophytes + subchondral sclerosis
- OA vs RA on X-ray: OA = asymmetric JSN + osteophytes (no erosions); RA = symmetric JSN + periarticular erosions + osteopenia (no osteophytes)
- OA vs RA on exam: OA = bony-hard Heberden nodes (DIP); RA = spares DIP, affects MCP/PIP
- X-ray vs symptoms in OA: Poorly correlated - treat the patient's pain, not the X-ray
- First pharmacologic agent in OA: Acetaminophen (though NSAIDs are more effective)
- NSAIDs in OA: indicated for moderate-to-severe pain; lowest dose, shortest duration
- GI protection: Always add PPI when using oral NSAIDs in high-risk patients
- Best NSAID for cardiovascular-risk patients: Naproxen (least CV risk among oral NSAIDs)
- Safest route in elderly with GI/renal risk: Topical diclofenac
- Monitor on NSAIDs: Renal function, blood pressure, GI symptoms, edema
- Celecoxib: Better GI safety, same cardiovascular risk - do NOT use in sulfonamide allergy
- Ibuprofen + aspirin: Competition at COX-1 binding site; ibuprofen can block aspirin's cardioprotection
- NSAID + warfarin: Increased bleeding risk; avoid combination; use acetaminophen instead
- NSAIDs in pregnancy (3rd trimester): Contraindicated - premature closure of ductus arteriosus
3/ rheumatoid arthritis ACR classification criteria, DMARDS for long term management, indication, doses, monitoring, duration of therapy, evaluation for disease activity
RHEUMATOID ARTHRITIS - Complete Exam Guide
ACR Criteria, DMARDs, Disease Activity Evaluation
PART 1: OVERVIEW - THE KEY CONCEPTS
- Treat-to-target (T2T): The goal is remission or low disease activity, not just symptom control
- Early aggressive treatment: Start DMARDs as soon as RA is diagnosed - delay means irreversible joint damage
- Anchor drug principle: Methotrexate is the backbone of almost every regimen
PART 2: 2010 ACR/EULAR CLASSIFICATION CRITERIA
| Domain | Category | Points |
|---|---|---|
| A. Joint Involvement | 1 large joint (shoulder, elbow, hip, knee, ankle) | 0 |
| 2-10 large joints | 1 | |
| 1-3 small joints (MCP, PIP, wrists, thumb IP, MTP) | 2 | |
| 4-10 small joints | 3 | |
| >10 joints (at least 1 small joint) | 5 | |
| B. Serology (at least 1 test needed) | Negative RF AND negative ACPA | 0 |
| Low-positive RF or low-positive anti-CCP (<3x ULN) | 2 | |
| High-positive RF or high-positive anti-CCP (>3x ULN) | 3 | |
| C. Acute-phase Reactants (at least 1 needed) | Normal CRP AND normal ESR | 0 |
| Abnormal CRP OR abnormal ESR | 1 | |
| D. Duration of Symptoms | <6 weeks | 0 |
| ≥6 weeks | 1 |
Maximum score: 10. Score ≥6 = Definite RA.
Important Notes About the 2010 Criteria (Exam Traps)
- Classification ≠ Diagnostic criteria - They identify patients likely to develop chronic progressive disease, not replace clinical judgment
- No requirement for symptoms >6 weeks - unlike the old 1987 criteria (which required 6 weeks). Why? Viral polyarthritis typically resolves in 2-3 weeks, but you don't need to wait 6 weeks to classify someone as RA
- Anti-CCP (ACPA) included - more specific than RF (~90% specific). RF alone is less specific (positive in infection, SLE, Sjogren's, hepatitis C, healthy elderly)
- Rheumatoid nodules and X-ray erosions NOT included - they occur too late in disease to be useful for early classification
- Seronegative RA = about 25% of patients are RF and ACPA negative - can still have RA
Key Laboratory Tests in RA
- RF (IgM): Positive in ~80% of RA; positive in many other conditions (low specificity)
- Anti-CCP (anti-cyclic citrullinated peptide): ~90% specific for RA; most specific test; predicts more aggressive disease and erosive joint damage
- ESR and CRP: Non-specific inflammatory markers; used to track activity
- CBC: Anemia of chronic disease, thrombocytosis in active RA
- Anti-CCP positive + RF positive = highest risk for erosive, destructive disease
Exam tip: "Which antibody is most specific for RA?" = Anti-CCP (ACPA). "Which predicts erosive disease?" = Anti-CCP positive.
PART 3: DISEASE ACTIVITY EVALUATION
DAS28 (Disease Activity Score in 28 Joints) - Most Widely Used
- Number of tender joints (28 joints assessed)
- Number of swollen joints (28 joints assessed)
- ESR (mm/hr) or CRP (mg/L)
- Patient Global Assessment (PGA) - visual analog scale 0-100 mm
| DAS28 Score | Disease Activity Category |
|---|---|
| >5.1 | High disease activity |
| 3.2 - 5.1 | Moderate disease activity |
| 2.6 - 3.2 | Low disease activity |
| <2.6 | Remission |
Exam tip: Target = DAS28 <2.6 (remission) or at minimum <3.2 (low disease activity). If not achieved at 3-6 months - escalate therapy.
Other Disease Activity Tools
| Tool | Components | Notes |
|---|---|---|
| SDAI (Simplified DAI) | SJC28 + TJC28 + PGA + evaluator global + CRP | Simple arithmetic sum; no calculator needed |
| CDAI (Clinical DAI) | SJC28 + TJC28 + PGA + evaluator global (no labs) | Useful in clinic without lab results |
| ACR20/50/70 | % improvement in tender/swollen joints + 3 of 5 other measures | Used in clinical trials as endpoints, not routine practice |
| RAPID3 | Patient-reported outcomes only | Quick self-administered questionnaire |
Treat-to-Target (T2T) Principle
- Assess disease activity every 1-3 months in active disease
- If target not achieved after 3 months of therapy - adjust treatment
- Once at target - monitor every 3-6 months
- ACR 2021 guidelines: Recommend targeting remission (DAS28 <2.6) as primary goal, especially in early disease; low disease activity is acceptable in established disease if remission not achievable
PART 4: DMARDS - OVERVIEW
- Conventional synthetic DMARDs (csDMARDs): Methotrexate, hydroxychloroquine, sulfasalazine, leflunomide
- Biologic DMARDs (bDMARDs): TNF inhibitors, IL-6 inhibitors, abatacept, rituximab
- Targeted synthetic DMARDs (tsDMARDs): JAK inhibitors (tofacitinib, baricitinib, upadacitinib)
PART 5: CONVENTIONAL DMARDs IN DETAIL
1. METHOTREXATE (MTX) - THE ANCHOR DRUG
- Start: 10-15 mg once weekly (oral or subcutaneous)
- Escalate by 5 mg every 4-6 weeks based on response and tolerability
- Target dose: 15-25 mg once weekly
- At doses >15 mg/week: subcutaneous route preferred (oral absorption becomes saturated and variable)
- Always give folic acid 1 mg/day (or 5 mg once weekly) to reduce side effects (especially mucositis, GI toxicity, alopecia) without reducing efficacy
| Parameter | Frequency | Why |
|---|---|---|
| CBC | Baseline; every 2-3 months | Myelosuppression (leukopenia, thrombocytopenia) |
| LFTs (AST/ALT) | Baseline; every 2-3 months | Hepatotoxicity (elevation common; fibrosis/cirrhosis rare) |
| Creatinine/eGFR | Baseline; every 2-3 months | MTX renally excreted; renal impairment → toxicity |
| Viral hepatitis panel (HBsAg, anti-HBc, anti-HCV) | Baseline only | Reactivation of hepatitis B; fulminant hepatitis possible |
| Chest X-ray | Baseline | MTX pneumonitis (rare but serious) |
| Albumin | Periodically | Low albumin → less protein binding → more free MTX → toxicity |
- ALT/AST >3x ULN: hold and recheck
- If persistently elevated: stop and consider liver biopsy
- Creatinine clearance <30 mL/min: avoid MTX (accumulates, causes toxicity); dialysis is an absolute contraindication
- Pregnancy: absolute contraindication (Category X - teratogenic, causes fetal death and major malformations); stop 3+ months before planned conception
- GI: nausea, vomiting, diarrhea, stomatitis/mouth ulcers (most common - reduced by folic acid)
- Hepatotoxicity: transaminase elevation common; fibrosis/cirrhosis with long-term use (especially with alcohol)
- Myelosuppression: leukopenia, thrombocytopenia
- Pulmonary: acute interstitial pneumonitis (rare ~0.4%; presents with dyspnea, cough, fever)
- Alopecia (reduced by folic acid)
- Opportunistic infections (PCP, herpes zoster)
- Teratogenicity - must be stopped before pregnancy
Drug interactions (Exam high-yield):
- NSAIDs/aspirin/penicillin/probenecid - inhibit MTX renal tubular secretion → increased MTX levels (generally only clinically relevant at higher doses)
- TMP-SMX - both inhibit folate metabolism → additive toxicity (avoid combination)
- Alcohol - additive hepatotoxicity; patients must minimize/avoid alcohol
2. HYDROXYCHLOROQUINE (HCQ)
- Irreversible retinal damage ("bull's eye maculopathy") is the most serious side effect
- Usually dose-dependent and cumulative
- Screening:
- Baseline eye exam if age ≥40 or prior eye disease
- Then optical coherence tomography (OCT) + visual field testing every 12 months
- Other side effects: nausea, diarrhea, headache, skin rash; rare cardiotoxicity (prolonged QT, conduction abnormalities) and blood dyscrasias
Exam tip: "What monitoring is required for hydroxychloroquine?" = Annual ophthalmology review (OCT + visual fields). Maximum dose ≤5 mg/kg/day.
3. SULFASALAZINE (SSZ)
- Start: 500 mg twice daily
- Maintenance: 1000-1500 mg twice daily (2-3 g/day total)
| Parameter | Frequency |
|---|---|
| CBC | Every 2-4 weeks for first 3 months, then every 3 months |
| LFTs | Every 3 months initially, then every 3-6 months |
| G6PD level | Baseline (risk of hemolytic anemia in G6PD deficiency) |
4. LEFLUNOMIDE
- CBC and LFTs every 2-3 months
- Creatinine periodically
- Baseline: CBC, LFTs, viral hepatitis panel
- Diarrhea (most common GI)
- Alopecia
- Hepatotoxicity
- Hypertension
- Myelosuppression
- Teratogenic - Category X (contraindicated in pregnancy; must washout with cholestyramine before conception)
Exam tip: Leflunomide and MTX = both Category X (teratogenic). Both require washout before pregnancy. Leflunomide needs cholestyramine washout because of its very long half-life (enterohepatic recirculation).
PART 6: BIOLOGIC DMARDs
5. TNF-α INHIBITORS (Anti-TNF Agents)
| Agent | Route | Dosing |
|---|---|---|
| Etanercept | SC | 50 mg/week or 25 mg twice weekly |
| Adalimumab | SC | 40 mg every 2 weeks |
| Infliximab | IV | 3 mg/kg at weeks 0, 2, 6 then every 8 weeks (can increase to 10 mg/kg) |
| Certolizumab pegol | SC | 400 mg at weeks 0, 2, 4 then 200 mg every 2 weeks |
| Golimumab | SC/IV | 50 mg/month SC |
- TB screening: Tuberculin test (TST) or IGRA (QuantiFERON) + chest X-ray. Latent TB must be treated before starting (9 months INH or 4 months rifampin). Risk of reactivation is the most important safety concern with TNF inhibitors
- Hepatitis B serology (HBsAg, anti-HBc, anti-HBs): TNF inhibitors can cause HBV reactivation
- Hepatitis C screening
- HIV if indicated
- Live vaccine update BEFORE starting (cannot give live vaccines while on biologics)
- Serious infections (bacterial, fungal - especially histoplasmosis, coccidioidomycosis)
- TB reactivation (most important - hence mandatory TB screening)
- Demyelinating disease (multiple sclerosis-like) - avoid in established demyelinating disease
- CHF exacerbation - avoid TNF inhibitors in moderate-to-severe heart failure (NYHA III-IV)
- Drug-induced lupus (especially infliximab, etanercept)
- Increased lymphoma risk (controversial)
- Injection site reactions / infusion reactions
- LFTs periodically
- Signs of infection at each visit
- CBC if clinical concern
- Annual TB screening (some guidelines)
6. OTHER BIOLOGICS (High-Yield Summary)
| Drug | Class | Key Points |
|---|---|---|
| Tocilizumab | IL-6 receptor inhibitor | Also effective as monotherapy (unlike most biologics); can normalize CRP/ESR (masking inflammation marker monitoring); watch LFTs, lipids, neutrophil count |
| Abatacept | CTLA-4-Ig (T-cell co-stimulation blocker) | Blocks CD28-CD80/86 interaction; IV or SC; lower infection risk than TNF inhibitors; preferred in seropositive (RF/ACPA positive) patients |
| Rituximab | Anti-CD20 (B-cell depletion) | IV infusion every 6 months; preferred in patients with previous lymphoma (safer than TNF inhibitors); screen for HBV (reactivation risk); infusion reactions; monitor immunoglobulin levels |
| IL-1 inhibitors (anakinra) | IL-1 receptor antagonist | Less used now; daily SC injections; good for Still's disease and periodic fever syndromes |
7. JAK INHIBITORS (tsDMARDs) - Targeted Synthetic
| Drug | Dose |
|---|---|
| Tofacitinib | 5 mg BID or 11 mg XR once daily |
| Baricitinib | 2 mg or 4 mg once daily |
| Upadacitinib | 15 mg once daily |
- Same TB and viral reactivation screening as biologics required
- Cardiovascular events and venous thromboembolism (VTE) risk (class warning, especially tofacitinib); use caution in CV risk patients
- Malignancy risk (especially non-melanoma skin cancer)
- Herpes zoster reactivation (higher than TNF inhibitors)
- Anemia, neutropenia
- Black box warning for serious infections, malignancy, CV events, thrombosis
Exam tip: JAK inhibitors are oral - convenient. But they carry a black box warning for thrombosis and cardiovascular events (FDA). This is a key MCQ distinction from biologics.
PART 7: TREATMENT ALGORITHM
DIAGNOSIS OF RA
↓
INITIATE MTX (first-line csDMARD) + folic acid
± bridging low-dose prednisone for rapid symptom control
↓
Reassess at 3 months (DAS28/CDAI)
↓
Target achieved? (DAS28 <2.6 or <3.2)
YES → continue and monitor every 3-6 months
NO → escalate
↓
Options when MTX inadequate:
1. Add another csDMARD (HCQ ± SSZ = "triple therapy")
2. Add biologic: TNF inhibitor (first choice) + MTX
or Abatacept + MTX
or Tocilizumab ± MTX
or JAK inhibitor
↓
If second biologic/JAK inhibitor fails:
→ Rituximab (especially if lymphoma history or seropositive)
→ Switch to different class biologic
PART 8: ROLE OF GLUCOCORTICOIDS
- Low dose prednisone (5-10 mg/day): Rapid symptom control when starting DMARDs; short-term use preferred
- Higher doses (0.5-1 mg/kg/day): Severe flares, extraarticular manifestations (vasculitis, pleuritis)
- Intra-articular corticosteroid: Excellent for isolated active joint flare
- Long-term use: Avoid if possible - osteoporosis, diabetes, hypertension, infection, adrenal suppression. If unavoidable (>3 months on ≥5 mg/day), start calcium + vitamin D and consider bisphosphonate for bone protection
PART 9: HIGH-YIELD MCQ SUMMARY
- ACR 2010 criteria score ≥6 = definite RA (max score 10)
- Most specific antibody for RA: Anti-CCP (ACPA) ~90% specific
- Anti-CCP positive = marker of erosive, aggressive disease
- DAS28 <2.6 = remission (target); reassess every 1-3 months in active disease
- First-line DMARD = Methotrexate (anchor drug); start 10-15 mg/week, escalate to 25 mg/week
- MTX must always be given with folic acid 1 mg/day
- MTX monitoring: CBC + LFTs + creatinine every 2-3 months
- MTX contraindications: Pregnancy (Category X), CrCl <30, dialysis, active liver disease, active serious infection
- Before biologics/JAK inhibitors: Screen for latent TB (IGRA/TST) + hepatitis B
- TNF inhibitors: Avoid in NYHA III/IV heart failure; avoid in demyelinating disease
- Hydroxychloroquine dose: ≤5 mg/kg/day; annual ophthalmology exam (OCT + visual fields)
- Leflunomide teratogenic: Cholestyramine washout before pregnancy
- JAK inhibitors: Oral; black box warning for VTE, CV events, malignancy
- Rituximab: Preferred if lymphoma history; screens for HBV reactivation
- Tocilizumab: Can be used as monotherapy; normalizes CRP (can mask disease monitoring)
- Steroids in RA: Bridge therapy only; not DMARDs; protect bone if long-term use
4/ osteoporosis meds, indication, doses, monitoring, duration of therapy, DEXA (to check BMD) when? WHO classification criteria? I'm gonna take mcq and short exam in hospital so as a mentor explain it and how can question asked
OSTEOPOROSIS - Complete Exam Guide
WHO Criteria, DEXA, Medications, Doses, Monitoring, Duration
HOW EXAMINERS THINK ABOUT THIS TOPIC
- "A 65-year-old woman, what do you do next?" → DEXA scan
- "T-score is -2.8, what do you start?" → Bisphosphonate
- "Patient on alendronate, what must you tell her?" → Take fasting, upright, wait 30 minutes
- "Which drug causes osteonecrosis of the jaw?" → Bisphosphonates / denosumab
- "Which drug is absolutely contraindicated in pregnancy?" → Bisphosphonates, denosumab
- "When do you stop a drug holiday from bisphosphonate?" → After 3-5 years for oral
PART 1: WHAT IS OSTEOPOROSIS?
Exam fact: Vertebral compression fractures are the most common osteoporotic fracture. Hip fractures cause the most morbidity and mortality (20-25% die within 1 year).
PART 2: WHO CLASSIFICATION CRITERIA (T-SCORE)
Understanding T-score vs Z-score
| Score | Compared Against | Used For |
|---|---|---|
| T-score | Young healthy adults (age 30, same sex) | Diagnose osteoporosis (postmenopausal women and men >50) |
| Z-score | Age- and sex-matched adults | Use in premenopausal women, men <50, children - to detect secondary causes |
Exam trap: T-score compares to YOUNG NORMAL adults. Z-score compares to AGE-MATCHED peers. Osteoporosis is defined by T-score, not Z-score. If a question asks about a 35-year-old, you use Z-score.
WHO T-Score Classification
| T-Score | Classification |
|---|---|
| ≥ -1.0 | Normal |
| -1.0 to -2.5 | Osteopenia (low bone mass) |
| ≤ -2.5 | Osteoporosis |
| ≤ -2.5 + fragility fracture | Severe osteoporosis |
Memory trick: "-2.5 is the cutoff for osteoporosis." If they give you -2.8, -3.0, -3.1 → osteoporosis. If they give you -1.5, -2.0, -2.3 → osteopenia.
Exam trap: Ward's triangle on DEXA appears as the lowest BMD area in the femoral head but is NOT used for diagnosis - it is a generated point, not an anatomical site. Use femoral neck, total hip, or lumbar spine.
PART 3: DEXA SCAN - WHEN TO ORDER?
Indications for DEXA (Screening)
- All women ≥65 years
- All men ≥70 years
- Postmenopausal women <65 with any major risk factor (below)
- Men age 50-69 with risk factors
- Any adult with a fragility fracture
- Adults on long-term glucocorticoids (≥5 mg prednisone/day for ≥3 months)
- Adults with secondary causes of bone loss (hyperparathyroidism, malabsorption, hypogonadism, RA, hyperthyroidism, multiple myeloma, COPD)
Major Risk Factors for Osteoporosis (NOF List - Exam Favourite)
- Age >65 (most important)
- Female sex and menopause
- Personal history of fragility fracture as adult
- First-degree relative with fragility fracture (especially maternal hip fracture)
- Low body weight (<127 lbs / ~58 kg)
- Current smoking
- Oral corticosteroid use >3 months
- Low calcium/vitamin D intake
- Estrogen deficiency (early menopause <45 years)
- Physical inactivity
- Excessive alcohol (>2 drinks/day)
Exam trap: Obesity is NOT a risk factor for osteoporosis. Osteoarthritis is NOT directly a risk factor. These are classic distractors.
FRAX Score
- WHO fracture risk assessment tool
- Calculates 10-year probability of major osteoporotic fracture (spine, hip, wrist, humerus) and hip fracture specifically
- Uses age, sex, BMI, fracture history, glucocorticoid use, RA, secondary causes ± femoral neck BMD
- Treatment is generally indicated when 10-year risk of major fracture ≥20% or hip fracture ≥3%
How Often to Repeat DEXA?
- Every 2 years when on treatment (to monitor response)
- Every 1-2 years in high-risk patients not yet on treatment
- Same machine, same technician where possible (machine variability is a known issue)
PART 4: WORKUP BEFORE STARTING TREATMENT
| Test | Rules Out |
|---|---|
| Serum calcium | Hyperparathyroidism (↑Ca), malnutrition (↓Ca) |
| PTH | Primary hyperparathyroidism |
| 25-OH Vitamin D | Vitamin D deficiency (very common; especially in elderly) |
| TSH | Hyperthyroidism |
| CBC | Multiple myeloma, anemia |
| Renal function (Cr) | CKD (different bone disease - renal osteodystrophy) |
| LFTs | Liver disease (reduced vitamin D activation) |
| 24-hr urine calcium | Hypercalciuria (<50 mg/day = malabsorption; >300 mg/day = renal leak/hypercalciuria) |
| Serum protein electrophoresis | Myeloma (especially in men) |
| Celiac serology (anti-tTG) | Malabsorption (low Z-score in young patient) |
| 24-hr urine cortisol or overnight dexamethasone suppression | Cushing's syndrome |
| Testosterone/FSH/LH | Hypogonadism (in men) |
PART 5: NON-PHARMACOLOGIC TREATMENT (ALWAYS FIRST)
- Calcium: Total intake 1000-1200 mg/day (dietary preferred); supplement the deficit
- Premenopausal women + men <50: 1000 mg/day
- Postmenopausal women + men >50: 1200 mg/day
- Take in divided doses ≤500 mg at a time (max absorption)
- Calcium carbonate: take with food (needs acid for absorption)
- Calcium citrate: can take without food (preferred in elderly, on PPIs)
-
Vitamin D: 800-1000 IU/day (some guidelines up to 2000 IU); target serum 25-OH D ≥30 ng/mL (≥75 nmol/L)
-
Weight-bearing exercise (walking, resistance training) - stimulates osteoblasts
-
Fall prevention: Remove home hazards, balance training, review medications causing dizziness (antihypertensives, sedatives, opioids)
-
Lifestyle: Stop smoking, limit alcohol, adequate protein intake
PART 6: PHARMACOLOGIC TREATMENT
When to Start Medication?
| Indication | Treatment Threshold |
|---|---|
| T-score ≤ -2.5 (osteoporosis) | Treat regardless of other risk factors |
| T-score -1.0 to -2.5 (osteopenia) + fragility fracture | Treat |
| T-score -1.0 to -2.5 (osteopenia) + FRAX ≥20% major fracture risk OR ≥3% hip fracture risk | Treat |
| Any fragility fracture (hip or spine) | Treat (by definition this is severe osteoporosis) |
| Long-term glucocorticoids (≥5 mg/day ≥3 months) | Treat per GIOP guidelines (lower T-score threshold of -1.5 in some guidelines) |
CLASS 1: BISPHOSPHONATES (First-Line Antiresorptives)
A. Alendronate (Fosamax) - Most Commonly Used Oral Bisphosphonate
| Details | |
|---|---|
| Indication | Treatment and prevention of postmenopausal osteoporosis; glucocorticoid-induced osteoporosis; osteoporosis in men |
| Dose (treatment) | 70 mg orally once weekly |
| Dose (prevention) | 35 mg orally once weekly |
| Administration | Take fasting (empty stomach), with a full glass of plain water (200-250 mL), in the morning |
| Remain upright (sitting or standing) for at least 30 minutes after | |
| Do NOT eat, drink (except water), or take other medications for 30 minutes after | |
| Duration | See "Drug Holiday" section below |
B. Risedronate (Actonel)
- 35 mg once weekly or 5 mg daily or 150 mg once monthly
- Same administration rules as alendronate (fasting, upright, 30 min wait)
- Slightly better GI profile than alendronate
C. Zoledronic Acid (Reclast) - IV Bisphosphonate
| Details | |
|---|---|
| Dose | 5 mg IV infusion once yearly (over ≥15 minutes) |
| Advantage | Best compliance (once yearly); effective in patients who cannot tolerate oral bisphosphonates or have GI disease/malabsorption |
| Side effect | Acute phase reaction (fever, myalgia, flu-like symptoms lasting 1-3 days after first infusion - give acetaminophen, ensure patient is well hydrated) |
| Precaution | Do NOT give if eGFR <35 mL/min (accumulates in kidney) |
D. Ibandronate
- 150 mg orally once monthly or 3 mg IV every 3 months
- Note: Proven only for vertebral fracture reduction, NOT hip fracture (important MCQ distinction)
BISPHOSPHONATE ADMINISTRATION RULES (Exam Favourite - Gets Asked Directly)
- Take on empty stomach, first thing in morning
- Full glass of water (not juice, coffee, or milk - impairs absorption)
- Remain upright (sitting or standing) for 30 minutes - prevents esophageal ulceration
- Wait 30 minutes before any food, drink, or other medications
- Do NOT crush or chew tablet
Why upright posture? Bisphosphonates are irritating to the esophagus. If the patient lies down after, reflux of drug → esophageal ulceration/stricture. This is the most important counselling point.
BISPHOSPHONATE MONITORING
| What | When | Why |
|---|---|---|
| DEXA scan | Baseline; repeat every 2 years on treatment | Monitor BMD response |
| Serum creatinine | Baseline; before each IV dose (for zoledronic acid); periodically | Renal clearance; avoid in eGFR <30-35 |
| Serum calcium + vitamin D | Baseline; especially before IV bisphosphonate | Must correct hypocalcemia before treatment; adequate Ca/VitD required |
| Dental exam | Before starting (especially for IV bisphosphonates at high doses) | Osteonecrosis of the jaw risk |
| Bone markers (CTX, NTX) | Optional; can confirm adherence and response | Reduced CTX indicates antiresorptive effect |
| Symptoms of atypical femoral fracture | Each visit (ask about thigh/groin pain) | Rare but serious complication of long-term use |
| Esophageal symptoms | Each visit (for oral bisphosphonates) | Esophagitis, ulceration |
BISPHOSPHONATE SIDE EFFECTS (Exam High-Yield)
| Side Effect | Drug | Notes |
|---|---|---|
| Esophagitis/esophageal ulceration | Oral bisphosphonates | Prevented by upright posture + water; contraindicated in esophageal stricture, achalasia |
| Acute phase reaction | IV zoledronic acid (first dose) | Fever, myalgia, headache - 1-3 days; give pre-hydration + acetaminophen |
| Osteonecrosis of the jaw (ONJ) | All bisphosphonates (especially IV/high dose) | Rare in osteoporosis doses; higher risk with dental procedures, poor dental hygiene, cancer doses |
| Atypical femoral fracture | Long-term oral bisphosphonates (>5 years) | Subtrochanteric/femoral shaft stress fracture; presents with prodromal thigh pain; bilateral in 25% |
| Hypocalcemia | IV bisphosphonates | Ensure calcium/vitamin D replete before giving |
| Renal impairment | IV zoledronic acid especially | Avoid if eGFR <35 |
BISPHOSPHONATE DRUG HOLIDAY (Critical Concept)
| Drug | When to Consider Holiday | Holiday Duration |
|---|---|---|
| Oral (alendronate, risedronate) | After 3-5 years in low-to-moderate risk | 2-3 years off |
| IV zoledronic acid | After 3 years in low-moderate risk; 6 years in high risk | Monitor DEXA/markers; restart if BMD falls |
Do NOT take a holiday if: History of hip or vertebral fracture, very low T-score (< -3.0), on glucocorticoids, high fracture risk.
BISPHOSPHONATE CONTRAINDICATIONS
- eGFR <30-35 mL/min
- Hypocalcemia (must correct first)
- Esophageal abnormalities (achalasia, stricture - for oral only)
- Pregnancy and breastfeeding (accumulate in bone, potential fetal harm)
CLASS 2: DENOSUMAB (Prolia)
| Details | |
|---|---|
| Indication | Postmenopausal osteoporosis; osteoporosis in men; glucocorticoid-induced osteoporosis; preferred when eGFR <30 (safe in CKD unlike bisphosphonates) |
| Dose | 60 mg SC injection every 6 months |
| Advantages | No renal dose adjustment; greater BMD increase than bisphosphonates; SC injection (not swallowing large pills) |
| Critical danger on stopping | REBOUND bone loss - if denosumab is stopped abruptly, bone turnover surges above baseline → rapid BMD loss and increased vertebral fracture risk (multiple vertebral fractures can occur). Must transition to a bisphosphonate when stopping denosumab |
- Serum calcium (risk of hypocalcemia, especially in CKD; ensure Ca + VitD sufficient)
- DEXA every 2 years
- Dental health (ONJ risk - same as bisphosphonates)
- Signs of infection (immunosuppressive effect; increased cellulitis, serious skin infections)
- Atypical femoral fracture risk (similar to bisphosphonates)
- Hypocalcemia (especially in CKD - must pre-treat with calcium/VitD)
- Increased serious infections (cellulitis - particularly of skin)
- ONJ
- Atypical femoral fracture
- Rebound vertebral fractures on discontinuation (most important)
Exam trap: "What happens if you stop denosumab?" = Rebound fracture risk. Always transition to bisphosphonate when stopping. This is a frequently asked question.
CLASS 3: TERIPARATIDE AND ABALOPARATIDE (Anabolic/Bone-Building Agents)
- Teriparatide = recombinant PTH(1-34) - stimulates osteoblasts (bone formation); also increases calcium absorption
- Abaloparatide = synthetic PTHrP analogue - similar anabolic mechanism; less hypercalcemia
| Teriparatide | |
|---|---|
| Indication | Severe osteoporosis (T-score ≤ -3.0 or fracture + T-score ≤ -2.5); failed antiresorptive therapy; glucocorticoid-induced osteoporosis at very high fracture risk |
| Dose | 20 mcg SC injection once daily |
| Duration | Maximum 2 years (lifetime; cannot restart) |
| After stopping | Must transition to an antiresorptive (bisphosphonate or denosumab) immediately, otherwise BMD gain is lost |
| Contraindications | Paget's disease; prior radiation therapy to bone; hypercalcemia; bone malignancy or metastases; Paget's disease; history of radiation therapy; not in children/adolescents (open growth plates) |
- Serum calcium (can cause hypercalcemia)
- Serum phosphate and uric acid
- Renal function
- DEXA (can be done 12-18 months into therapy to assess response)
Historical note: Previous animal studies showed osteosarcoma at very high doses, which led to the 2-year lifetime limit and contraindication in patients with bone malignancy. This is a classic MCQ point.
CLASS 4: ROMOSOZUMAB (Evenity) - Dual-Action
| Details | |
|---|---|
| Dose | 210 mg SC once monthly x 12 months only |
| Indication | Severe postmenopausal osteoporosis at very high fracture risk; after bisphosphonate failure |
| After stopping | Must transition to antiresorptive (bisphosphonate) |
| Black box warning | Increased risk of MI and stroke - contraindicated in patients who have had MI or stroke in the past year |
CLASS 5: SERMs (Selective Estrogen Receptor Modulators)
- Dose: 60 mg/day orally
- Acts as estrogen agonist in bone (preserves BMD) but estrogen antagonist in breast and uterus
- Reduces vertebral fractures by 30-50%; does NOT reduce hip fracture risk
- Also reduces invasive breast cancer risk ~65% (dual benefit)
- Does NOT cause uterine cancer (unlike tamoxifen)
- Side effects: Hot flashes (estrogenic); DVT/PE (increased risk - avoid in immobile patients); possible increased stroke risk in elderly
- Avoid in women >70 (stroke risk)
- NOT used in women with bothersome menopausal symptoms (worsens hot flashes)
CLASS 6: HORMONE REPLACEMENT THERAPY (HRT/MHT)
- Estrogen ± progesterone
- Effective for prevention of postmenopausal bone loss and fracture
- Not first-line for osteoporosis treatment due to cardiovascular/breast cancer risks
- Role: Women with menopausal symptoms + osteoporosis prevention; benefit outweighs risk in younger postmenopausal women (<60 years or within 10 years of menopause)
PART 7: GLUCOCORTICOID-INDUCED OSTEOPOROSIS (GIOP) - Exam Favourite
When to Give Bone Protection?
- Prednisone ≥5 mg/day expected duration ≥3 months
- Lower threshold if additional risk factors present
- Calcium 1200 mg/day + Vitamin D 800-1000 IU/day - everyone on chronic steroids
- Oral bisphosphonate (alendronate 70 mg/week or risedronate 35 mg/week) - if treatment threshold met
- Consider teriparatide if very high fracture risk (T-score < -3.5 or fracture)
- Monitor DEXA annually during steroid therapy
Exam tip: A patient being started on long-term prednisone for RA or IBD or COPD - what do you prescribe? → Calcium + Vitamin D + consider bisphosphonate based on DEXA/FRAX.
PART 8: DRUG COMPARISON TABLE (Quick Reference)
| Drug | Mechanism | Route | Key Side Effect | Max Duration |
|---|---|---|---|---|
| Alendronate | Inhibits osteoclasts | Oral weekly | Esophagitis | 3-5 years then holiday |
| Risedronate | Inhibits osteoclasts | Oral weekly/monthly | Esophagitis (less than alendronate) | 3-5 years |
| Zoledronic acid | Inhibits osteoclasts | IV yearly | Acute phase reaction | 3-6 years then holiday |
| Denosumab | Anti-RANKL | SC every 6 months | Hypocalcemia; rebound fractures on stopping | Indefinite (but plan exit) |
| Teriparatide | Stimulates osteoblasts (PTH analogue) | SC daily | Hypercalcemia | 2 years max |
| Romosozumab | Anti-sclerostin (dual action) | SC monthly | MI/stroke risk | 12 months |
| Raloxifene | SERM (estrogen agonist in bone) | Oral daily | Hot flashes; DVT | Long-term |
| Estrogen (HRT) | Prevents osteoclast activation | Oral/patch/gel | DVT, breast cancer | Shortest effective duration |
PART 9: HOW QUESTIONS ARE ASKED - MENTOR TIPS
MCQ Pattern 1: "T-score question"
MCQ Pattern 2: "When to screen?"
MCQ Pattern 3: "Drug of choice"
MCQ Pattern 4: "Side effect/counselling"
MCQ Pattern 5: "Hip vs vertebral fracture"
Short Answer Pattern
PART 10: HIGH-YIELD EXAM SUMMARY (Final Rapid Review)
| Fact | Answer |
|---|---|
| Gold standard test for BMD | Central DEXA |
| T-score for osteoporosis | ≤ -2.5 |
| T-score for osteopenia | -1.0 to -2.5 |
| T-score for normal | ≥ -1.0 |
| Score used in premenopausal/young | Z-score |
| Universal screening age (women) | ≥65 years |
| Most common osteoporotic fracture | Vertebral |
| Most lethal osteoporotic fracture | Hip (20-25% die in 1 year) |
| First-line pharmacotherapy | Bisphosphonate (alendronate) |
| Bisphosphonate key instruction | Fasting, full water, upright 30 min |
| Bisphosphonate for eGFR <30 | Contraindicated - use denosumab |
| Drug holiday for oral bisphosphonate | After 3-5 years |
| Teriparatide max duration | 2 years (lifetime) |
| After stopping teriparatide | Give antiresorptive immediately |
| After stopping denosumab | Give bisphosphonate to prevent rebound |
| Romosozumab warning | MI/stroke - avoid if recent CV event |
| Raloxifene: fractures prevented | Vertebral only (NOT hip) |
| Raloxifene bonus benefit | Reduces breast cancer risk |
| Raloxifene risk | DVT/PE |
| ONJ risk drugs | Bisphosphonates + denosumab |
| GIOP prevention threshold | ≥5 mg/day prednisone for ≥3 months |
Do it again
Do OSTEOPOROSIS again
🦴 OSTEOPOROSIS - Complete Exam Guide (Rebuilt)
SECTION 1: DEFINITION AND BASICS
- Classic sites: vertebral body, hip (proximal femur), distal radius (Colles'), proximal humerus
- Excludes: fingers, toes, skull, face fractures
- Most common osteoporotic fracture = vertebral (but >70% are asymptomatic/incidental)
- Most deadly osteoporotic fracture = hip (20-25% mortality within 1 year; 30% need long-term care)
-
50% of all fractures occur in people with osteopenia (T-score -1.0 to -2.5), not osteoporosis - hence why FRAX matters
- Lifetime fracture risk for Caucasian woman reaching age 50 = ~50%
SECTION 2: WHO CLASSIFICATION (THE #1 MCQ TABLE)
T-score vs Z-score - Understand This First
| Score Type | Compared To | Use It For |
|---|---|---|
| T-score | Young healthy adults, age 30, same sex | Postmenopausal women, men ≥50 |
| Z-score | Age- and sex-matched peers | Premenopausal women, men <50, children |
Exam trap #1: A 38-year-old woman with Z-score -2.8 → you use Z-score (not T-score) because she is premenopausal and <50. A Z-score ≤ -2.0 = "below expected range for age" → investigate for secondary cause.
WHO T-Score Classification Table
| T-Score | Diagnosis |
|---|---|
| ≥ -1.0 | Normal |
| -1.0 to -2.5 (not including -2.5) | Osteopenia (low bone mass) |
| ≤ -2.5 | Osteoporosis |
| ≤ -2.5 + fragility fracture | Severe osteoporosis |
Exam trap #2: "Between -1.0 and -2.5" means the number is more negative than -1.0 but less negative than -2.5. So -1.5, -2.0, -2.3 = osteopenia. -2.5, -2.8, -3.0 = osteoporosis.
Exam trap #3: Ward's triangle on DEXA shows the lowest BMD area but is NOT an anatomical site and NOT used for diagnosis. Use: lumbar spine, femoral neck, or total hip.
Exam trap #4: Use the lowest T-score from any measured site to make the diagnosis.
SECTION 3: DEXA SCAN - WHEN, HOW, HOW OFTEN
Do NOT use for diagnosis:
- Peripheral DEXA (pDEXA) - screening only
- Quantitative ultrasound (QUS) - screening only
- Quantitative CT (QCT) - more radiation, not standard
- Plain X-ray - insensitive (only detects loss >30%)
Indications for DEXA (When to Order)
- All women ≥ 65 years
- All men ≥ 70 years
- Postmenopausal women < 65 with ≥1 risk factor
- Men 50-69 with risk factors
- Any fragility fracture in adults (any age) → get DEXA
- Long-term glucocorticoids (≥5 mg prednisone/day for ≥3 months)
- Secondary causes of bone loss (see below)
Secondary Causes of Osteoporosis (Must Know for MCQs)
| Endocrine | Medications | GI/Other |
|---|---|---|
| Hyperparathyroidism | Glucocorticoids (most common drug cause) | Celiac disease / malabsorption |
| Hyperthyroidism | GnRH agonists | Inflammatory bowel disease |
| Hypogonadism / low testosterone | Anticonvulsants | Multiple myeloma |
| Cushing's syndrome | Aromatase inhibitors | RA, COPD |
| Diabetes (types 1 and 2) | Heparin (long-term) | Anorexia nervosa |
Exam tip: Obesity is NOT a risk factor for osteoporosis. Osteoarthritis is NOT a direct risk factor. Classic distractors.
Major Risk Factors (NOF/USPSTF List)
- Age > 65 (strongest)
- Female sex, postmenopausal
- Personal fragility fracture as adult
- First-degree relative with hip fracture
- Low body weight (<58 kg / 127 lbs)
- Current smoking
- Oral corticosteroids >3 months
- Low calcium/Vitamin D
- Early menopause (<45 years)
- Alcohol >2 drinks/day
- Physical inactivity
How Often to Repeat DEXA?
- On treatment: every 1-2 years
- Not on treatment, moderate risk: every 2 years
- Always use same machine, same technician (minimize variability)
FRAX Tool
- Calculates 10-year probability of major osteoporotic fracture + hip fracture
- Uses: age, sex, BMI, prior fracture, parental hip fracture, glucocorticoids, RA, secondary causes ± femoral neck BMD
- Treat if: 10-year major fracture risk ≥20% OR 10-year hip fracture risk ≥3% (even if T-score is only osteopenic)
SECTION 4: WORKUP BEFORE TREATMENT
| Test | Purpose |
|---|---|
| Serum calcium, phosphate | Hyperparathyroidism, hypocalcemia |
| Serum PTH | Primary hyperparathyroidism (high PTH + high Ca) |
| 25-OH Vitamin D | Deficiency (most common finding - target ≥30 ng/mL) |
| TSH | Hyperthyroidism |
| CBC | Myeloma (anemia), marrow disorders |
| Creatinine/eGFR | CKD-MBD (different disease, different treatment) |
| LFTs | Liver disease |
| 24-hr urine calcium | <50 mg = malnutrition/malabsorption; >300 mg = hypercalciuria |
| Testosterone (men) | Hypogonadism |
| SPEP / serum free light chains | Myeloma ("punched-out" lesions on X-ray) |
| 24-hr urine cortisol / overnight dexamethasone suppression | Cushing's syndrome |
| Anti-tTG (celiac serology) | Malabsorption in young patients with unexpectedly low Z-scores |
SECTION 5: NON-PHARMACOLOGIC (NEVER SKIP THIS IN EXAMS)
- Calcium supplementation:
- Total intake goal: 1200 mg/day (postmenopausal women + men >50)
- Take in divided doses ≤500 mg (maximal absorption per dose)
- Calcium carbonate: Take with food (needs acid)
- Calcium citrate: Take with or without food (preferred in elderly, PPIs users, achlorhydria)
-
Vitamin D: 800-1000 IU/day; maintain serum 25-OH D ≥30 ng/mL
-
Weight-bearing + resistance exercise (walking, weights, Tai Chi)
-
Fall prevention: Remove rugs/hazards, adequate lighting, balance training, review medications (antihypertensives, sedatives, opioids - all increase fall risk)
-
Lifestyle: Stop smoking, limit alcohol, adequate protein
SECTION 6: PHARMACOLOGIC TREATMENT
When to Start Medication?
| Clinical Scenario | Action |
|---|---|
| T-score ≤ -2.5 | Treat |
| T-score -1.0 to -2.5 + fragility fracture | Treat |
| T-score -1.0 to -2.5 + FRAX ≥20% major fracture or ≥3% hip fracture | Treat |
| Any hip or vertebral fragility fracture | Treat (by definition severe osteoporosis) |
| Glucocorticoids ≥5 mg/day ≥3 months | Give Ca+VitD ± bisphosphonate |
DRUG CLASS 1: BISPHOSPHONATES (First-Line)
- Alendronate/risedronate/zoledronic acid: reduce vertebral fracture ~50%, hip fracture ~40-50%
- Ibandronate: reduces vertebral fracture only (no proven hip fracture reduction - EXAM TRAP)
A. ALENDRONATE (Fosamax) - Most Commonly Tested
| Parameter | Details |
|---|---|
| Indication | Treatment of postmenopausal osteoporosis; osteoporosis in men; GIOP |
| Dose (treatment) | 70 mg orally once weekly |
| Dose (prevention) | 35 mg orally once weekly |
| How to take | Fasting, first thing in morning, full glass plain water (200 mL), upright ≥30 min, no food/drink/meds for 30 min |
| Duration | 3-5 years → reassess for drug holiday |
| Monitoring | DEXA every 1-2 years; creatinine; calcium/Vit D levels; symptoms |
B. RISEDRONATE (Actonel)
| Parameter | Details |
|---|---|
| Dose | 35 mg once weekly or 5 mg daily or 150 mg once monthly |
| Same administration rules as alendronate | Fasting, upright, 30 min |
| Advantage | Slightly better GI tolerability than alendronate |
C. ZOLEDRONIC ACID (Reclast/Aclasta) - IV
| Parameter | Details |
|---|---|
| Indication | Cannot tolerate oral bisphosphonate; malabsorption; high compliance concern |
| Dose | 5 mg IV infusion once yearly (over ≥15 minutes) |
| Key pre-requirement | Ensure adequately hydrated; correct hypocalcemia + Vit D first |
| Side effect (unique) | Acute phase reaction - fever, myalgia, headache, arthralgia after first dose (1-3 days). Give acetaminophen + ensure hydration |
| Renal caution | Do NOT give if eGFR < 35 mL/min |
D. IBANDRONATE
| Parameter | Details |
|---|---|
| Dose | 150 mg orally once monthly or 3 mg IV every 3 months |
| Critical limitation | Proven only for vertebral fractures - NO data for hip fracture prevention |
| Same oral administration rules apply | Fasting, upright, 30 min |
BISPHOSPHONATE ADMINISTRATION - THE EXAM'S FAVOURITE COUNSELLING QUESTION
Q: "What instructions do you give a patient starting oral bisphosphonate?"
- Take first thing in the morning, on an empty stomach
- Use a full glass (200-250 mL) of plain water only - NOT coffee, juice, or milk (impairs absorption)
- Do NOT eat, drink anything other than water, or take any other medication for 30 minutes
- Remain sitting upright or standing for at least 30 minutes (prevents esophageal irritation from drug reflux)
- Do NOT crush or chew the tablet
Why upright? Bisphosphonates are caustic to the esophagus. Lying down → reflux → esophageal ulcer → stricture.
BISPHOSPHONATE SIDE EFFECTS (Exam High-Yield)
| Side Effect | Drug | Exam Point |
|---|---|---|
| Esophagitis, esophageal ulceration | All oral bisphosphonates | Prevented by administration rules; contraindicate in esophageal stricture/achalasia |
| Acute phase reaction (flu-like) | IV zoledronic acid, 1st dose | Give paracetamol + hydration; resolves 1-3 days |
| Osteonecrosis of the jaw (ONJ) | All bisphosphonates + denosumab | More common with IV/high dose; risk with dental procedures; do dental check before starting |
| Atypical femoral fracture | Long-term use >3-5 years | Subtrochanteric/diaphyseal stress fracture; prodromal thigh/groin pain; bilateral 25%; STOP bisphosphonate if suspected |
| Hypocalcemia | IV bisphosphonates especially | Must correct Ca + VitD deficiency before giving IV |
| Nephrotoxicity | IV zoledronic acid | Avoid eGFR <35 |
BISPHOSPHONATE DRUG HOLIDAY - FREQUENTLY TESTED
| Drug | Start Holiday After | Holiday Duration |
|---|---|---|
| Oral (alendronate, risedronate) | 3-5 years (low-moderate risk) | 2-3 years - monitor DEXA/markers; restart if significant BMD loss |
| IV zoledronic acid | 3 years (low risk); 6 years (high risk) | Same monitoring approach |
- Prior hip or vertebral fracture
- T-score ≤ -3.0
- On chronic glucocorticoids
- Very high FRAX risk
BISPHOSPHONATE CONTRAINDICATIONS
- eGFR <30 mL/min (oral) or <35 mL/min (IV zoledronic)
- Uncorrected hypocalcemia (correct first)
- Esophageal abnormalities (stricture, achalasia) - oral only
- Inability to sit/stand upright for 30 min - oral only
- Pregnancy (Category C/D; accumulate in fetal bone)
DRUG CLASS 2: DENOSUMAB (Prolia)
| Parameter | Details |
|---|---|
| Mechanism | Monoclonal antibody against RANKL → inhibits osteoclast formation and activation |
| Dose | 60 mg SC injection every 6 months |
| Indication | Postmenopausal osteoporosis; men; GIOP; preferred when eGFR <30 (safe in CKD unlike bisphosphonates) |
| Advantage | Most potent BMD increase of all antiresorptives; safe in renal failure; no GI issues |
| Duration | Can be used long-term; no maximum defined - but must plan exit strategy |
DENOSUMAB UNIQUE DANGER - THE REBOUND EFFECT (Exam Favourite)
Q: "What must you do when stopping denosumab?"
Denosumab Monitoring
| What | Why |
|---|---|
| Serum calcium (before each dose) | Hypocalcemia - especially dangerous in CKD; give Ca + VitD before each injection |
| DEXA every 1-2 years | Monitor BMD response |
| Dental health | ONJ risk (same as bisphosphonates) |
| Signs of infection | Denosumab suppresses RANKL in immune cells too → increased serious skin infections (cellulitis) |
| Atypical femoral fracture | Similar risk to bisphosphonates with long-term use |
DRUG CLASS 3: TERIPARATIDE (Forteo) - Anabolic
| Parameter | Details |
|---|---|
| Mechanism | Recombinant human PTH(1-34) - stimulates osteoblasts (bone formation). When given as intermittent (not continuous) PTH → net anabolic effect |
| Dose | 20 mcg SC once daily |
| Indication | Severe osteoporosis (T-score ≤ -3.0 or fracture + T ≤ -2.5); failed antiresorptive therapy; very high fracture risk glucocorticoid-induced osteoporosis |
| Maximum duration | 2 years lifetime (cannot restart; cannot give a second course) |
| After stopping | MUST immediately start antiresorptive (bisphosphonate or denosumab) or all the BMD gain is lost |
Teriparatide Contraindications (Exam High-Yield)
| Contraindication | Reason |
|---|---|
| Paget's disease of bone | Abnormal bone remodeling - risk of osteosarcoma |
| Prior radiation therapy to bone | Increased osteosarcoma risk |
| Bone malignancy or metastases | Same reason |
| Open growth plates (children/adolescents) | Not established in pediatric patients |
| Hypercalcemia | Teriparatide raises serum calcium |
Historical MCQ trap: Teriparatide carries an osteosarcoma warning from rat studies at very high doses. This led to the 2-year lifetime limit and the list of contraindications above. The actual osteosarcoma risk in humans is extremely low, but this warning is tested in MCQs.
Teriparatide Monitoring
- Serum calcium (hypercalcemia, hypercalciuria)
- Serum phosphate, uric acid
- Renal function
- DEXA at 12-18 months into treatment
- Bone formation marker: P1NP (rises rapidly after starting - confirms response)
DRUG CLASS 4: ABALOPARATIDE (Tymlos)
- Synthetic PTHrP analogue (parathyroid hormone-related protein)
- Similar mechanism to teriparatide (anabolic)
- Dose: 80 mcg SC daily
- Maximum: 18-24 months
- Slightly less hypercalcemia than teriparatide
- Must follow with antiresorptive on stopping
DRUG CLASS 5: ROMOSOZUMAB (Evenity) - Dual Action
| Parameter | Details |
|---|---|
| Mechanism | Monoclonal antibody against sclerostin → removes the brake on bone formation AND reduces bone resorption simultaneously (dual effect) |
| Dose | 210 mg SC once monthly x 12 months only |
| Indication | Severe postmenopausal osteoporosis at very high fracture risk; after bisphosphonate failure |
| After stopping | Transition to antiresorptive (bisphosphonate) |
| BLACK BOX WARNING | Increased MI and stroke risk - contraindicated in patients who had MI or stroke in the past year |
MCQ trap: "Which osteoporosis drug is contraindicated in patients with recent cardiovascular events?" → Romosozumab
DRUG CLASS 6: RALOXIFENE (Evista) - SERM
| Parameter | Details |
|---|---|
| Mechanism | Selective Estrogen Receptor Modulator - estrogen agonist in bone (preserves BMD), estrogen antagonist in breast and uterus |
| Dose | 60 mg orally once daily |
| Fractures prevented | Vertebral fractures reduced 30-50%; does NOT reduce hip fracture |
| Bonus benefit | Reduces invasive breast cancer risk ~65% (ER-positive); FDA approved for breast cancer prevention |
| Does NOT cause | Uterine cancer (unlike tamoxifen - important MCQ distinction) |
| Side effects | Hot flashes (worsens menopausal symptoms); DVT/PE (contraindicated in immobile patients); increased stroke risk in elderly |
| Avoid | Women >70 (stroke risk); women with bothersome hot flashes (makes them worse); history of DVT |
Exam trap: "Which osteoporosis drug also prevents breast cancer?" → Raloxifene. "Does it prevent hip fractures?" → NO - vertebral only.
DRUG CLASS 7: HORMONE REPLACEMENT THERAPY (HRT/MHT)
- Estrogen ± progesterone
- Effective for prevention of bone loss, reduces fracture risk
- Not recommended as primary osteoporosis treatment (cardiovascular + breast cancer risks from WHI trial)
- Role: Women with menopausal symptoms + bone protection in early menopause (<60 years or within 10 years of menopause) - benefit may outweigh risk in this group
DRUG CLASS 8: CALCITONIN
- Salmon calcitonin nasal spray (200 IU/day) or SC
- Weak antiresorptive; modest BMD effect
- Main current use: pain relief from acute vertebral compression fractures (modest analgesic effect)
- Largely replaced by more effective agents
- Not recommended as primary treatment in most current guidelines
SECTION 7: GLUCOCORTICOID-INDUCED OSTEOPOROSIS (GIOP)
| Situation | Action |
|---|---|
| Starting prednisone ≥5 mg/day for expected ≥3 months | Give Ca 1200 mg/day + Vit D 800-1000 IU/day |
| DEXA T-score ≤ -2.5 OR fragility fracture | Add oral bisphosphonate (alendronate 70 mg/week) |
| T-score -1.0 to -2.5 + high FRAX risk | Add oral bisphosphonate |
| Very high risk (T-score ≤ -3.5, prior vertebral fracture) | Consider teriparatide (superior to bisphosphonates in GIOP) |
| Monitoring | DEXA annually while on steroids |
MCQ: "A patient is started on prednisone 20 mg/day for SLE. What do you prescribe for bone protection?" Answer: Calcium 1200 mg/day + Vitamin D 800-1000 IU/day + bisphosphonate (alendronate 70 mg/week) if treatment threshold met. Get baseline DEXA.
SECTION 8: MONITORING ALL OSTEOPOROSIS DRUGS (Master Table)
| Drug | Pre-Treatment | Ongoing Monitoring | Key Specific Issue |
|---|---|---|---|
| Oral bisphosphonates | Creatinine; Ca/VitD; dental exam; DEXA | DEXA q1-2yr; creatinine; GI symptoms | Drug holiday at 3-5 years |
| Zoledronic acid | Creatinine (eGFR >35 required); Ca/VitD; dental; DEXA | DEXA q1-2yr; creatinine before each dose; acute reaction after 1st dose | Once-yearly infusion |
| Denosumab | Ca/VitD; dental; DEXA | Serum calcium before each dose (hypocalcemia); DEXA q1-2yr; infections | Plan exit - transition to bisphosphonate |
| Teriparatide | Serum Ca; creatinine; DEXA; rule out contraindications | Serum Ca; DEXA at 12-18 months; P1NP (optional - bone formation marker) | 2-year max lifetime; follow with antiresorptive |
| Romosozumab | CV history (MI/stroke); Ca/VitD | Serum Ca; DEXA; CV symptoms | 12 months only; avoid if recent MI/stroke |
| Raloxifene | Hx DVT/PE; CV risk | No specific labs; watch for DVT symptoms | Annual mammogram |
SECTION 9: DURATION OF THERAPY - SIMPLIFIED
| Drug | Duration | Then What? |
|---|---|---|
| Alendronate/Risedronate | 3-5 years → drug holiday 2-3 years | Restart if BMD falls or fracture |
| Zoledronic acid | 3-6 years → holiday | Same |
| Denosumab | Indefinite, but plan exit | Transition to bisphosphonate when stopping |
| Teriparatide | Max 2 years, lifetime | Immediately start bisphosphonate/denosumab |
| Abaloparatide | Max 18-24 months | Immediately start antiresorptive |
| Romosozumab | Exactly 12 months | Start bisphosphonate |
| Raloxifene | Long-term (years) as tolerated | Can continue; reassess risk/benefit |
SECTION 10: TREATMENT ALGORITHM (Clean Version)
STEP 1 → Calcium 1200 mg/day + Vitamin D 800-1000 IU/day
+ fall prevention + weight-bearing exercise (ALL patients)
STEP 2 → Decide on drug therapy:
T-score ≤ -2.5 OR fragility fracture OR FRAX ≥20%/≥3%?
YES → START PHARMACOTHERAPY
STEP 3 → Choose drug based on patient:
Standard postmenopausal osteoporosis:
→ First line: BISPHOSPHONATE (alendronate 70mg/wk oral OR zoledronic acid 5mg IV/yr)
CKD (eGFR <30-35):
→ DENOSUMAB 60mg SC every 6 months (safe in CKD)
Severe osteoporosis (T ≤ -3.0, multiple fractures, failed antiresorptive):
→ TERIPARATIDE 20mcg SC daily (max 2 years) → then bisphosphonate
Very high risk + intolerant to bisphosphonates, no recent MI/stroke:
→ ROMOSOZUMAB 210mg SC monthly x 12 months → then bisphosphonate
Younger postmenopausal + menopausal symptoms:
→ HRT (estrogen ± progesterone)
Vertebral fracture only + breast cancer risk:
→ RALOXIFENE 60mg daily
STEP 4 → Monitor: DEXA q1-2 years; bone markers (optional); drug-specific monitoring
STEP 5 → Reassess at 3-5 years:
Good response + low ongoing risk → drug holiday (bisphosphonates)
Poor response → switch drug class or add anabolic
SECTION 11: MCQ PATTERNS AND EXAM TRAPS
Pattern 1: T-score Identification
Pattern 2: When to screen
Pattern 3: Which drug?
Pattern 4: Drug counselling
Pattern 5: Drug-specific side effects
Pattern 6: Glucocorticoid-induced osteoporosis
Pattern 7: Teriparatide rules
SECTION 12: FINAL RAPID RECALL TABLE
| Fact | Answer |
|---|---|
| Gold standard BMD test | Central DEXA |
| T-score = osteoporosis | ≤ -2.5 |
| T-score = osteopenia | -1.0 to -2.5 |
| T-score = normal | ≥ -1.0 |
| Severe osteoporosis | ≤ -2.5 + fragility fracture |
| T-score used in | Postmenopausal women, men ≥50 |
| Z-score used in | Premenopausal women, men <50 |
| Universal DEXA screening age (women) | ≥65 |
| FRAX treatment threshold | Major fracture ≥20% OR hip ≥3% |
| Most common osteoporotic fracture | Vertebral (70% asymptomatic) |
| Most deadly fracture | Hip (20-25% mortality/year) |
| First-line drug | Bisphosphonate |
| Bisphosphonate key instruction | Fasting, full water, upright 30 min |
| Bisphosphonate drug holiday | After 3-5 years |
| Bisphosphonate + eGFR <30 | Contraindicated |
| Drug for CKD eGFR <30 | Denosumab |
| Denosumab on stopping | Must give bisphosphonate (rebound risk) |
| Teriparatide max duration | 2 years lifetime |
| After teriparatide | Start antiresorptive immediately |
| Teriparatide contraindication | Paget's, bone XRT, malignancy, hypercalcemia |
| Romosozumab duration | 12 months only |
| Romosozumab warning | MI / stroke |
| Raloxifene fractures | Vertebral only (NOT hip) |
| Raloxifene bonus | Reduces breast cancer |
| Raloxifene risk | DVT/PE |
| ONJ risk drugs | Bisphosphonates + denosumab |
| Atypical femoral fracture | Bisphosphonates long-term; prodromal thigh pain |
| GIOP prevention | ≥5 mg/day prednisolone ≥3 months → Ca + VitD ± bisphosphonate |
| GIOP severe → use | Teriparatide (superior to bisphosphonates) |
| Calcium carbonate → take | With food (needs acid) |
| Calcium citrate → take | With or without food |