Various cysts of the ovary Pathology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have all the content needed for a comprehensive answer. Let me compile the full pathology overview.
Cysts of the Ovary - Pathology
Ovarian cysts are the most common cause of gynecologic masses. They occur at any stage of life but are most frequent in the reproductive years because of cyclic ovarian changes associated with menstruation. Most are benign and resolve without intervention, though some may be malignant or complicated by hemorrhage or torsion. - Rosen's Emergency Medicine
Classification
Ovarian cysts fall into two broad categories:
1. Non-neoplastic (Functional / Reactive) Cysts
2. Neoplastic Cysts (benign, borderline, or malignant)
I. Non-Neoplastic (Functional) Cysts
These are the most common type. All are benign and usually do not require surgical management.
1. Follicular Cyst
- Most common functional cyst
- Arises from a Graafian follicle that fails to rupture or regress
- Defined as pathologic when diameter exceeds 3 cm; rarely larger than 8 cm
- Gross: Thin-walled, unilocular, filled with clear serous fluid
- Micro: Lined by granulosa cells (inner) and theca cells (outer); if large, the epithelium may be flattened or absent
- Clinical: Usually asymptomatic; may rupture causing transient pelvic pain or dyspareunia; rarely associated with hemorrhage
- Resolution: Typically within 4-8 weeks with expectant management
- Cigarette and marijuana smoking increase risk; oral contraceptives reduce risk
2. Corpus Luteum Cyst
- Less common than follicular cysts
- Forms when the corpus luteum fails to regress after ovulation, or persists after conception
- Gross: Often filled with hemorrhagic (blood-stained) fluid; thick yellow-orange wall (due to luteinization)
- Micro: Lined by large luteinized granulosa cells and theca-lutein cells
- Clinical: May range from asymptomatic to chronic dull pelvic pain; rupture can cause significant hemoperitoneum (more so than follicular cyst)
- Ruptures more commonly on the right side, often on cycle days 20-26; may be triggered by intercourse, trauma, or pelvic examination
- Patients on anticoagulants are at particular risk for hemorrhage
3. Theca-Lutein Cysts
- Least common functional cyst
- Typically bilateral and multiple
- Caused by excessive hCG stimulation of the theca-lutein cells
- Associated with: molar pregnancy, choriocarcinoma, multiple gestations, ovulation induction drugs (clomiphene, hMG-hCG), GnRH analogs
- Up to one-quarter of complete molar pregnancies have theca-lutein cysts
- Regress spontaneously once the hCG stimulus is removed
- Gross: Often large, multilocular, bilateral; pale yellow walls
II. Neoplastic Cysts
WHO Classification (Surface Epithelial Origin - most common ~70%)
4. Serous Cystadenoma / Cystadenocarcinoma
- Most common epithelial ovarian tumor; constitutes ~25% of all ovarian tumors
- Gross: Unilocular or multilocular cyst; thin-walled; filled with watery (serous) fluid; may have papillary excrescences
- Micro (benign): Lined by a single layer of low cuboidal to columnar tubal-type (ciliated) epithelium; psammoma bodies may be present
- Borderline: Increased architectural complexity, nuclear stratification (2-3 layers), no stromal invasion
- Malignant (High-grade serous carcinoma): Solid and cystic; papillary architecture; high nuclear grade; TP53 mutations in nearly all; BRCA1/BRCA2 germline mutations in ~10-15%; thought to arise from fallopian tube epithelium (serous tubal intraepithelial carcinoma - STIC)
- Bilateral in ~30% of serous cystadenomas; higher bilaterality in carcinomas
5. Mucinous Cystadenoma / Cystadenocarcinoma
- Second most common epithelial tumor
- Gross: Often large (can reach 50+ cm), multilocular ("honeycomb" appearance); filled with viscous, mucoid material; smooth inner surface
- Micro (benign): Lined by tall columnar mucin-secreting cells resembling endocervical or intestinal epithelium; goblet cells may be present
- Borderline: Epithelial stratification up to 3 layers, tufting, mild atypia; no stromal invasion
- Malignant: Glandular structures invading stroma; often intestinal type; KRAS mutations common
- Typically unilateral
- A rare but serious complication: rupture can seed the peritoneum with mucin-secreting cells causing pseudomyxoma peritonei
6. Endometrioma ("Chocolate Cyst")
- Ovarian cyst arising from endometriosis within the ovary
- Gross: Unilocular cyst containing thick, dark-brown ("chocolate") fluid - old hemorrhagic debris from cyclical bleeding; can grow 6-8 cm
- Micro: Wall lined by endometrial-type glandular epithelium and stroma, with hemosiderin-laden macrophages; epithelium may be attenuated or absent in older lesions
- Clinical: Pelvic pain (often cyclical/menstrual), dyspareunia; rupture causes acute generalized peritoneal irritation; associated with infertility
- Dense adhesions are characteristic
- Diagnosis by histology (since chocolate fluid may also be found in hemorrhagic corpus luteum cysts)
III. Germ Cell Tumors with Cystic Morphology
7. Mature Cystic Teratoma (Dermoid Cyst)
- Most common germ cell tumor of the ovary; accounts for ~15-25% of all ovarian tumors in young women
- Age: Young adult females (reproductive age)
- Bilateral in 10-15%
- Karyotype: 46,XX; arises from an ovum after the first meiotic division
Gross Appearance:
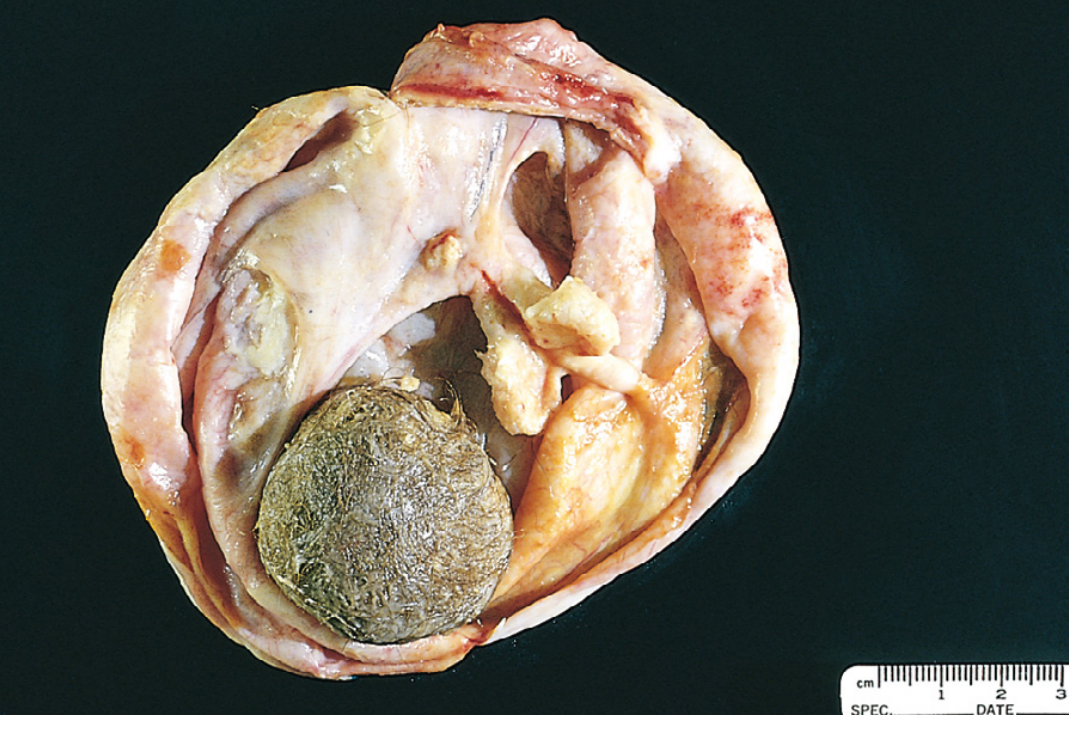
- Unilocular cyst filled with sebaceous material and hair
- Wall is opaque, gray-white, wrinkled epidermis with protruding hair shafts
- Contains teeth and areas of calcification (visible on plain X-ray)
- A Rokitansky protuberance (dermoid plug) - a nodule of tissue at one pole of the cyst - is characteristic
Micro:
- Wall lined by stratified squamous epithelium with sebaceous glands, hair shafts, and skin adnexa
- Tissues from all three germ layers can be found: cartilage, bone, thyroid (struma ovarii), neural tissue, respiratory epithelium
- ~1% undergo malignant transformation, most commonly to squamous cell carcinoma
Clinical:
- Usually asymptomatic; discovered incidentally
- May rupture causing chemical peritonitis (sebaceous material is highly irritating)
- Torsion is a common complication
- Struma ovarii - if thyroid tissue predominates, may cause hyperthyroidism
- Rarely associated with anti-NMDA receptor encephalitis (paraneoplastic)
8. Immature (Malignant) Teratoma
- Rare; mean age 18 years (prepubertal/adolescent)
- Contains immature embryonal/fetal tissue - chiefly immature neuroepithelium
- Gross: Bulky, smooth external surface, predominantly solid with areas of necrosis and hemorrhage
- Micro: Graded I-III based on proportion of immature neuroepithelium - grade determines prognosis
- More aggressive than mature teratoma; risk of spread correlates with histologic grade
IV. Other Cystic Ovarian Lesions
9. Brenner Tumor (Transitional Cell Tumor)
- Usually benign (~10% of ovarian epithelial tumors); typically unilateral (90%)
- Gross: Solid or cystic; variable size (< 1 cm to 20-30 cm); fibrous, white-gray cut surface
- Micro: Nests of urothelium-like (transitional) epithelial cells within a dense fibrous stroma; mucinous glands often present in centers of nests
- Often detected incidentally; even when large, usually behaves benignly
10. Polycystic Ovary (PCOS)
- Bilateral, enlarged ovaries with multiple small follicular cysts (< 1 cm each; ≥12 per ovary) in the cortex with a thickened, white fibrous cortex
- Not a true cyst - represents a syndrome of anovulation (LH:FSH imbalance, insulin resistance, hyperandrogenism)
- Rotterdam criteria: >10 mL ovarian volume or ≥12 subcentimeter antral follicles per ovary
Summary Table
| Cyst Type | Origin | Fluid | Bilaterality | Key Feature |
|---|---|---|---|---|
| Follicular | Graafian follicle | Clear, serous | Unilateral | Thin wall; resolves in 4-8 weeks |
| Corpus Luteum | Ruptured follicle | Hemorrhagic | Unilateral | Right-sided rupture; hemoperitoneum |
| Theca-Lutein | hCG excess | Straw-colored | Bilateral | Molar pregnancy association |
| Serous Cystadenoma | Surface epithelium | Watery/serous | ~30% bilateral | Psammoma bodies; BRCA association |
| Mucinous Cystadenoma | Surface epithelium | Viscous, mucoid | Mostly unilateral | Largest ovarian tumors; pseudomyxoma peritonei |
| Endometrioma | Ectopic endometrium | Thick, dark brown | Can be bilateral | "Chocolate cyst"; cyclical pain |
| Dermoid Cyst | Germ cells (all layers) | Sebaceous + hair | 10-15% bilateral | Teeth; Rokitansky protuberance; 1% malignant change |
| Brenner Tumor | Surface epithelium | Solid/cystic | 90% unilateral | Urothelial nests in fibrous stroma |
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease - Classification, Morphology of Teratomas, Epithelial Tumors, Brenner Tumors
- Berek & Novak's Gynecology - Functional Cysts, Theca-Lutein Cysts, Endometriomas, PCOS
- Rosen's Emergency Medicine - Follicular and Corpus Luteum Cysts, Clinical Features
- Schwartz's Principles of Surgery - Benign Ovarian Lesions
This is a shared conversation. Sign in to Orris to start your own chat.