
Diagnosis and treatment
Checking Date & Time
Reading File
Finding Sources
Searching PubMed
pleural effusion diagnosis treatment
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Searching Images
massive left pleural effusion chest X-ray with mediastinal shift
I now have comprehensive information from the medical library to provide a thorough analysis. Here is the complete radiological interpretation and management plan.
Chest X-Ray Analysis
Patient: Swathi, 44-year-old female | Date: 22/04/2026
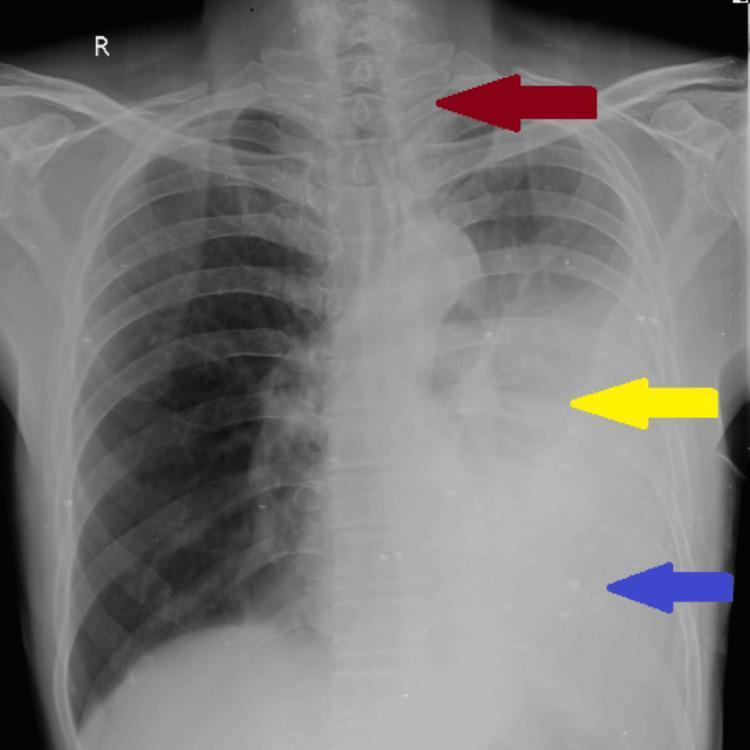
Radiological Findings
| Feature | Finding |
|---|---|
| Left hemithorax | Complete homogeneous white-out — total opacification |
| Left costophrenic angle | Obliterated |
| Left hemidiaphragm | Not visible |
| Left cardiac border | Silhouette sign — obscured |
| Mediastinum | Shifted to the RIGHT (trachea and cardiac silhouette displaced contralaterally) |
| Right lung | Relatively clear; compensatory expansion |
The mediastinum shifting away from the opaque side is the key discriminating sign: in massive pleural effusion, the large fluid volume pushes the mediastinum contralaterally. If it were shifted toward the white-out, collapse/atelectasis would be favored instead.
Diagnosis
Massive Left-Sided Pleural Effusion
The entire left hemithorax is opacified with rightward mediastinal shift — the classic CXR appearance of a massive pleural effusion (>1 liter, often >2–3 liters). As described in Roberts & Hedges' Clinical Procedures in Emergency Medicine: "In the case of a massive pleural effusion, the entire hemithorax is opacified. In the absence of a diseased lung or mediastinum, large fluid collections push the mediastinum contralaterally."
A reference image from the medical literature showing the identical pattern:
Differential Diagnosis of the Underlying Cause
The effusion must be characterized as transudative vs. exudative (Light's criteria). Given that this is a 44-year-old woman with a massive unilateral effusion, the most likely causes are:
Exudative (more likely given unilateral massive effusion)
| Cause | Notes |
|---|---|
| Malignancy (lung, breast, lymphoma, mesothelioma) | #1 cause of massive unilateral effusion in adults |
| Tuberculosis | Very common in India; exudate, high lymphocytes, high ADA |
| Parapneumonic / Empyema | Fever, purulent fluid; pH <7.2 |
| Chylothorax | Milky fluid; high triglycerides |
Transudative (less likely for massive unilateral)
| Cause | Notes |
|---|---|
| Congestive heart failure | Usually bilateral |
| Nephrotic syndrome / cirrhosis | Usually bilateral, associated signs |
| Meigs syndrome | Ovarian fibroma + effusion + ascites |
Diagnostic Workup
Immediate
-
Thoracentesis (diagnostic + therapeutic) — first priority
- Send pleural fluid for: protein, LDH, glucose, pH, cell count & differential, Gram stain & culture, AFB smear & culture, cytology, ADA (adenosine deaminase — critical for TB in this demographic)
- Apply Light's Criteria to classify transudate vs. exudate:
- PF protein / serum protein > 0.5 → exudate
- PF LDH / serum LDH > 0.6 → exudate
- PF LDH > 2/3 upper limit normal serum LDH → exudate
-
Ultrasound of chest — before thoracentesis to identify safe puncture site, detect loculations
-
CT chest with contrast — defines underlying lung parenchyma, masses, lymphadenopathy, pleural nodularity
-
Bloods — CBC, CRP, LFTs, renal function, serum protein/albumin, LDH
-
Sputum AFB × 3, CBNAAT if TB suspected
-
Pleural biopsy (Abrams needle or VATS) if cytology negative and diagnosis unclear
Treatment
Acute Management
- Therapeutic thoracentesis — remove up to 1.5 L at a time to relieve dyspnea; re-expansion pulmonary edema can occur if >1.5 L removed rapidly
- Supplemental oxygen — for hypoxia from mediastinal shift and compressive atelectasis
- Upright positioning — improves respiratory mechanics
Definitive Treatment (based on cause)
| Etiology | Treatment |
|---|---|
| TB | Anti-tubercular therapy (HRZE 2 months → HR 4 months); consider corticosteroids to reduce fibrous sequelae |
| Malignant | Intercostal drain + pleurodesis (talc/doxycycline) or indwelling pleural catheter (IPC) for recurrent effusion; systemic oncological treatment |
| Parapneumonic | IV antibiotics + chest tube drainage; fibrinolytics (tPA/DNase) for loculated empyema; VATS decortication if organized |
| Heart failure / transudative | Treat underlying cause (diuretics, dialysis); avoid chest tube in hepatic hydrothorax |
| Chylothorax | Low-fat diet / TPN; octreotide; surgical ligation of thoracic duct |
Indications for Chest Tube / Surgical Intervention
- Empyema (pus on aspiration, pH <7.2, glucose <60, LDH >1000)
- Loculated effusion not draining with needle thoracentesis
- Recurrent symptomatic effusion (consider IPC or pleurodesis)
- Trapped lung requiring decortication
Key Points for This Patient
Given the patient demographics (44F, India, 2026), tuberculosis and malignancy (especially lung/breast primary) are the top differentials for a massive unilateral pleural effusion. ADA >35–40 U/L in pleural fluid strongly suggests TB. A CT chest and pleural fluid cytology/biopsy are essential if thoracentesis alone is inconclusive.
Sources:
- Sabiston Textbook of Surgery, 20e — Pleural Effusions, Light's Criteria, Benign and Malignant PE management
- Roberts & Hedges' Clinical Procedures in Emergency Medicine — Massive pleural effusion CXR interpretation, thoracentesis technique
- Fishman's Pulmonary Diseases and Disorders — Malignant pleural effusion management, IPC, pleurodesis
- British Thoracic Society Guideline for pleural disease, 2023 (Thorax) — PMID 37553157
- ERS Statement on Benign Pleural Effusions, 2024 (Eur Respir J) — PMID 39060018
⚠️ Disclaimer: This analysis is for educational/clinical decision support purposes. All management decisions must be made by a qualified clinician with full clinical context, examination findings, and patient history.
This is a shared conversation. Sign in to Orris to start your own chat.