Hyponatremia correction
Reading File
Finding Sources
Searching PubMed
"hyponatremia"[MeSH Terms] AND "treatment"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive data from multiple authoritative sources. Here is a complete, structured answer.
Hyponatremia Correction
Definition: Serum sodium < 135 mEq/L (severe: < 120-125 mEq/L).
Step 1 - Classify Before Treating
Before correcting, determine:
- Acuity - Acute (< 48 h) vs. chronic (> 48 h, or unknown duration which is treated as chronic)
- Severity of symptoms - Mild (headache, nausea) vs. severe (seizures, obtundation, coma)
- Volume status - Hypovolemic / Euvolemic / Hypervolemic
Common Causes by Volume Status
| Volume Status | Causes |
|---|---|
| Hypovolemic | Diarrhea/vomiting, thiazide diuretics, adrenal insufficiency, cerebral salt wasting |
| Euvolemic | SIADH, hypothyroidism, psychogenic polydipsia, beer potomania, MDMA |
| Hypervolemic | Heart failure, cirrhosis, chronic kidney disease |
| Pseudo-hyponatremia | Hyperlipidemia, hyperproteinemia, hyperglycemia |
Step 2 - Determine the Correction Strategy
A. Acute Symptomatic Hyponatremia (< 48 h, or seizures/coma regardless of chronicity)
Goal: Raise sodium by 4-6 mmol/L promptly to stop herniation - do not aim for full correction acutely.
Treatment:
- Severe symptoms (seizures, coma): 100 mL of 3% NaCl IV over 10 minutes, repeated up to 2 more times (total up to 300 mL)
- Mild to moderate symptoms: 3% NaCl infusion at 0.5-2 mL/kg/hour
- Rate of correction is not restricted in true acute hyponatremia
- Add supplemental O2 and ventilatory support if pulmonary edema develops; IV loop diuretics treat pulmonary edema and increase free water excretion
"A bolus of 100 mL of hypertonic saline is more effective than an infusion, rapidly improving both serum sodium and mental status." - Harrison's Principles of Internal Medicine 22E
B. Chronic Hyponatremia (> 48 h, or unknown duration)
This is where the risk of osmotic demyelination syndrome (ODS) - formerly called central pontine myelinolysis - is greatest.
Correction Rate Limits
| Risk of ODS | 24-hour limit | Goal per 24 h |
|---|---|---|
| Normal risk | ≤ 10-12 mmol/L (≤ 18 mmol/L per 48 h) | 4-8 mmol/L |
| High risk | ≤ 8 mmol/L | 4-6 mmol/L |
High-risk patients for ODS:
- Serum Na < 105 mmol/L
- Hypokalemia
- Alcohol use disorder / malnutrition
- Advanced liver disease (cirrhosis)
- Beer potomania
"The rate of correction should not exceed 8 mmol/L in any 24-hour period in patients at high risk of ODS, and not exceed 10-12 mmol/L in any 24-hour period for patients at normal risk." - Goldman-Cecil Medicine
Schwartz's Surgery uses a slightly more conservative number: no more than 0.5 mEq/L/hour for asymptomatic correction, maximum 12 mEq/L/day; symptomatic cases may target 1 mEq/L/hour until Na reaches 130 mEq/L.
Step 3 - Treatment by Cause
Hypovolemic Hyponatremia
- IV isotonic (normal) saline to restore volume
- ADH will normalize once volume is restored, which can sometimes cause a rapid spontaneous rise in sodium - monitor closely
Euvolemic Hyponatremia (SIADH)
- Fluid restriction (typically ≥ 500 mL less than urine output per day)
- Use the urine-to-plasma electrolyte ratio ([uNa + uK] / pNa) to guide restriction aggressiveness:
- Ratio > 1 → aggressive restriction < 500 mL/day
- Ratio ~1 → restrict to 500-700 mL/day
- Ratio < 1 → restrict to < 1 L/day
- Oral solute loading: salt tablets + furosemide (20 mg BID) to increase free water excretion
- Oral urea is also effective and well-tolerated
- Vaptans (V2-receptor antagonists): tolvaptan 15-60 mg/day orally; conivaptan IV - indicated for persistent SIADH unresponsive to fluid restriction; NOT for hypovolemic or acute hyponatremia; tolvaptan is restricted to < 1-2 months due to hepatotoxicity risk, and is contraindicated in cirrhosis
- Demeclocycline - inhibits ADH at collecting duct; rarely used now due to nephrotoxicity
Hypervolemic Hyponatremia (heart failure, cirrhosis, CKD)
- Sodium + water restriction
- Loop diuretics
- Treat underlying condition (e.g., optimize ACE inhibition in heart failure)
- Tolvaptan may be used in heart failure but NOT in cirrhosis
Step 4 - Sodium Deficit Formula
The traditional formula for calculating how much Na+ to give:
Na deficit = 0.6 × body weight (kg) × (target [Na+] - current [Na+])
(use 0.5 for women; 0.6 for men)
This estimates the amount of Na+ needed, but plasma Na+ changes unpredictably in practice - check sodium every 2-4 hours during active correction with hypertonic saline.
Step 5 - Managing Overcorrection
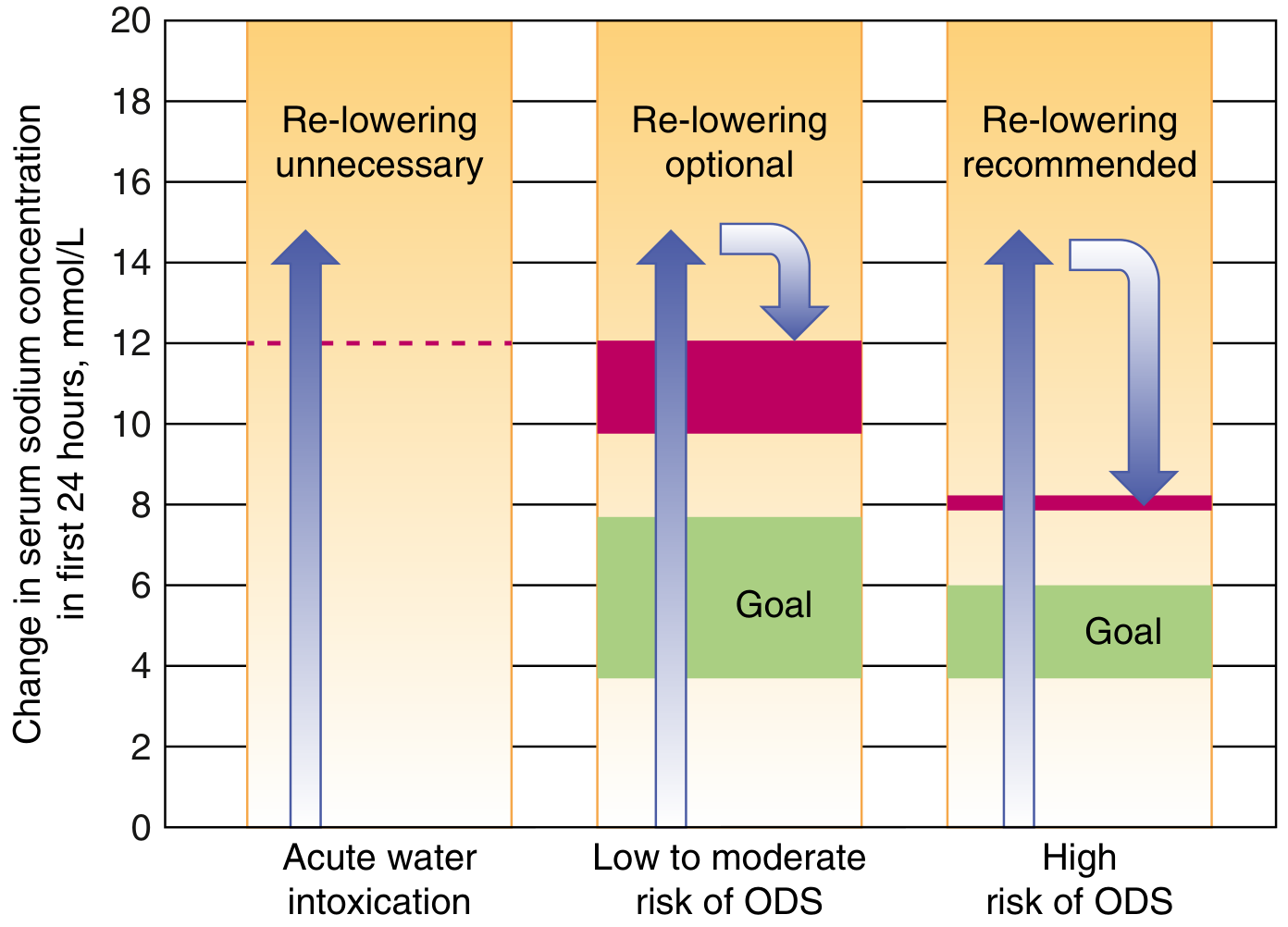
If the sodium rises too fast (exceeds limits above):
- If starting Na was ≥ 120 mmol/L → re-lowering is often unnecessary
- If starting Na was < 120 mmol/L → re-lower to target:
- DDAVP 2-4 mcg IV/SC every 8 hours (clamps further water excretion)
- D5W IV at ~3 mL/kg/hour to replace free water
- Withhold next vaptan dose if correction > 8 mmol/L
- Consider dexamethasone 4 mg IV every 6 hours for 24-48 h if overcorrection has occurred
- Check Na hourly until target is reached
ODS (Osmotic Demyelination Syndrome) - Key Points
- Occurs days after rapid correction of chronic hyponatremia
- Affects the pons most often (central pontine myelinolysis); can also affect extrapontine sites
- Clinical features: fluctuating consciousness, pseudobulbar palsy, quadriparesis, ataxia, dysarthria, dysphagia
- Diagnosis: MRI of brainstem
- Prevention is the only reliable strategy - there is no established treatment once it develops
Practical Summary
| Scenario | Target | Treatment |
|---|---|---|
| Acute severe (seizures) | +4-6 mmol/L urgently | 3% NaCl 100 mL bolus x1-3 |
| Chronic symptomatic | +4-8 mmol/L/24 h | 3% NaCl infusion + monitoring |
| Chronic asymptomatic | ≤ 12 mmol/L/24 h, ideally 4-8 | Fluid restriction ± medications |
| Hypovolemic | Correct volume | 0.9% NaCl |
| SIADH | Slow, controlled | Fluid restrict → vaptans if refractory |
| Overcorrection | Re-lower to goal | DDAVP + D5W |
Sources: Goldman-Cecil Medicine (International Ed.), Harrison's Principles 22E, Schwartz's Principles of Surgery 11E, Brenner & Rector's The Kidney, Tintinalli's Emergency Medicine, Rosen's Emergency Medicine, Fischer's Mastery of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.