Diagnostic criteria for refractory ascites
refractory ascites diagnostic criteria International Ascites Club 2024
"refractory ascites" AND "diagnostic criteria"
"refractory ascites" AND cirrhosis AND management
Diagnostic Criteria for Refractory Ascites
Two Subtypes (IAC Classification)
A. Diuretic-Resistant Ascites
B. Diuretic-Intractable Ascites
Prior Treatment Requirements (must be met before labeling "refractory")
| Parameter | Requirement |
|---|---|
| Diuretic regimen | Spironolactone 400 mg/day + furosemide 160 mg/day (or amiloride 30 mg/day if spironolactone not tolerated) |
| Duration | At least 1 week of intensive diuretic therapy |
| Diet | Salt-restricted diet of <80 mEq/day (<2 g sodium/day) |
Operational Definitions
| Term | Definition |
|---|---|
| Lack of response | Mean weight loss <0.8 kg over 4 days AND urinary sodium output less than sodium intake |
| Early ascites recurrence | Reappearance of grade 2 or 3 ascites within 4 weeks of initial mobilization |
| Diuretic-induced hepatic encephalopathy | Development of encephalopathy in the absence of any other precipitating factor |
| Diuretic-induced renal impairment | Serum creatinine increase by >100% to a value >2 mg/dL in a patient whose ascites is otherwise responding to treatment |
| Diuretic-induced hyponatremia | Serum sodium <125 mEq/L |
| Diuretic-induced hypo/hyperkalemia | Potassium <3 mEq/L (hypokalemia) or >6 mEq/L (hyperkalemia) despite appropriate supplementation |
Key Points
- Compliance with sodium restriction must be confirmed before applying the label "refractory." Non-compliance is a common reason for apparent diuretic resistance. Spot urinary Na:K ratio or 24-hour urine sodium can help assess adherence.
- Patients who maintain urinary sodium excretion >30 mEq/day on diuretics may continue diuretics (even with refractory ascites) to prolong intervals between large-volume paracenteses (LVPs).
- Once refractory ascites is confirmed, diuretics should generally be stopped in non-responders to avoid adverse events.
- The classification was established by the International Ascites Club (Salerno et al.) and has been adopted by EASL and AASLD guidelines.
Management After Diagnosis
- LVP + IV albumin (8 g per liter removed) - first-line
- TIPS (covered stent preferred) - improves ascites control; survival benefit shown in recurrent ascites but not clearly in refractory ascites alone
- Liver transplantation - definitive therapy; all eligible patients should be referred
How to differentiate between compensated and decompensated cirrhosis
compensated vs decompensated cirrhosis differentiation criteria clinical features 2024
Compensated vs. Decompensated Cirrhosis
Core Distinction
"The development of complications of variceal haemorrhage, ascites, encephalopathy, jaundice, or HCC characterizes decompensated cirrhosis. In compensated cirrhosis, these complications are absent."
- Sleisenger & Fordtran's GI and Liver Disease
The Four-Stage Clinical Model
| Stage | Description | 1-Year Mortality |
|---|---|---|
| Stage 1 (Compensated) | No varices, no ascites | ~1% |
| Stage 2 (Compensated) | Varices present, no bleeding, no ascites | ~3-4% |
| Stage 3 (Decompensated) | Ascites ± varices (no bleeding) | ~20% |
| Stage 4 (Decompensated) | Variceal bleeding ± ascites | ~57% |
- Stages 1-2 = Compensated cirrhosis
- Stages 3-4 = Decompensated cirrhosis
- Yamada's Textbook of Gastroenterology, 7th ed.
Clinical Features
| Feature | Compensated | Decompensated |
|---|---|---|
| Symptoms | Often none; mild fatigue, anorexia | Overt, often disabling |
| Ascites | Absent | Present (grade 2-3) |
| Variceal bleeding | No bleeding (varices may be present) | Active or prior bleed |
| Hepatic encephalopathy | Absent | Present (any grade) |
| Jaundice | Absent or minimal | Present |
| Spontaneous bacterial peritonitis | No | Possible |
| Hepatorenal syndrome | No | Possible |
| HCC | Marks transition to decompensated stage | High-risk |
| Signs on exam | Firm liver, possible splenomegaly, spider angiomata | Jaundice, ascites, asterixis, caput medusae, muscle wasting |
Key Labs and Scores
| Parameter | Compensated | Decompensated |
|---|---|---|
| Serum albumin | Near normal (>35 g/L) | Low (<28 g/L severe) |
| Bilirubin | <2 mg/dL | Elevated (>3 mg/dL severe) |
| INR/PT | Near normal (<1.7) | Elevated (>2.3 severe) |
| Creatinine | Usually normal | May be elevated (HRS) |
| Serum Na | Normal | May be hyponatremic |
| Child-Pugh class | Class A (5-6 pts) | Class B (7-9 pts) or Class C (10-15 pts) |
| MELD score | Typically <10 | Higher; used for transplant priority in decompensated patients |
| Platelets | Mildly low (splenomegaly) | Often <100,000/mm³ |
Role of HVPG (Portal Pressure)
| HVPG | Interpretation | Clinical significance |
|---|---|---|
| >5 mmHg | Portal hypertension (defined) | - |
| ≥10 mmHg | Clinically Significant Portal Hypertension (CSPH) | Predicts decompensation, varices, HCC |
| ≥12 mmHg | Threshold for variceal bleeding | Increased bleeding risk |
- Among patients with compensated cirrhosis followed >4 years, only 10% with HVPG <10 mmHg experienced decompensation, versus significantly more when HVPG ≥10 mmHg.
- HVPG and MELD are independent predictors of decompensation in compensated cirrhosis.
- Noninvasive surrogate: liver stiffness (transient elastography) >20 kPa = CSPH.
- Miller's Anesthesia, 10th ed.; Yamada's Textbook of Gastroenterology, 7th ed.
Prognosis
| Compensated | Decompensated | |
|---|---|---|
| Mortality vs. general population | 5× increased | 10× increased |
| Median survival | 9-12 years | ~2 years |
| 5-year survival | 80-85% | 30-50% |
| Main cause of death | Cardiovascular disease, stroke, malignancy | Portal hypertension complications, sepsis, multi-organ failure |
Practical Tips for Differentiation
- Single decompensating event is enough - one episode of ascites, bleeding, or encephalopathy shifts the patient from compensated to decompensated.
- Re-compensation is possible - with treatment of the underlying cause (e.g., viral hepatitis cure, alcohol abstinence), patients can revert to a compensated state, improving prognosis.
- Infection is now recognized as a distinct stage in the natural history, associated with poor survival even after infection clearance.
- ACLF (Acute-on-Chronic Liver Failure) represents an acute deterioration in decompensated patients with multi-organ failure and very high short-term mortality.
SAAG gradient
SAAG serum ascites albumin gradient interpretation causes 2024
Serum-Ascites Albumin Gradient (SAAG)
Formula
- Both samples must be drawn on the same day (ideally simultaneously)
- It is a subtraction, not a ratio
- It does not change with diuresis - safe to calculate even in a patient on diuretics
- Accuracy: ~97% in identifying portal hypertension as the cause of ascites
Physiological Basis
Interpretation: The Cut-off
| SAAG | Interpretation | Accuracy |
|---|---|---|
| ≥1.1 g/dL | Portal hypertension is present | ~97% |
| <1.1 g/dL | Portal hypertension is NOT the cause | ~97% |
Step 1 - Categorize by SAAG
High SAAG (≥1.1 g/dL) - Portal Hypertensive Causes
| Condition | Mechanism |
|---|---|
| Cirrhosis | Sinusoidal fibrosis + portal hypertension |
| Cardiac ascites / Right heart failure | Post-hepatic sinusoidal congestion |
| Budd-Chiari syndrome | Hepatic vein obstruction |
| Sinusoidal obstruction syndrome (veno-occlusive disease) | Hepatic sinusoidal injury |
| Portal vein thrombosis | Pre-hepatic portal hypertension |
| Massive liver metastases | Sinusoidal compression |
| Fulminant hepatic failure | Acute sinusoidal hypertension |
| Fatty liver of pregnancy |
Low SAAG (<1.1 g/dL) - Non-Portal Hypertensive (Peritoneal) Causes
| Condition |
|---|
| Peritoneal carcinomatosis |
| Tuberculous peritonitis |
| Pancreatic ascites |
| Biliary ascites |
| Nephrotic syndrome |
| Serositis (connective tissue diseases, SLE) |
| Bowel obstruction or infarction |
| Postoperative lymphatic leak |
| Chylous ascites |
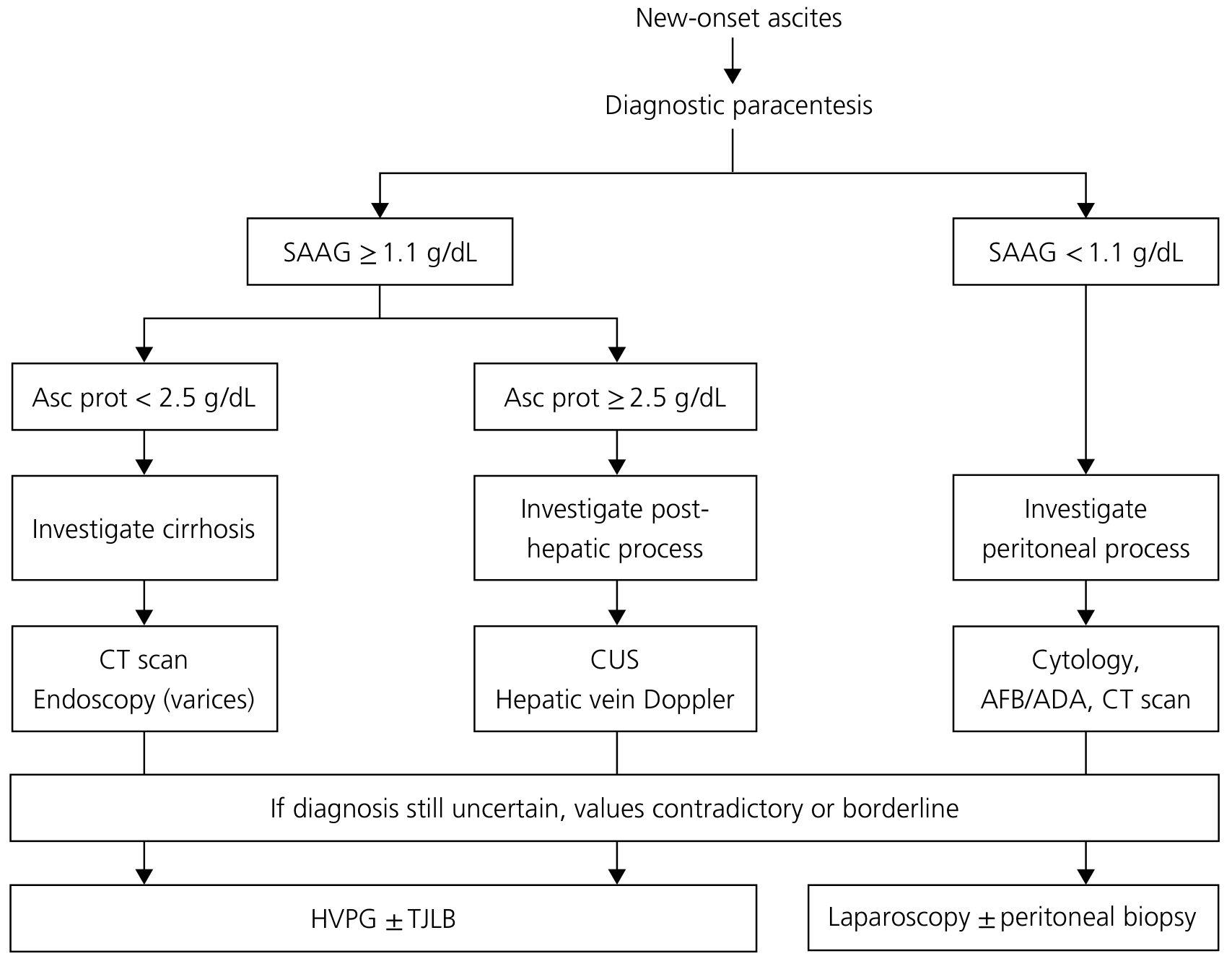
Step 2 - For High SAAG: Sub-classify by Ascitic Fluid Total Protein
| SAAG ≥1.1 g/dL | Ascitic protein | Interpretation | Next investigation |
|---|---|---|---|
| High | <2.5 g/dL | Intrahepatic cause - cirrhosis, late Budd-Chiari, massive metastases. Sinusoids are scarred ("capillarization") and do not allow protein passage | CT scan + endoscopy for varices |
| High | ≥2.5 g/dL | Post-hepatic cause - cardiac ascites, early Budd-Chiari, sinusoidal obstruction syndrome. Normal sinusoids are "leaky" and allow protein outpouring | Cardiac echo (BNP), hepatic vein Doppler |
In cirrhosis, fibrosis deposits in sinusoids ("capillarization of the sinusoid") make them less permeable to macromolecules, resulting in low protein in the ascitic fluid - even though portal pressure is high.
Diagnostic Flowchart (Yamada's, Fig. 98.1)
Practical Pearls & Pitfalls
| Situation | Effect on SAAG | How to handle |
|---|---|---|
| Chylous ascites | Falsely high SAAG (lipids interfere with albumin assay) | Check triglycerides in ascitic fluid (>200 mg/dL = chylous) |
| Very low serum albumin (≤1.1 g/dL) | SAAG unreliable - cannot be ≥1.1 | Interpret with caution |
| Serum hyperglobulinemia (>5 g/dL) | Falsely low SAAG - globulins narrow the gradient | Corrected SAAG = uncorrected SAAG × (0.16 × [serum globulin (g/dL) + 2.5]) |
| Samples not drawn same day | Inaccurate | Always collect simultaneously |
| Post-albumin infusion | May transiently raise serum albumin | Draw before infusion if possible |
| Diuretics | No effect on SAAG | Safe to calculate at any time |
| "Mixed" ascites (e.g., cirrhosis + peritoneal TB) | May give intermediate or misleading SAAG | Consider both etiologies |
Additional Ascitic Fluid Tests by Indication
| Clinical suspicion | Test to order |
|---|---|
| SBP | Cell count + differential (PMN ≥250 = SBP), culture in blood culture bottles |
| Secondary peritonitis | Glucose (<50 mg/dL), LDH (>serum level), Gram stain (polymicrobial) |
| Pancreatic ascites | Amylase (typically >1000 IU/L) |
| Malignancy | Cytology (≥50 mL fluid, immediate processing) |
| Tuberculous peritonitis | AFB smear/culture, ADA level, lymphocyte predominance |
| Biliary ascites | Bilirubin (ascitic > serum bilirubin) |
| Chylous ascites | Triglycerides (>200 mg/dL) |
| Heart failure | Serum BNP/pro-BNP |
Summary Rule
SAAG ≥1.1 → Portal hypertension
+ Ascitic protein <2.5 → Cirrhosis (intrahepatic)
+ Ascitic protein ≥2.5 → Cardiac / post-hepatic cause
SAAG <1.1 → Peritoneal process
(TB, malignancy, pancreatitis, nephrotic, etc.)
Which is best site for ascitic paracentesis
best site paracentesis ascites technique preferred insertion site guidelines
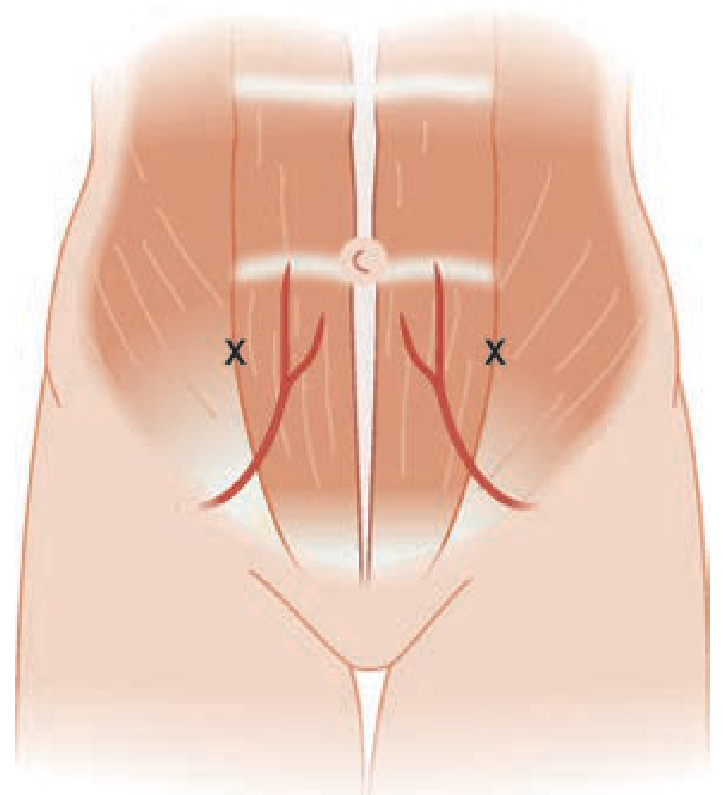
Best Site for Ascitic Paracentesis
Preferred Site: Left Lower Quadrant (LLQ)
3-5 cm superomedial (cranial and medial) to the anterior superior iliac spine (ASIS), lateral to the rectus sheath.
Why LLQ is Preferred Over Other Sites
| Reason | Explanation |
|---|---|
| Thinner abdominal wall | Less subcutaneous fat in LLQ vs. midline, easier access |
| Deeper fluid pocket | More ascitic fluid pools laterally than at midline |
| Avoids inferior epigastric artery | Vessels run along the rectus sheath; LLQ entry is lateral to this |
| Avoids the cecum | Right lower quadrant risks injuring a dilated cecum or appendectomy scar |
| Sigmoid displaces bowel | Sigmoid colon pushes small bowel loops away, creating a safer fluid pocket |
| Avoids liver and spleen | LLQ is away from both organs |
Alternative Sites
| Site | Landmark | When used |
|---|---|---|
| Right lower quadrant (RLQ) | 3-5 cm superomedial to right ASIS, lateral to rectus | If LLQ has scarring, ostomy, or distorted anatomy |
| Midline (infraumbilical) | 2-3 cm below the umbilicus in the midline | Avascular linea alba; used when no US available, especially with tense ascites. Patient in semiupright position |
Anatomical Structures to Avoid
- Inferior epigastric artery - runs within the rectus sheath bilaterally; stay lateral to the rectus muscle
- Surgical scars - adhesions underneath can tether bowel to the abdominal wall
- Abdominal wall collateral veins (caput medusae) - dilated in portal hypertension; visible and palpable
- Liver (right upper quadrant) and spleen (left upper quadrant)
- Urinary bladder - always empty the bladder (void or Foley catheter) before procedure
- Distended cecum (RLQ)
Positioning
- Supine with head of bed at 30-45° - standard
- Left lateral decubitus tilt - if using LLQ; allows fluid to pool toward the left flank
- A pillow under the flank on the opposite side helps shift fluid toward the puncture site
- For small fluid collections: lateral decubitus position with needle in the dependent (down) side
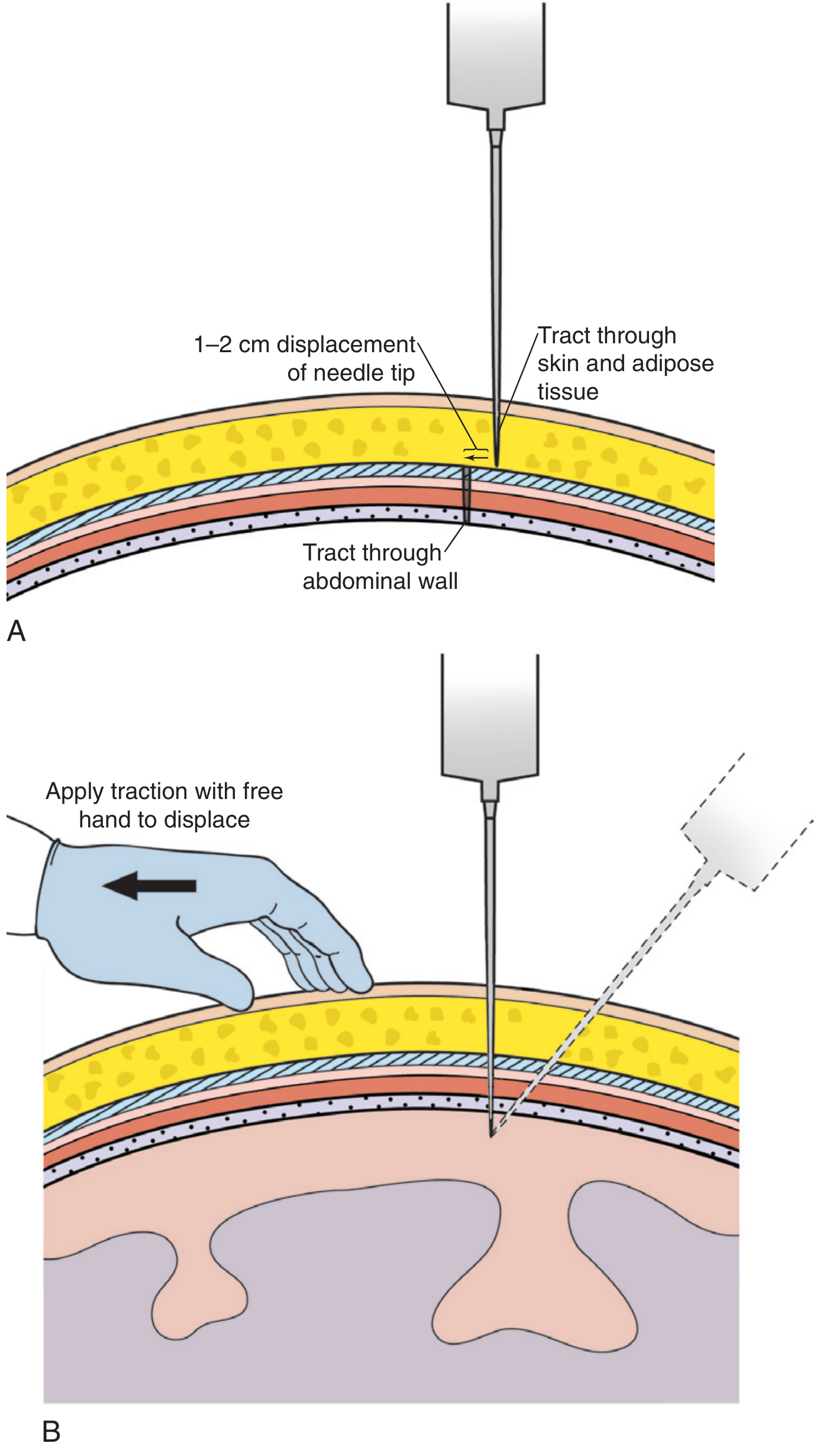
Needle Insertion Technique
Role of Ultrasound Guidance
| Parameter | Without US | With US |
|---|---|---|
| Success rate | ~65% | ~95% |
| Bleeding complications | Higher | Significantly reduced |
| Bowel perforation risk | Higher | Significantly reduced |
Contraindications to Chosen Site
| Contraindication | Alternative |
|---|---|
| Surgical scar at LLQ | Choose RLQ or midline; use US to confirm |
| Ostomy (stoma) near LLQ | Use contralateral side or midline |
| Cellulitis/abscess at site | Choose a different site |
| Pregnancy (>1st trimester) | US-guided paracentesis mandatory; use site away from gravid uterus |
| Distended bladder | Empty first; catheterize if needed |
Diagnostic criteria for SBP and management
spontaneous bacterial peritonitis SBP diagnostic criteria management guidelines 2024
Spontaneous Bacterial Peritonitis (SBP): Diagnostic Criteria and Management
Definition
When to Suspect / Indications for Diagnostic Paracentesis
- Symptoms or signs of SBP: fever, abdominal pain/tenderness, ileus
- Unexplained hepatic encephalopathy
- Unexplained renal dysfunction
- Any hospitalized patient with cirrhosis and ascites, regardless of admission reason
- Upper GI bleeding in a cirrhotic patient
- New or worsening ascites
"Because SBP is often asymptomatic and frequently community acquired, diagnostic paracentesis should be performed when any patient with cirrhosis is admitted to the hospital." - Goldman-Cecil Medicine
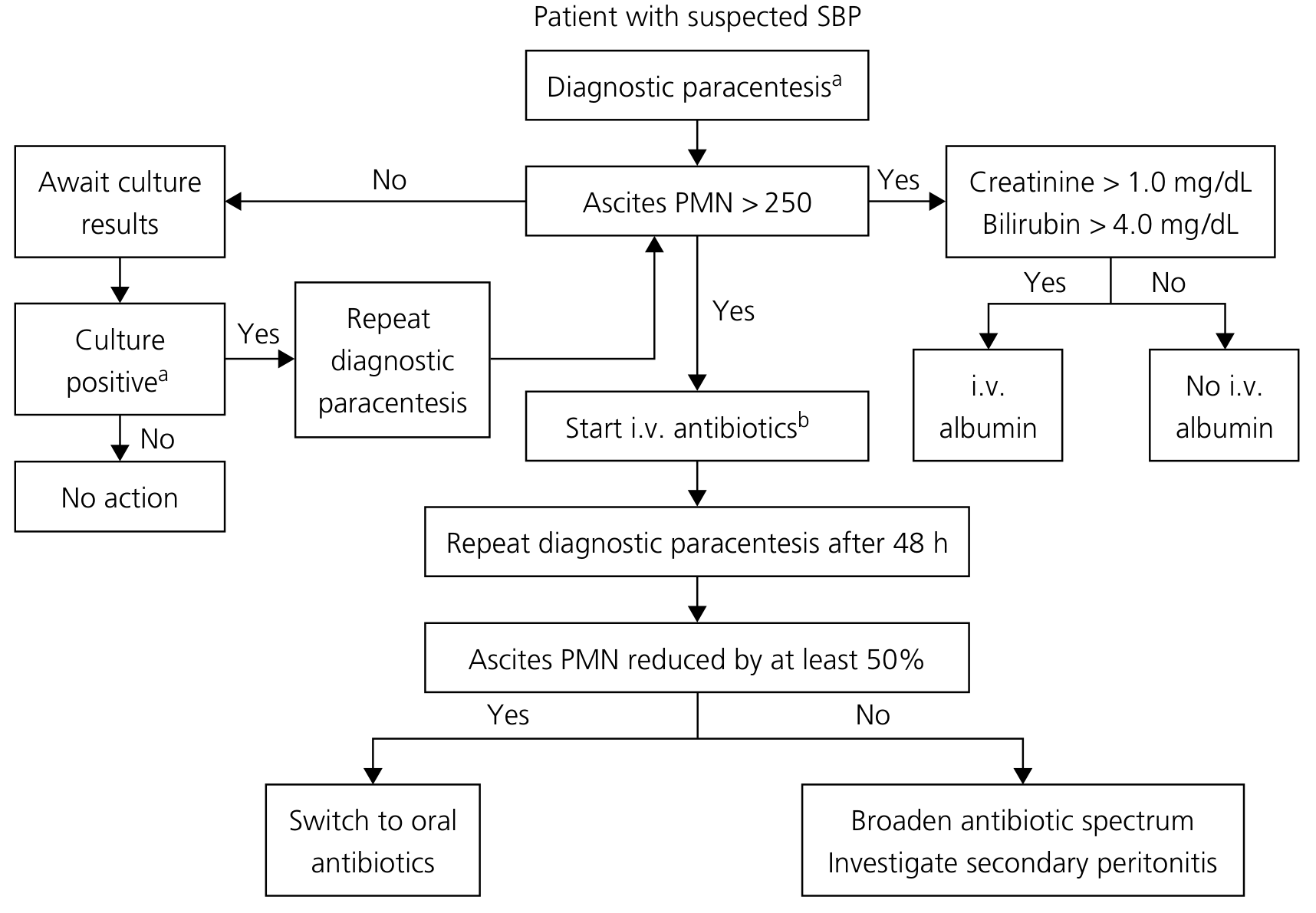
Diagnostic Criteria
Primary Diagnostic Test: Ascitic Fluid PMN Count
| PMN Count | Interpretation | Action |
|---|---|---|
| ≥250 cells/mm³ | SBP diagnosed - Start antibiotics immediately, do NOT wait for culture | Treat + send cultures |
| <250 + culture positive (bacterascites) | Repeat PMN count | See algorithm below |
| <250 + culture negative | No SBP - no treatment | Monitor |
Cultures are positive in only 40-60% of cases even with blood culture bottle inoculation. The diagnosis rests on the PMN count, not culture positivity.
SBP Variants
| Variant | PMN Count | Culture | Action |
|---|---|---|---|
| Classic SBP | ≥250/mm³ | + (single organism) | Treat immediately |
| Culture-negative neutrocytic ascites (CNNA) | ≥250/mm³ | Negative | Treat - same mortality as culture-positive SBP |
| Bacterascites (monomicrobial non-neutrocytic) | <250/mm³ | + (single organism) | Repeat PMN count: if ≥250 → treat; if still <250, await 2nd culture |
| Secondary bacterial peritonitis | ≥250/mm³ | Polymicrobial | Investigate surgically - do NOT treat as SBP alone |
Distinguishing SBP from Secondary Bacterial Peritonitis
| Feature | SBP | Secondary Peritonitis |
|---|---|---|
| Organisms | Monomicrobial (usually gram-negative) | Polymicrobial |
| Ascitic protein | Low (<1 g/dL) | >1 g/dL |
| Ascitic glucose | Normal | <50 mg/dL |
| Ascitic LDH | Normal | >upper limit of serum normal |
| CEA | Normal | >5 ng/mL |
| ALP | Normal | >240 U/L |
| Treatment response | PMN drops ≥25% at 48h | PMN fails to drop |
Management Algorithm
Treatment
1. Antibiotics
| Setting | First-line | Alternative |
|---|---|---|
| Community-acquired | IV Cefotaxime 2g q8-12h × 5-7 days | Ceftriaxone 2g IV q24h |
| Healthcare-associated (hospitalized in last 3 months) | Broader spectrum (Pip-tazo, ertapenem) | Narrow based on cultures |
| Nosocomial (>48h after admission) | Imipenem/meropenem ± vancomycin (for MDR coverage) | Based on local resistance patterns |
- Do NOT use aminoglycosides - nephrotoxic in cirrhosis
- Duration: 5-7 days (can be guided by PMN trend)
- Start empirically before culture results - do not delay
2. IV Albumin (Renal Protection)
| Indication | Dose |
|---|---|
| Creatinine >1.0 mg/dL, OR BUN >30 mg/dL, OR bilirubin >4 mg/dL | Day 1: 1.5 g/kg IV within 6h of diagnosis Day 3: 1 g/kg IV Max: 100 g/dose |
| Creatinine normal AND bilirubin <4 mg/dL | Albumin may NOT be needed |
"Albumin reduces the risk of renal failure and acute mortality" but does not reduce 3-month mortality in cirrhotic patients with infections other than SBP. - Goldman-Cecil Medicine
3. Monitoring Response
- Repeat diagnostic paracentesis at 48 hours
- Adequate response: PMN count decreased by ≥25% from baseline (some sources say ≥50%)
- If PMN fails to decrease: broaden antibiotic coverage, investigate secondary peritonitis with imaging
Prophylaxis
Secondary Prophylaxis (after an SBP episode) - MANDATORY
| Drug | Dose | Duration |
|---|---|---|
| Ciprofloxacin (preferred - norfloxacin withdrawn from US market) | 500 mg PO daily | Until ascites resolves, liver transplant, or death |
| Rifaximin | 400 mg TID or 550 mg BID | Alternative to ciprofloxacin |
| TMP-SMX | 1 DS tab daily | Alternative |
1-year SBP recurrence rate without prophylaxis is ~70%. Prophylaxis reduces this significantly.
Primary Prophylaxis
| Indication | Drug | Duration |
|---|---|---|
| Acute variceal bleeding | Ceftriaxone 1g IV q24h (preferred in-hospital) OR ciprofloxacin 500 mg PO q12h | 7 days |
| Low ascitic protein <1.5 g/dL + renal dysfunction (Cr ≥1.2, BUN ≥25, Na ≤130) OR liver failure (Child-Pugh ≥9, bilirubin ≥3 mg/dL) | Ciprofloxacin 500 mg PO daily | Long-term |
Prognosis
- In-hospital mortality: ~20-30%
- 2-year survival after SBP: ~30%
- All patients who survive SBP should be referred for liver transplant evaluation
Definition of sepsis, SIRS and septic shock
Sepsis-3 definition SIRS septic shock 2024 Surviving Sepsis Campaign criteria
Definitions: SIRS, Sepsis, and Septic Shock
Historical Context: Evolution of Definitions
| Year | Consensus | Key Change |
|---|---|---|
| 1991 | Bone et al. (ACCP/SCCM) | SIRS defined; Sepsis = SIRS + infection |
| 2001 | Sepsis-2 | Expanded list of criteria; SIRS retained |
| 2016 | Sepsis-3 (Singer et al., JAMA) | Abandoned SIRS; defined sepsis by organ dysfunction (SOFA); eliminated "severe sepsis" |
1. SIRS - Systemic Inflammatory Response Syndrome
Definition
Criteria: ≥2 of the following 4
| Parameter | Abnormal Value |
|---|---|
| Temperature | >38°C (100.4°F) OR <36°C (96.8°F) |
| Heart rate | >90 bpm |
| Respiratory rate | >20 breaths/min OR PaCO₂ <32 mmHg |
| WBC count | >12,000/mm³ OR <4,000/mm³ OR >10% bands |
Causes of SIRS (non-infectious)
Why SIRS is no longer sufficient to define sepsis (Sepsis-3 rationale)
- SIRS is present in many hospitalized patients who never develop infection
- SIRS criteria fail to identify the key pathobiology: dysregulated host response causing organ dysfunction
- Both pro- and anti-inflammatory cascades are activated in sepsis - a purely inflammatory criterion misses this
- A SOFA increase of ≥2 has a 10% in-hospital mortality - SIRS alone does not carry this prognostic weight
- The term "severe sepsis" has been eliminated (all sepsis by Sepsis-3 involves organ dysfunction)
"The current use of 2 or more SIRS criteria to identify sepsis was unanimously considered by the task force to be unhelpful." - Sepsis-3 Task Force
2. Sepsis (Sepsis-3, 2016)
Definition
"Life-threatening organ dysfunction caused by a dysregulated host response to infection."
Operationalized as:
SOFA Score (Sequential Organ Failure Assessment)
| Organ System | Parameter | Score 0 | Score 1 | Score 2 | Score 3 | Score 4 |
|---|---|---|---|---|---|---|
| Respiratory | PaO₂/FiO₂ | >400 | 301-400 | <300 | <200 | <100 |
| Coagulation | Platelets (×10³/µL) | >150 | 101-150 | 51-100 | 21-50 | <20 |
| Liver | Bilirubin (mg/dL) | <1.2 | 1.2-1.9 | 2.0-5.9 | 6.0-11.9 | >12 |
| Cardiovascular | MAP or vasopressors | MAP >70 | MAP <70 | Vasopressors (low dose) | Vasopressors (higher dose) | Vasopressors (high dose) |
| CNS | GCS | 15 | 13-14 | 10-12 | 6-9 | <6 |
| Renal | Creatinine (mg/dL) / UO | <1.2 | 1.2-1.9 | 2.0-3.4 | 3.5-4.9 or UO <500 mL/d | >5.0 or UO <200 mL/d |
qSOFA (Quick SOFA) - Bedside Screening Tool
| Criterion | Threshold |
|---|---|
| Altered mental status | GCS <15 |
| Systolic blood pressure | ≤100 mmHg |
| Respiratory rate | ≥22 breaths/min |
3. Septic Shock (Sepsis-3)
Definition
Diagnostic Criteria (ALL three must be met):
| Criterion | Threshold |
|---|---|
| Sepsis present | SOFA ≥2 with infection |
| Vasopressor requirement | To maintain MAP ≥65 mmHg |
| Serum lactate | >2 mmol/L (>18 mg/dL) despite adequate fluid resuscitation |
Lactate >2 mmol/L must persist after volume resuscitation - this excludes simple hypovolemia.
Summary Comparison Table
| Feature | SIRS | Sepsis (Sepsis-3) | Septic Shock |
|---|---|---|---|
| Core concept | Physiologic stress response | Dysregulated host response to infection with organ dysfunction | Profound circulatory + metabolic failure |
| Infection required | No (can be non-infectious) | Yes | Yes |
| Organ dysfunction | Not required | Required (SOFA ≥2) | Required |
| Criteria | ≥2 of 4 (temp, HR, RR, WBC) | Infection + SOFA ↑≥2 | Sepsis + vasopressor + lactate >2 |
| Vasopressor | No | No | Yes (MAP ≥65 target) |
| Lactate | Not included | Not required (but elevated = worse) | >2 mmol/L |
| Mortality | Low/variable | ~10% (SOFA ≥2) | >40% |
| Old term equivalent | SIRS | Severe sepsis | Septic shock |
Key Biomarkers in Sepsis
| Biomarker | Role | Limitation |
|---|---|---|
| Serum lactate | Marker of tissue hypoperfusion; guides resuscitation; part of septic shock definition | Elevated by non-infectious causes; impaired clearance in liver disease |
| Procalcitonin (PCT) | Bacterial infection marker; guides antibiotic de-escalation | Sensitivity 77%, specificity 79% for infection |
| C-reactive protein (CRP) | Acute-phase marker | Sensitivity 75%, specificity 67% - not specific for infection |
| Blood cultures | Identifies pathogen; guides targeted therapy | Positive in only 30-40% of sepsis cases |
Surviving Sepsis Campaign 2021 - Key "1-Hour Bundle"
- Measure lactate - re-measure if >2 mmol/L
- Blood cultures before antibiotics
- Broad-spectrum antibiotics within 1 hour
- 30 mL/kg crystalloid IV for hypotension or lactate ≥4 mmol/L
- Vasopressors (norepinephrine first-line) if hypotension persists - target MAP ≥65 mmHg
Role of metronidazole in hepatic encephalopathy
metronidazole hepatic encephalopathy role mechanism evidence guidelines
"metronidazole" AND "hepatic encephalopathy"
PMID: 41631546
Role of Metronidazole in Hepatic Encephalopathy (HE)
Background: Why Antibiotics in HE?
Mechanism of Action of Metronidazole in HE
- Metronidazole is active against gram-negative anaerobes (e.g., Bacteroides spp.) that possess urease activity
- By reducing the burden of anaerobic bacteria, it decreases urease-mediated conversion of urea to ammonia in the gut
- This reduces both luminal and systemic ammonia levels
- It also has weak activity against Helicobacter pylori, another urease-producing organism implicated in HE
Place in Therapy
| Drug | Position | Evidence |
|---|---|---|
| Lactulose | First-line - initial treatment and secondary prophylaxis | Strong RCT evidence |
| Rifaximin | Second-line - added when lactulose alone insufficient; preferred antibiotic | Strong RCT evidence; superior safety |
| Metronidazole | Third-line / alternative - short-term only | Limited; inferior safety profile |
| Neomycin | Alternative - rarely used now | Nephrotoxicity, ototoxicity |
Evidence for Metronidazole
Key Studies
- Morgan et al. (1982, Gut) - Landmark study: metronidazole 200 mg QID × 7 days was as effective as neomycin in 18 patients with cirrhosis and HE. Both groups showed improvement in mental status (West Haven Criteria), reduction in asterixis, and lower arterial ammonia levels.
- Studies comparing metronidazole to rifaximin showed no significant difference in treatment duration (4.2 ± 2.1 days vs. 3.9 ± 1.7 days) or ammonia reduction - but rifaximin has a better safety profile.
- Mulholland & Greenfield: "Metronidazole for 7 days is as effective as neomycin."
2026 Cochrane Systematic Review (Most Recent Evidence)
Jeyaraj R, et al. Aminoglycosides, vancomycin, and metronidazole for people with cirrhosis and hepatic encephalopathy. Cochrane Database Syst Rev. 2026. [PMID: 41631546]
- 24 RCTs, 1405 participants; 3 trials specifically assessed metronidazole
- Certainty of evidence was low to very low for all comparisons, mainly due to:
- High risk of bias in 22/24 trials
- Small sample sizes
- Significant heterogeneity
- Conclusion: Cannot draw firm conclusions about metronidazole's effects on mortality, HE outcomes, or adverse events compared to other agents due to insufficient evidence quality
AASLD/EASL 2014 Guideline Position
Recommendation 24: "Metronidazole is an alternative choice for treatment of overt hepatic encephalopathy (OHE)." (GRADE II-3, B, 2)
Dosing (When Used)
| Indication | Dose | Duration |
|---|---|---|
| Overt HE (short-term alternative) | 200-250 mg PO 3-4 times daily (800-1000 mg/day) | Short-term only (7 days; max 10-14 days) |
Adverse Effects Limiting Long-Term Use
| Adverse Effect | Details |
|---|---|
| Neurotoxicity ⚠️ | Metronidazole-induced encephalopathy - can mimic or worsen HE; peripheral neuropathy, dizziness, ataxia, seizures |
| Metallic taste | Very common |
| Nausea/vomiting | Common |
| Disulfiram-like reaction | With alcohol (important in alcoholic cirrhosis) |
| Drug interactions | Inhibits CYP2C9 - raises warfarin levels (important in coagulopathic cirrhotic patients) |
Critical point: Metronidazole-induced encephalopathy can be clinically indistinguishable from hepatic encephalopathy itself - making it particularly dangerous in this patient population. Case reports exist of severe encephalopathy in end-stage liver disease patients on metronidazole. The drug accumulates in liver failure due to reduced hepatic clearance.
Why Rifaximin Replaced Metronidazole as the Preferred Antibiotic
| Feature | Metronidazole | Rifaximin |
|---|---|---|
| Absorption | Systemic (well-absorbed) | Minimally absorbed (<0.4%) |
| Spectrum | Anaerobes mainly | Broad-spectrum gut flora |
| Neurotoxicity | Yes - significant | Minimal |
| Nephrotoxicity | No | No |
| Hepatic metabolism | Yes - accumulates in liver failure | Minimal systemic metabolism |
| Long-term use | Unsafe | Safe (RCT evidence up to 6 months) |
| Efficacy | Comparable short-term | Superior in maintenance/prevention |
| Cost | Cheap | Expensive |
Summary
- Metronidazole acts by reducing urease-producing anaerobic gut bacteria and thus lowering ammonia production
- It is as effective as neomycin short-term, but not superior to rifaximin
- It is classified as an alternative/third-line agent in both AASLD/EASL guidelines
- Its use is restricted to short courses (≤7-14 days) due to risk of peripheral neuropathy and encephalopathy - ironic and dangerous in a population already prone to encephalopathy
- In liver failure, metronidazole accumulates due to impaired hepatic metabolism, increasing toxicity risk
- Rifaximin + lactulose remain the standard of care; metronidazole is reserved for situations where rifaximin is unavailable or unaffordable