Osgood shlatter disease
Reading File
Finding Sources
Searching PubMed
"Osgood-Schlatter" disease management
Reading File
Reading File
Reading File
Searching Images
Osgood-Schlatter disease tibial tubercle apophysitis
Reading File
Loading Image
Loading Image
Osgood-Schlatter Disease
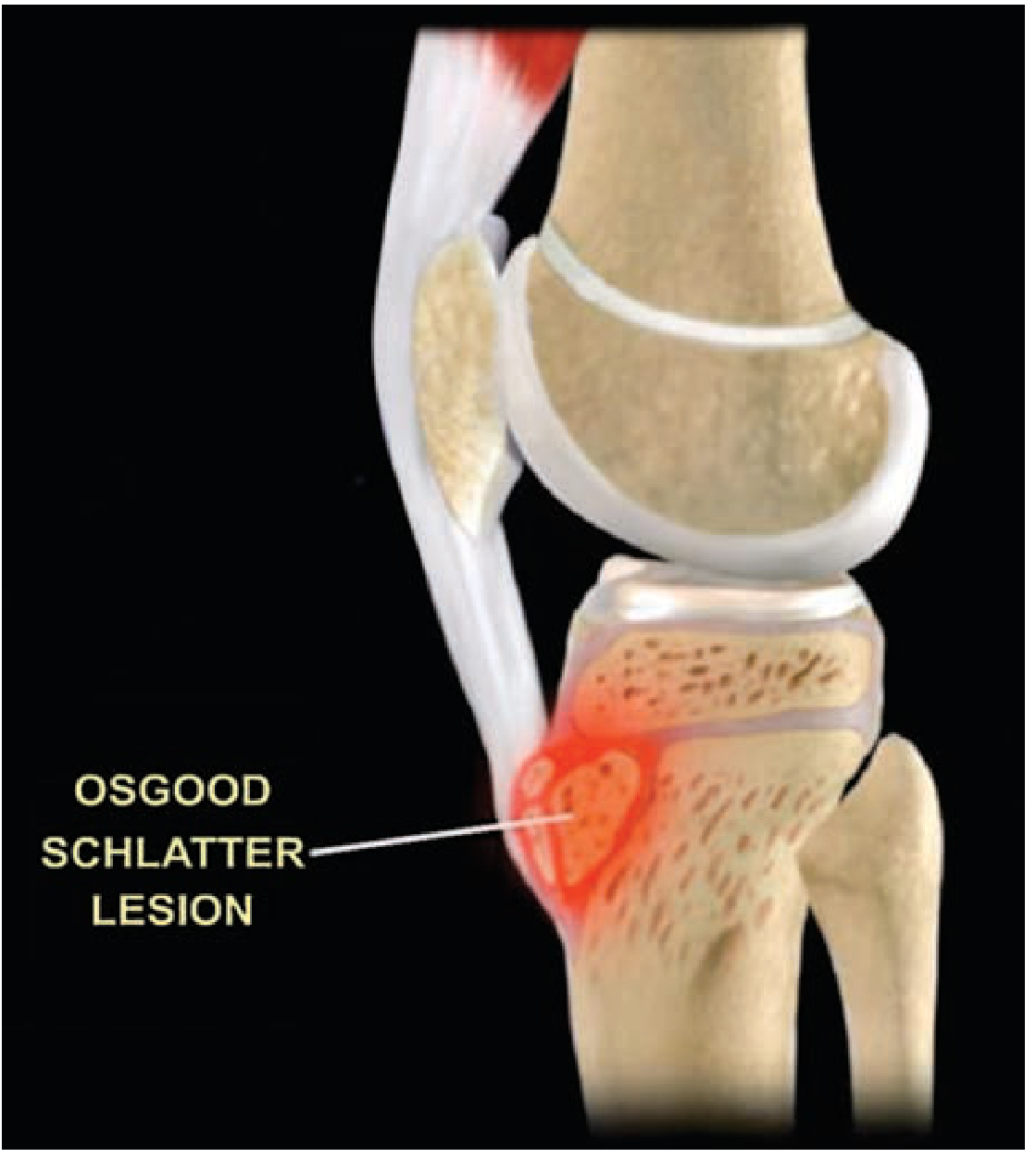
Definition & Pathophysiology
Osgood-Schlatter disease (OSD) is a traction apophysitis of the tibial tubercle caused by repetitive tensile stress from the patellar tendon on its insertion at the tibial tubercle ossification center. The repetitive pull causes a series of microavulsions of the ossification center and underlying cartilage, leading to local inflammation, ossification within the distal patellar tendon, and bony prominence formation. There is no avascular necrosis of the tibial tubercle.
Epidemiology
- Age: Most common in adolescents aged 10–15 years (boys); 8–12 years (girls)
- Sex: Boys more commonly affected
- Activity: Predominantly affects runners, jumpers, sprinters — sports involving repetitive quadriceps contraction
- Bilateral involvement: 20–30% of cases, though symptoms are commonly asymmetric
Clinical Features
| Feature | Detail |
|---|---|
| Pain location | Anterior knee over the tibial tuberosity |
| Pain character | Chronic, intermittent; worsened by running, jumping, kneeling, squatting, climbing stairs |
| Relief | Rest |
| Exam | Bony prominence, soft tissue swelling, tenderness over tibial tubercle; thick tender patellar tendon |
| Knee joint | Otherwise normal — no effusion |
Diagnosis
Diagnosis is clinical — based on history and physical examination. Imaging is not essential but may be obtained.
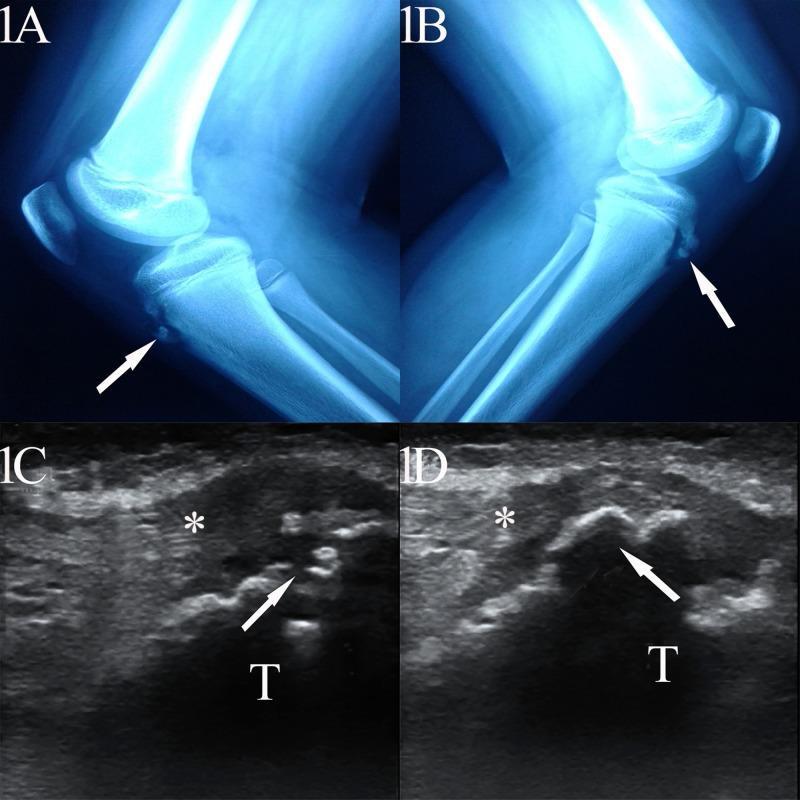
Radiograph (lateral knee):
- Soft tissue swelling anterior to the tibial tubercle
- Irregularity or fragmentation of the tibial tubercle ossification center
- Separate ossicles from the anterior border of the tubercle (chronic stage)
- Blurred margins of the patellar tendon (acute stage)
Ultrasound:
- Pretibial soft tissue swelling
- Fragmentation of the ossification center
- Insertional thickening of the patellar tendon (hypoechoic, loss of fibrillar architecture)
- Fluid in the infrapatellar bursa
Note: Irregularity of tibial tubercle ossification is normal in adolescents — radiographic changes must be correlated clinically.
Treatment
The disease is self-limited — symptoms resolve after closure of the proximal tibial growth plate (skeletal maturity).
Conservative (First-line)
- Activity modification: Limit pain-provoking activities for several months; complete rest is NOT required
- NSAIDs: For pain and swelling
- Ice: After activity to reduce swelling
- Physical therapy: Stretching and strengthening of quadriceps, hamstrings, and gastrocnemius muscles to reduce tendon stress
- Immobilization (cast 3–6 weeks): Only in refractory cases; routine immobilization is contraindicated as it leads to rapid quadriceps atrophy
What NOT to Do
- Do NOT inject corticosteroids into the patellar tendon or para-apophyseal soft tissues
- Do not enforce complete sport restriction
Surgical (Rare)
- Ossicle excision for the ~10% with nonunion of bone fragments who develop persistent anterior knee pain after skeletal maturity, especially with kneeling
Prognosis & Complications
- Majority resolve with conservative treatment
- Symptoms almost universally regress after skeletal maturity
- ~10% nonunion rate → persistent anterior knee pain (especially with kneeling) after adulthood
- Reassurance is key: the condition is benign and self-limited
Key Differentials
- Infrapatellar bursitis: Pain location similar, but tenderness is not localized to tibial tuberosity on palpation
- Sinding-Larsen-Johansson syndrome: Similar apophysitis at the inferior pole of the patella (rather than tibial tuberosity)
- Patellar tendinopathy: Older patients, no bony prominence
- Tibial plateau fracture / avulsion fracture
Sources: Schwartz's Principles of Surgery 11e, p. 1946 | Rosen's Emergency Medicine, p. 3317 | Tintinalli's Emergency Medicine, p. 966
Recent evidence: A 2025 systematic review (PMID 39972530) identified biomechanical alterations in OSD, consistent with the traction apophysitis mechanism described above — no changes to current management recommendations.
This is a shared conversation. Sign in to Orris to start your own chat.