Pharmacology about psvt and treatment
Reading File
Finding Sources
Finding Sources
Searching PubMed
"paroxysmal supraventricular tachycardia" AND treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive information. Let me compile the full answer.
Paroxysmal Supraventricular Tachycardia (PSVT) - Pharmacology and Treatment
Definition and Classification
PSVT is a clinical syndrome characterized by a rapid, regular tachycardia with abrupt onset and termination. The term covers all tachyarrhythmias arising from or involving supraventricular tissue. The three main mechanisms are:
| Type | Frequency | Mechanism |
|---|---|---|
| AV Nodal Reentrant Tachycardia (AVNRT) | ~65% | Reentry within dual AV node pathways |
| AV Reentrant Tachycardia (AVRT) / WPW | ~30% | Reentry via accessory pathway |
| Atrial Tachycardia (AT) | ~5% | Ectopic atrial focus |
- Fuster and Hurst's The Heart, p. 1126
ECG Features
(ECG strip showing PSVT - Tintinalli's Emergency Medicine)

Key ECG features (Table 18-16, Tintinalli's):
- Narrow QRS complex (<100 ms) - unless aberrant conduction
- Rate: typically 170-300 bpm (usually 170-180 bpm)
- No normal sinus P waves - P waves either buried in QRS (~70%) or appear as retrograde P waves immediately adjacent to QRS (in ~30%)
- Abrupt onset and termination
Pathophysiology: The Reentry Circuit
Most PSVT depends on AV nodal conduction as part of the reentry loop:
- In AVNRT, the AV node has dual pathways - a "fast" pathway (short conduction, long refractory) and a "slow" pathway (long conduction, short refractory). A premature atrial contraction can trigger unidirectional block in the fast pathway, allowing a reentry circuit to form.
- In AVRT (WPW), a bypass tract allows antegrade conduction via the AV node and retrograde conduction via the accessory pathway (orthodromic) or vice versa (antidromic).
This AV-node dependence is the key pharmacological target for both termination and prevention.
Treatment Algorithm
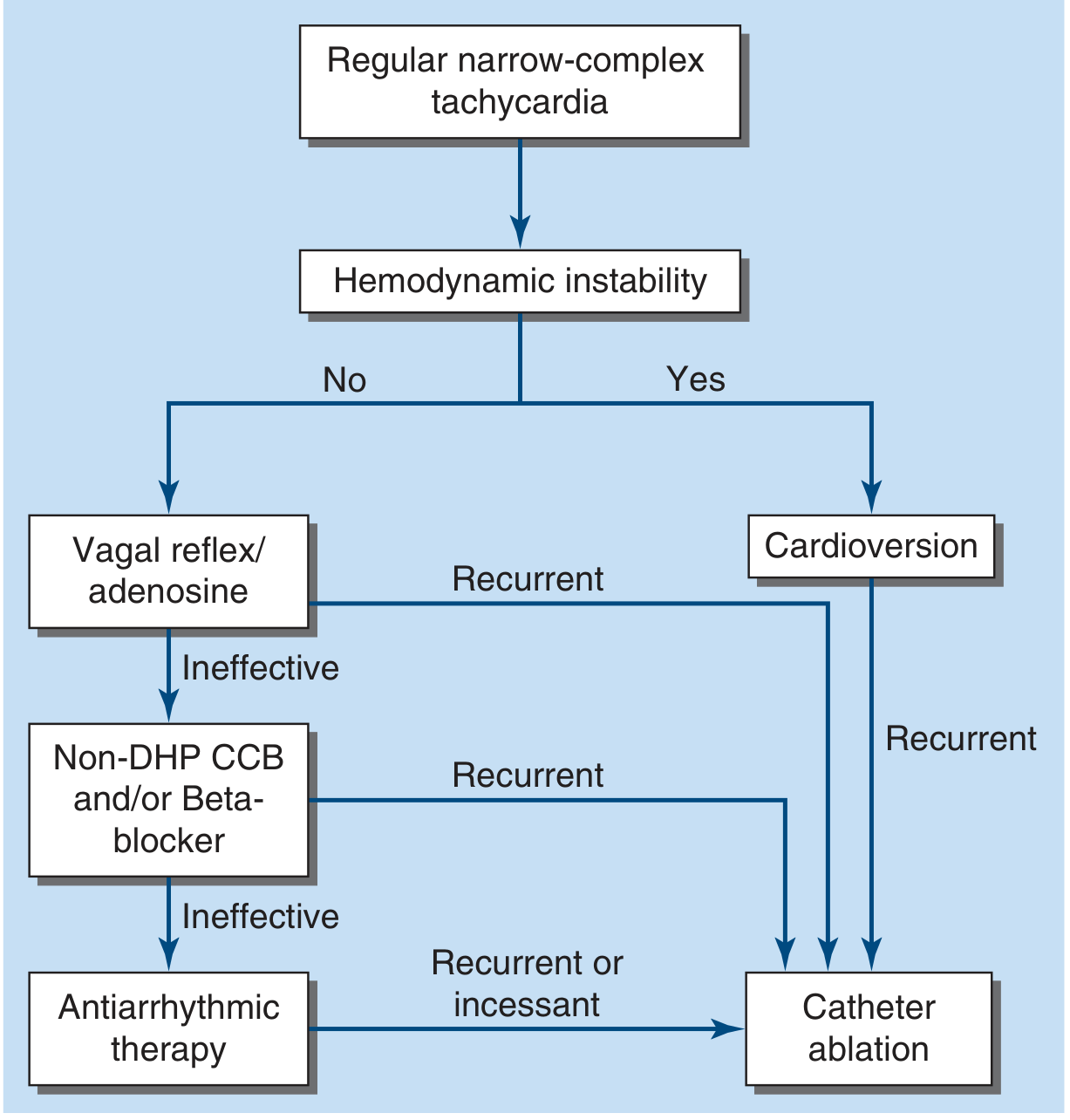
FIGURE 256-6 from Harrison's 22E: Treatment algorithm for hemodynamically stable PSVT
Step 1: Vagal Maneuvers (Non-pharmacologic)
If applied early, vagal maneuvers are often effective:
- Valsalva maneuver - preferred if the patient is cooperative; can be taught for self-management
- Carotid sinus massage - reasonable if no carotid bruits or prior stroke history
- Cold water/ice to face - effective especially in children (diving reflex)
- Modified Valsalva (semi-recumbent, then leg raise) - increases efficacy
Mechanism: increase vagal tone → increase AV nodal refractoriness → interrupt reentry circuit
Step 2: Pharmacological Termination (Acute)
Drug of Choice: ADENOSINE
Mechanism (Katzung's Pharmacology, 16th Ed.):
- Naturally occurring endogenous nucleoside
- Activates inward rectifier K+ current → hyperpolarization
- Inhibits calcium current → suppresses calcium-dependent action potentials
- Directly inhibits AV nodal conduction and increases AV nodal refractory period
- Half-life: <10 seconds in blood
Dose:
- 6 mg IV bolus (rapid push + NS flush) - first dose
- If ineffective: 12 mg IV bolus (can repeat once)
- Given via a large/proximal vein; very short-acting so must be pushed fast
Efficacy: 90-95% conversion to sinus rhythm
Adverse effects:
- Flushing (~20%)
- Dyspnea/chest burning/bronchospasm (>10%) - use cautiously in asthmatics
- Transient chest pain and anxiety
- Brief high-grade AV block (very short-lived due to ultrashort half-life)
- Atrial fibrillation in up to 15% (usually brief) - use with caution in WPW
Contraindications:
- Cardiac transplant recipients (hypersensitivity due to denervation)
- WPW with pre-excited AF (can accelerate conduction via accessory pathway)
Drug interactions:
- Theophylline/caffeine - adenosine receptor blockers → reduce efficacy (need higher dose)
- Dipyridamole - adenosine uptake inhibitor → potentiates effect (reduce dose)
CLASS IV - Non-Dihydropyridine Calcium Channel Blockers
Verapamil
- Mechanism: Blocks L-type Ca2+ channels in AV node → prolongs AV nodal conduction and refractoriness
- Dose: IV 5-10 mg over 2 minutes
- Use: Adenosine or verapamil is preferred over older treatments (propranolol, digoxin, cardioversion) for PSVT termination
- Toxicity: Hypotension (before and after arrhythmia termination), negative inotropy
- WARNING: Never give IV verapamil to VT misdiagnosed as PSVT - can cause hypotension and ventricular fibrillation
- Longer duration of action than adenosine - useful for prevention
Diltiazem
- Similar efficacy to verapamil for SVT management
- IV form available - causes hypotension or bradyarrhythmias less frequently than verapamil
- Also used for rate control in atrial fibrillation and flutter
CLASS II - Beta-Blockers
- IV metoprolol or esmolol can terminate PSVT by blocking sympathetic input to AV node
- Less effective acutely than adenosine or verapamil
- Useful when adenosine/CCBs fail or are contraindicated
- Risk of hypotension (especially combined with CCBs)
- Can be given orally for outpatient "pill-in-the-pocket" or prevention
Digoxin (Historical/Special Situations)
- Increases vagal tone on AV node
- Slow onset - not useful for acute termination
- Was used historically; largely replaced by adenosine and CCBs
- Still occasionally used in heart failure with SVT for rate control
Special Situation: WPW / Pre-excited Tachycardia
DO NOT USE AV nodal blocking agents (adenosine, verapamil, beta-blockers, digoxin) if pre-excited AF is suspected:
- Blocking the AV node forces all conduction through the accessory pathway
- Rapid accessory pathway conduction can cause ventricular fibrillation
For WPW with pre-excited AF:
- DC cardioversion (if hemodynamically unstable)
- Procainamide IV - blocks accessory pathway
- Ibutilide IV - alternative
For orthodromic AVRT (narrow-complex) in WPW, adenosine can be used cautiously.
Wide-Complex PSVT
- Could be PSVT with bundle branch block aberrancy, pre-excited tachycardia, or VT
- Treat as VT until proven otherwise
- If regular and patient is stable: a trial of IV adenosine is reasonable
- Irregular wide-complex tachycardia: likely pre-excited AF/flutter → cardioversion, IV procainamide, or ibutilide
Step 3: Hemodynamic Instability
Synchronized DC cardioversion is the treatment of choice if the patient is:
- Hypotensive with altered consciousness
- In respiratory distress
- Otherwise hemodynamically compromised
Initial energy for PSVT/atrial flutter: 50-100 J (synchronized)
Long-Term Prevention / Outpatient Management
| Option | Details |
|---|---|
| Oral beta-blockers | First-line for prevention; patient can take on as-needed basis |
| Oral CCBs (verapamil/diltiazem) | Alternative; can facilitate termination during Valsalva |
| "Pill-in-the-pocket" | Oral flecainide or diltiazem for episodic self-treatment |
| Catheter ablation | Definitive cure - preferred for recurrent/refractory PSVT; most patients with recurrent episodes are candidates |
Summary Table: Drug Comparison
| Drug | Class | Mechanism | Dose | Efficacy | Key Concern |
|---|---|---|---|---|---|
| Adenosine | Misc. | K+ activation + Ca2+ inhibition | 6 mg → 12 mg IV bolus | 90-95% | Brief AF, bronchospasm; avoid in transplant |
| Verapamil | Class IV | Ca2+ channel block | 5-10 mg IV | High | Hypotension; never in suspected VT |
| Diltiazem | Class IV | Ca2+ channel block | 15-20 mg IV | Similar to verapamil | Less hypotension than verapamil |
| Metoprolol/Esmolol | Class II | Beta blockade | Titrated IV | Moderate | Hypotension, bradycardia |
| Procainamide | Class IA | Na+ channel block | 10-17 mg/kg IV | For WPW/wide-complex | Hypotension, QT prolongation |
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 256
- Katzung's Basic and Clinical Pharmacology, 16th Edition, Chapters 14 & 16
- Fuster and Hurst's The Heart, 15th Edition, Chapter 35
- Tintinalli's Emergency Medicine, Chapter 18
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.