Dequervains ultrasound frequency physiotherapy
Reading File
Finding Sources
Finding Sources
Searching PubMed
de Quervain tenosynovitis ultrasound therapy physiotherapy
Reading File
Finding Sources
Reading Article
PMID: 40662610
Reading Article
PMID: 38613563
Finding Sources
Finding Sources
Searching the Web
de Quervain tenosynovitis therapeutic ultrasound frequency MHz physiotherapy protocol
Reading File
Searching PubMed
therapeutic ultrasound frequency intensity tenosynovitis wrist
Loading Image
Searching PubMed
therapeutic ultrasound 1MHz 3MHz soft tissue healing parameters
Here is a comprehensive answer on therapeutic ultrasound for De Quervain's tenosynovitis, synthesizing textbook content and the latest clinical evidence.
De Quervain's Tenosynovitis — Therapeutic Ultrasound in Physiotherapy
Anatomy Recap
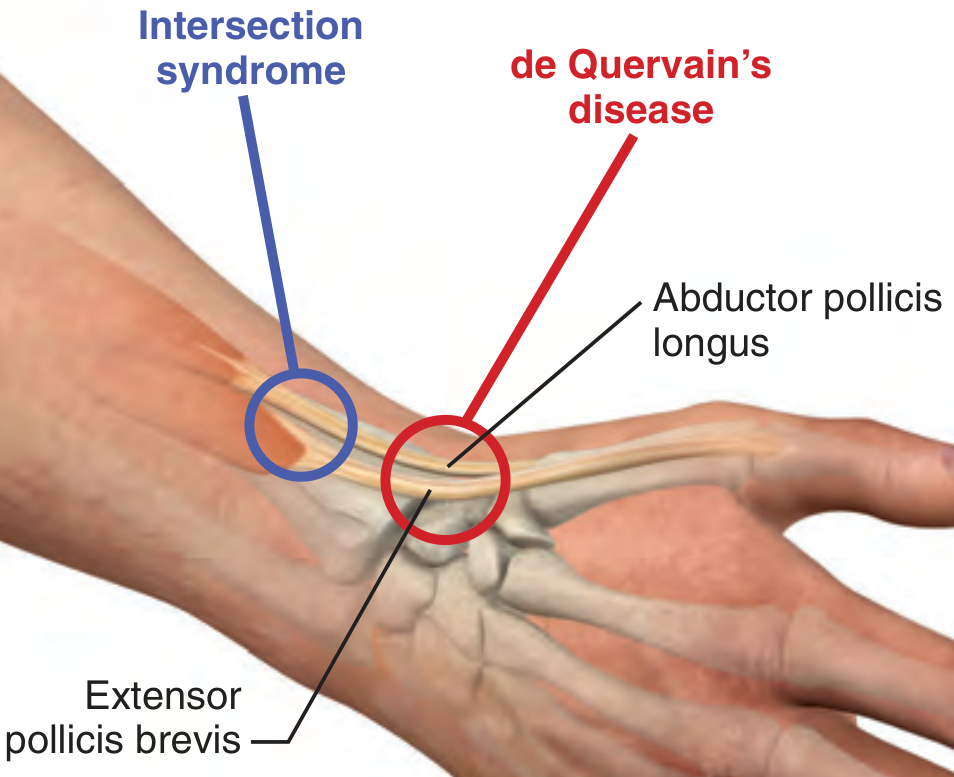
De Quervain's tenosynovitis is stenosing inflammation of the first dorsal compartment of the wrist — specifically the sheaths of the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) at the level of the radial styloid. The condition causes radial-sided wrist/thumb pain, a positive Finkelstein test, and reduced grip strength.
— Roberts and Hedges' Clinical Procedures in Emergency Medicine
Therapeutic Ultrasound (US) Parameters
The textbook library does not contain a dedicated physiotherapy electrophysical agents text, so the following parameters are drawn from well-established physiotherapy principles plus the available clinical trial evidence:
Frequency Selection
| Frequency | Penetration Depth | Best Used For |
|---|---|---|
| 1 MHz | 3–5 cm | Deeper structures, larger areas |
| 3 MHz | 1–2 cm | Superficial structures — preferred for de Quervain's |
The first dorsal wrist compartment is a superficial structure (~0.5–1 cm depth). 3 MHz is therefore the standard frequency choice, as energy is absorbed more efficiently in superficial tissues.
Standard Physiotherapy Protocol for De Quervain's
| Parameter | Recommended Value |
|---|---|
| Frequency | 3 MHz (superficial) |
| Intensity | 0.5–1.5 W/cm² (subacute); 0.5–1.0 W/cm² (chronic) |
| Mode | Pulsed (20–50% duty cycle) in acute/subacute; Continuous in chronic |
| ERA (Effective Radiating Area) | Probe moved slowly, overlapping strokes |
| Duration | 5–8 minutes per session |
| Frequency of sessions | 3–5 times/week |
| Course length | 6–10 sessions (2–3 weeks) |
| Coupling medium | Ultrasound gel; underwater technique may be used |
Rationale for pulsed mode: In the acute/subacute phase, pulsed ultrasound minimises thermal effects while still delivering non-thermal (mechanical/cavitation) effects — including increased membrane permeability, reduced oedema, and accelerated tissue repair.
Evidence Base
2025 RCT — Ultrasound vs Low-Level Laser Therapy (PMID: 40662610)
A single-blind RCT (n=72, 4 weeks, twice weekly) compared therapeutic ultrasound directly with LLLT in De Quervain's. Both groups had significant VAS pain reduction. LLLT showed superior wrist disability reduction at 4 weeks, but ultrasound therapy still produced significant within-group improvements in pain. This positions therapeutic US as an effective, though not the most potent standalone option. Farooq et al., Altern Ther Health Med, 2025
2024 Network Meta-Analysis — Comprehensive Treatment Hierarchy (PMID: 38613563)
14 RCTs across all non-surgical treatments. Key findings for physiotherapy context:
- Extracorporeal shockwave therapy (ESWT) ranked highest in short-to-medium term pain relief
- Corticosteroid injection + casting remains the primary evidence-based treatment
- Laser therapy + orthosis showed favourable outcomes
- Isolated conservative physiotherapy modalities (including ultrasound alone) need to be combined with orthosis/splinting for best results Chong et al., J Hand Surg Am, 2024
Clinical Approach in Physiotherapy
Therapeutic ultrasound for De Quervain's is best used as part of a multimodal programme, not in isolation:
- Thumb spica splint/orthosis — immobilises the first dorsal compartment; reduces mechanical irritation
- Therapeutic ultrasound (3 MHz, pulsed) — reduces synovial sheath inflammation, promotes healing
- Friction/transverse massage — to the tendon sheath (after acute phase)
- Stretching and strengthening — APL/EPB stretches, progressive grip/pinch strengthening
- Activity modification — ergonomic advice, especially for postpartum patients and occupational causes
If conservative physiotherapy fails after 4–6 weeks, corticosteroid injection (with or without splinting) is the next step, followed by surgical release in refractory cases.
Key Takeaway
For therapeutic ultrasound in De Quervain's tenosynovitis:
- Use 3 MHz (superficial structure)
- Pulsed mode in acute/subacute phase; continuous in chronic
- 0.5–1.5 W/cm² intensity
- 5–8 min, 3–5×/week, over 2–3 weeks
- Always combine with splinting; LLLT and ESWT have stronger standalone evidence
This is a shared conversation. Sign in to Orris to start your own chat.