Essay answer on dysphonia plica ventricular is for Ent postgraduate exam and graduate exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Searching PubMed
dysphonia plica ventricularis ventricular fold phonation
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching Images
ventricular fold dysphonia laryngoscopy false vocal cord phonation
Searching the Web
dysphonia plica ventricularis ENT postgraduate essay treatment classification
Loading Image
I have all the material needed. Here is the comprehensive postgraduate essay:
Dysphonia Plica Ventricularis (Ventricular Dysphonia)
Definition
Dysphonia plica ventricularis (DPV), also termed ventricular dysphonia or false cord phonation, is a voice disorder in which the ventricular folds (false vocal cords) participate abnormally in phonation — either by adducting to partially or completely obscure the true vocal folds, or by actually vibrating and themselves generating sound. Because the ventricular folds are thick, poorly compliant, and lack the specialised layered microstructure of the true vocal folds, their participation produces a characteristically rough, low-pitched, strained voice — the hallmark of this condition.
Anatomy Relevant to the Condition
The ventricular folds (vestibular folds / false vocal cords) are paired mucosal folds located immediately superior to the true vocal folds, separated from them by the lateral recess of the ventricle of Morgagni. They consist of a thick submucous layer containing seromucinous glands and loose connective tissue, with no specialised vibratory epithelium. Under normal circumstances they remain stationary during phonation; they close during Valsalva manoeuvres, swallowing, and effort closure but do not contribute to voice production.
The true vocal folds vibrate via the mucosal wave mechanism (Hirano's body-cover model), their layered structure (squamous epithelium → superficial lamina propria [Reinke's space] → intermediate and deep lamina propria → vocalis muscle) allowing efficient mucosal wave propagation. Any disruption of this mechanism can provoke the superior, heavier ventricular folds to compensate.
Aetiology and Classification
DPV is best understood within a two-type classification:
1. Vicarious (Compensatory) Type
Occurs secondary to an organic laryngeal pathology that impairs true vocal fold function. The ventricular folds hypertrophy and adduct as a compensatory mechanism. Causes include:
- Laryngitis (acute or chronic) — most common precipitant; true fold oedema raises the phonation threshold, prompting supraglottic substitution
- Vocal fold paralysis / paresis — unilateral or bilateral; ventricular fold adducts contralaterally to compensate (seen on laryngoscopy as "ventricular show")
- Laryngeal surgery — post-cordectomy, partial laryngectomy, or microlaryngoscopy
- Vocal fold nodules / polyps / cysts — impair mucosal wave, triggering false fold compensation
- Laryngeal web or stenosis
- Reinke's oedema / polypoid degeneration
- Contact ulcers or granulomas
2. Non-Compensatory (Usurpative / Habitual) Type
The ventricular folds assume phonatory function in the absence of significant true vocal fold pathology. Sub-types:
- Habitual: learned maladaptive phonatory behaviour, often arising after an episode of laryngitis that resolved but the abnormal pattern persisted
- Psychoemotional / psychogenic: associated with emotional stress, conversion disorder, or psychosocial upheaval; may present as frank aphonia
- Idiopathic: no identifiable organic or psychological cause
- Occupational: seen in voice professionals who overload the larynx
Koufman & Blalock Classification of Muscle Tension Dysphonia (MTD)
DPV represents the most severe end of the MTD spectrum (Cummings Otolaryngology):
| Class | Features |
|---|---|
| I | Posterior glottal gap, elevated larynx, palpable neck tension; breathy or strident voice |
| II | Lateral-to-medial constriction; false vocal folds adducted; vocal fatigue — plica ventricularis in its most severe form |
| III | Anterior-to-posterior supraglottic constriction; epiglottis and arytenoids obscure ≥50% of laryngeal aditus |
| IV | Epiglottis and arytenoids contact; combined lateral constriction |
— Cummings Otolaryngology Head and Neck Surgery
Pathophysiology
Under normal phonation, the true vocal folds adduct, sub-glottic pressure builds, the Bernoulli effect and tissue elasticity produce rhythmic opening and closing (mucosal wave), generating sound at ~100–300 Hz in adults.
In DPV:
- True fold dysfunction (organic) or habituated supraglottic tension (functional) triggers compensatory medial adduction of the ventricular folds.
- The greater mass of the false folds lowers the fundamental frequency (F0) and produces irregular, aperiodic vibration.
- The result is a rough, low-pitched, strained voice — acoustically characterised by increased jitter, shimmer, and a low harmonics-to-noise ratio.
- A mixed glottal-ventricular phonation pattern may occur, where both true and false folds vibrate simultaneously, producing diplophonia.
- Chronic supraglottic overloading generates a cycle: increased tension → ventricular fold hypertrophy → further obscuration of true folds → worsening phonation.
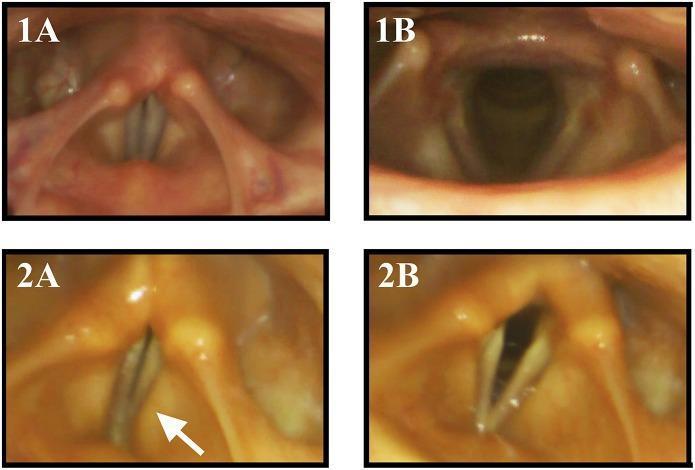
The image below shows flexible laryngoscopy in a patient with neurodegenerative disease: panel 2A (white arrow) demonstrates compensatory medial activation of the vestibular (false) folds during phonation when true vocal fold adduction is insufficient.
Clinical Features
Symptoms
- Voice quality: Constantly harsh, rough, low-pitched, strained voice — often described as a "stage whisper," "croaky," or "throttled" quality
- Pitch: Abnormally low due to the greater mass of false folds (comparable acoustically to Louis Armstrong's singing technique)
- Diplophonia: Two simultaneous pitches when both true and false folds vibrate
- Vocal fatigue: Disproportionate effort required; early fatigue with extended voicing
- Breaks and inconsistency: Intermittent voice loss or pitch breaks
- Neck discomfort or pain: From extrinsic laryngeal muscle overuse
- Normal cough: A key feature — the cough reflex closes the glottis using true fold reflexes, so cough sounds normal, distinguishing DPV from true organic hoarseness
- Sudden onset: Particularly in psychogenic type, often following an URTI or emotional event
Signs on Examination
- Neck palpation: Tenderness over the thyrohyoid space, suprahyoid muscles; larynx may sit elevated
- Larynx elevation on phonation (from strap muscle hypertension)
- Laryngoscopy: False folds closely approximated on phonation, partially or completely obscuring the true vocal folds; the true folds may appear normal when the false folds are displaced
- Videostroboscopy: May reveal partial or complete false fold adduction with disturbed or absent true vocal fold mucosal wave
Diagnosis
A thorough, multimodal assessment is essential.
1. History
- Onset (sudden vs. gradual), precipitating event (URTI, stress, surgery)
- Prior laryngeal disease, surgery, or intubation
- Vocal demands (professional voice user?)
- Psychosocial history
2. Perceptual Voice Assessment
- GRBAS scale: Grade (overall dysphonia), Roughness, Breathiness, Asthenia, Strain
- DPV typically scores high on G, R, S (rough and strained)
3. Laryngoscopy
- Flexible transnasal laryngoscopy: Gold standard for functional assessment; allows evaluation during connected speech without distorting supraglottic posture
- Rigid 70° or 90° telescope with stroboscopy: Best magnification and mucosal wave assessment
- Videostroboscopy: Identifies the pattern of false fold adduction, any underlying true fold pathology, mucosal wave regularity
4. Acoustic Analysis
- Fundamental frequency (F0) — typically low
- Jitter and shimmer — elevated
- Harmonics-to-noise ratio (HNR) — reduced
- Spectrographic analysis shows aperiodic, noisy pattern
5. Aerodynamic Evaluation
- Increased phonation threshold pressure
- Reduced maximum phonation time (MPT)
6. Electromyography (EMG) of the Larynx
- Differentiates DPV from vocal fold paralysis, neurogenic disorders
7. High-Speed Video Laryngoscopy (HSVL) / Laryngeal High-Speed Videoendoscopy (LHSV)
- Can differentiate between adductor spasmodic dysphonia and muscle tension dysphonia (Cummings)
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Adductor spasmodic dysphonia | Neurological; strained-strangled voice with breaks; responds to botulinum toxin |
| Bilateral vocal fold paralysis | EMG/laryngoscopy shows immobile true folds; cough abnormal |
| Puberphonia (mutational falsetto) | High-pitched (not low-pitched); adolescent males; responds to Gutzmann test |
| Laryngeal carcinoma | Mucosal irregularity, irregular margins; must be excluded |
| Psychogenic aphonia | Complete voice loss, not a low-pitched dysphonia; laryngoscopy normal |
| Reinke's oedema | Bilateral polypoid degeneration; more typical of smokers |
Treatment
Management is tailored to the underlying type.
A. Treat Underlying Cause (Vicarious Type)
- Manage laryngitis: voice rest, hydration, mucolytics, treat reflux (PPI)
- Surgical correction of nodules, polyps, cysts, webs → once organic cause is removed, compensatory false fold activity often resolves with voice therapy
- Medialization procedures for vocal fold paralysis (injection laryngoplasty, thyroplasty)
B. Voice Therapy (Primary treatment for non-compensatory type)
This is the cornerstone of management and is curative in the majority of cases.
- Goal: Suppress false fold activity and restore habitual true fold phonation
- Techniques:
- Pushing/pulling exercises to elicit true fold phonation
- Yawn-sigh technique: Relaxes supraglottic tension
- Resonant voice therapy and Lessac-Madsen Resonance Therapy (LMRT)
- Manual circumlaryngeal massage (Aronson; Mathieson): Downward mobilisation of elevated larynx; reduces extrinsic muscle tension
- Vegetative voicing approaches: Using reflexive sounds (laughing, sighing, coughing) to trigger true fold closure habitually
- Confidential voice technique
- Humming: Encourages forward oral resonance, reduces posterior laryngeal tension
- Respiratory re-education: Diaphragmatic support; avoid low lung volume phonation (characteristic in DPV)
- Duration: Usually 6–10 weekly sessions; outcomes generally good for habitual type
C. Psychotherapy / Psychological Support
- For psychogenic DPV, combined psychological counselling with voice therapy is essential
- Cognitive-behavioural therapy (CBT) addresses underlying anxiety, conversion dynamics, or emotional precipitants
- Sudden onset cases (following URTI + stress) often resolve quickly with a single or few voice therapy sessions once the psychological component is addressed
D. Pharmacological Adjuncts
- Botulinum toxin (Botox) injection into the ventricular fold or false cord musculature has been reported for refractory cases — reduces hyperfunctional adduction
- Local anaesthetic injection into the false folds: May transiently relieve false fold spasm and "reset" phonatory pattern
- Treat co-existent reflux (PPIs) and allergy (antihistamines, topical steroids)
E. Surgery (Reserved for Refractory Cases)
- CO₂ laser ventriculoplasty / laser resection of hypertrophied false folds: Used when ventricular fold hypertrophy is the primary obstruction and fails conservative management
- "We describe the successful use of the carbon dioxide laser in the excision of the hypertrophied false vocal cords in a patient who failed conservative management with speech therapy" (PubMed PMID 3813385)
- Not performed for psychogenic type
- Goal is to reduce the bulk of the false folds, allowing true fold visualisation and phonation
Prognosis
- Vicarious DPV: Excellent once the underlying true fold pathology is treated
- Habitual non-compensatory DPV: Good to excellent with voice therapy
- Psychogenic DPV: Good with combined voice and psychological therapy; sudden-onset cases may resolve in one or two sessions
- Idiopathic / refractory DPV: May require botulinum toxin or CO₂ laser surgery; prognosis guarded
Key Points for the Examination
- Definition: False fold phonation in place of true fold phonation — the essence of DPV.
- Two types: Vicarious (compensatory, due to organic true fold disease) vs. Usurpative/Non-compensatory (habitual, psychogenic, idiopathic).
- Voice quality: Rough, low-pitched, strained, harsh — the heavy mass of false folds slows vibration → low F0; aperiodic vibration → roughness.
- Normal cough is the classical clinical clue — true fold reflex closure is preserved.
- Koufman Class II MTD — DPV in its most severe form represents Class II in the Koufman classification.
- Gold standard investigation: Flexible videolaryngoscopy / videostroboscopy.
- Treatment: Voice therapy is first-line for non-compensatory type; treat the cause for vicarious type; CO₂ laser or Botox for refractory cases.
- Differential: Adductor spasmodic dysphonia is the most important differential — distinguished by its neurological basis, specific voice break pattern, and response to botulinum toxin.
- Psychogenic subtype: Predominantly female; sudden onset; often triggered by URTI in context of emotional stress.
Summary
Dysphonia plica ventricularis is a clinically distinctive voice disorder characterised by abnormal ventricular fold participation in phonation, producing a rough, low-pitched, strained voice with a paradoxically normal cough reflex. It ranges from a compensatory response to organic laryngeal disease to a purely functional or psychogenic pattern. Diagnosis requires comprehensive laryngological and voice assessment including videostroboscopy, acoustic analysis, and aerodynamics. Voice therapy remains the cornerstone of treatment for the non-compensatory type, while management of the underlying pathology addresses the vicarious form. Surgical intervention with CO₂ laser resection of hypertrophied false folds is reserved for those who fail conservative measures.
Sources: Cummings Otolaryngology Head and Neck Surgery; Kaplan & Sadock's Comprehensive Textbook of Psychiatry; Ventricular dysphonia: clinical aspects and therapeutic options (PMID 12792323); Laser therapy of dysphonia plica ventricularis (PMID 3813385)
Can you make the whole information given into pdf
Reading File
Running Command
ls -la /home/daytona/workspace/
Running Command
mkdir -p /home/daytona/workspace/dysphonia-essay
Writing File
~/dysphonia-essay/generate_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import cm
from reportlab.lib import colors
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, PageBreak, KeepTogether
)
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
from reportlab.platypus.flowables import HRFlowable
import urllib.request
import os
OUTPUT_PATH = "/home/daytona/workspace/dysphonia-essay/Dysphonia_Plica_Ventricularis.pdf"
# Download the laryngoscopy image
IMG_URL = "https://cdn.orris.care/cdss_images/pmc_clinical_VQA_4ad223539f65e1601ccb70f39912db3d70b7724de4cbd18fe4d4343478d36462.jpg"
IMG_PATH = "/home/daytona/workspace/dysphonia-essay/laryngoscopy.jpg"
try:
urllib.request.urlretrieve(IMG_URL, IMG_PATH)
print("Image downloaded.")
except Exception as e:
print(f"Image download failed: {e}")
IMG_PATH = None
doc = SimpleDocTemplate(
OUTPUT_PATH,
pagesize=A4,
rightMargin=2.2*cm,
leftMargin=2.2*cm,
topMargin=2.2*cm,
bottomMargin=2.2*cm,
title="Dysphonia Plica Ventricularis",
author="ENT Postgraduate Essay"
)
styles = getSampleStyleSheet()
# Custom styles
title_style = ParagraphStyle(
'CustomTitle',
parent=styles['Title'],
fontSize=20,
textColor=colors.HexColor('#1a3a5c'),
spaceAfter=6,
alignment=TA_CENTER,
fontName='Helvetica-Bold'
)
subtitle_style = ParagraphStyle(
'Subtitle',
parent=styles['Normal'],
fontSize=11,
textColor=colors.HexColor('#4a6fa5'),
spaceAfter=14,
alignment=TA_CENTER,
fontName='Helvetica-Oblique'
)
h1_style = ParagraphStyle(
'H1',
parent=styles['Heading1'],
fontSize=13,
textColor=colors.white,
backColor=colors.HexColor('#1a3a5c'),
spaceBefore=14,
spaceAfter=6,
leftIndent=-10,
rightIndent=-10,
borderPad=5,
fontName='Helvetica-Bold'
)
h2_style = ParagraphStyle(
'H2',
parent=styles['Heading2'],
fontSize=11,
textColor=colors.HexColor('#1a3a5c'),
spaceBefore=10,
spaceAfter=4,
fontName='Helvetica-Bold',
borderPad=2,
leftIndent=0,
)
h3_style = ParagraphStyle(
'H3',
parent=styles['Heading3'],
fontSize=10,
textColor=colors.HexColor('#2e6da4'),
spaceBefore=8,
spaceAfter=3,
fontName='Helvetica-BoldOblique'
)
body_style = ParagraphStyle(
'Body',
parent=styles['Normal'],
fontSize=9.5,
leading=14,
spaceAfter=6,
alignment=TA_JUSTIFY,
fontName='Helvetica'
)
bullet_style = ParagraphStyle(
'Bullet',
parent=styles['Normal'],
fontSize=9.5,
leading=13,
spaceAfter=2,
leftIndent=18,
bulletIndent=6,
fontName='Helvetica'
)
sub_bullet_style = ParagraphStyle(
'SubBullet',
parent=styles['Normal'],
fontSize=9,
leading=12,
spaceAfter=2,
leftIndent=36,
bulletIndent=22,
fontName='Helvetica'
)
key_style = ParagraphStyle(
'Key',
parent=styles['Normal'],
fontSize=9.5,
leading=13,
spaceAfter=3,
leftIndent=14,
fontName='Helvetica',
backColor=colors.HexColor('#f0f4f8'),
borderPad=4
)
caption_style = ParagraphStyle(
'Caption',
parent=styles['Normal'],
fontSize=8.5,
textColor=colors.HexColor('#555555'),
alignment=TA_CENTER,
fontName='Helvetica-Oblique',
spaceAfter=8
)
source_style = ParagraphStyle(
'Source',
parent=styles['Normal'],
fontSize=8,
textColor=colors.HexColor('#777777'),
spaceAfter=4,
fontName='Helvetica-Oblique'
)
def section_header(text):
return [
Spacer(1, 4),
Paragraph(f" {text}", h1_style),
Spacer(1, 4)
]
def sub_header(text):
return [Paragraph(text, h2_style)]
def sub_sub_header(text):
return [Paragraph(text, h3_style)]
def body(text):
return Paragraph(text, body_style)
def bullet(text, sub=False):
s = sub_bullet_style if sub else bullet_style
return Paragraph(f"• {text}", s)
def spacer(h=6):
return Spacer(1, h)
story = []
# ─── TITLE BLOCK ─────────────────────────────────────────────────────────────
story.append(spacer(10))
story.append(Paragraph("Dysphonia Plica Ventricularis", title_style))
story.append(Paragraph("(Ventricular Dysphonia / False Cord Phonation)", subtitle_style))
story.append(HRFlowable(width="100%", thickness=2, color=colors.HexColor('#1a3a5c')))
story.append(Paragraph("ENT Postgraduate & Graduate Examination Essay", subtitle_style))
story.append(spacer(10))
# ─── DEFINITION ──────────────────────────────────────────────────────────────
story += section_header("1. Definition")
story.append(body(
"Dysphonia plica ventricularis (DPV), also termed <b>ventricular dysphonia</b> or <b>false cord phonation</b>, "
"is a voice disorder in which the <b>ventricular folds (false vocal cords)</b> participate abnormally in phonation — "
"either by adducting to partially or completely obscure the true vocal folds, or by actually vibrating and "
"themselves generating sound. Because the ventricular folds are thick, poorly compliant, and lack the specialised "
"layered microstructure of the true vocal folds, their participation produces a characteristically rough, low-pitched, "
"strained voice — the hallmark of this condition."
))
# ─── ANATOMY ─────────────────────────────────────────────────────────────────
story += section_header("2. Relevant Anatomy")
story.append(body(
"The <b>ventricular folds</b> (vestibular folds / false vocal cords) are paired mucosal folds located immediately "
"superior to the true vocal folds, separated from them by the lateral recess of the <b>ventricle of Morgagni</b>. "
"They consist of a thick submucous layer containing seromucinous glands and loose connective tissue, with no "
"specialised vibratory epithelium. Under normal circumstances they remain stationary during phonation; they close "
"during Valsalva manoeuvres, swallowing, and effort closure but do not contribute to voice production."
))
story.append(body(
"The <b>true vocal folds</b> vibrate via the mucosal wave mechanism (Hirano's body-cover model), their layered "
"structure — squamous epithelium → superficial lamina propria (Reinke's space) → intermediate and deep lamina "
"propria → vocalis muscle — allowing efficient mucosal wave propagation. Any disruption of this mechanism can "
"provoke the superior, heavier ventricular folds to compensate."
))
# ─── AETIOLOGY & CLASSIFICATION ──────────────────────────────────────────────
story += section_header("3. Aetiology and Classification")
story.append(body(
"DPV is best understood within a <b>two-type classification</b>:"
))
story += sub_header("3.1 Vicarious (Compensatory) Type")
story.append(body(
"Occurs secondary to an organic laryngeal pathology that impairs true vocal fold function. The ventricular folds "
"hypertrophy and adduct as a compensatory mechanism. Causes include:"
))
for item in [
"<b>Laryngitis</b> (acute or chronic) — most common precipitant; true fold oedema raises the phonation threshold, "
"prompting supraglottic substitution",
"<b>Vocal fold paralysis / paresis</b> — unilateral or bilateral; ventricular fold adducts contralaterally to compensate "
"(seen on laryngoscopy as 'ventricular show')",
"<b>Laryngeal surgery</b> — post-cordectomy, partial laryngectomy, or microlaryngoscopy",
"<b>Vocal fold nodules / polyps / cysts</b> — impair mucosal wave, triggering false fold compensation",
"<b>Reinke's oedema / polypoid degeneration</b>",
"<b>Contact ulcers or granulomas</b>",
"<b>Laryngeal web or stenosis</b>",
]:
story.append(bullet(item))
story += sub_header("3.2 Non-Compensatory (Usurpative / Habitual) Type")
story.append(body(
"The ventricular folds assume phonatory function in the absence of significant true vocal fold pathology. Sub-types:"
))
for item in [
"<b>Habitual</b>: Learned maladaptive phonatory behaviour, often arising after an episode of laryngitis that "
"resolved but the abnormal pattern persisted",
"<b>Psychoemotional / psychogenic</b>: Associated with emotional stress, conversion disorder, or psychosocial "
"upheaval; may present as frank aphonia",
"<b>Idiopathic</b>: No identifiable organic or psychological cause",
"<b>Occupational</b>: Seen in voice professionals who overload the larynx",
]:
story.append(bullet(item))
story += sub_header("3.3 Koufman & Blalock Classification of Muscle Tension Dysphonia (MTD)")
story.append(body(
"DPV represents the most severe end of the MTD spectrum. The classification is:"
))
table_data = [
["Class", "Features"],
["I", "Posterior glottal gap, elevated larynx, palpable neck tension; breathy or strident voice"],
["II", "Lateral-to-medial constriction; false vocal folds adducted; vocal fatigue\n— plica ventricularis in its most severe form"],
["III", "Anterior-to-posterior supraglottic constriction; epiglottis and arytenoids obscure ≥50% of aditus"],
["IV", "Epiglottis and arytenoids contact; combined lateral constriction"],
]
table = Table(table_data, colWidths=[1.8*cm, 13.5*cm])
table.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), colors.HexColor('#1a3a5c')),
('TEXTCOLOR', (0,0), (-1,0), colors.white),
('FONTNAME', (0,0), (-1,0), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,-1), 9),
('BACKGROUND', (0,2), (-1,2), colors.HexColor('#dce8f5')),
('ROWBACKGROUNDS', (0,1), (-1,-1), [colors.white, colors.HexColor('#f0f4f8')]),
('GRID', (0,0), (-1,-1), 0.5, colors.HexColor('#aaaaaa')),
('ALIGN', (0,0), (0,-1), 'CENTER'),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('LEFTPADDING', (0,0), (-1,-1), 6),
('RIGHTPADDING', (0,0), (-1,-1), 6),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
('FONTNAME', (0,2), (-1,2), 'Helvetica-Bold'),
]))
story.append(table)
story.append(Paragraph("— Cummings Otolaryngology Head and Neck Surgery", source_style))
story.append(spacer(4))
# ─── PATHOPHYSIOLOGY ─────────────────────────────────────────────────────────
story += section_header("4. Pathophysiology")
story.append(body(
"Under normal phonation, the true vocal folds adduct, sub-glottic pressure builds, and the Bernoulli effect "
"combined with tissue elasticity produces rhythmic opening and closing (mucosal wave), generating sound at "
"~100–300 Hz in adults."
))
story.append(body("In DPV:"))
for item in [
"True fold dysfunction (organic) or habituated supraglottic tension (functional) triggers compensatory medial "
"adduction of the ventricular folds",
"The greater mass of the false folds <b>lowers the fundamental frequency (F0)</b> and produces irregular, aperiodic vibration",
"The result is a <b>rough, low-pitched, strained voice</b> — acoustically characterised by increased jitter, shimmer, "
"and a low harmonics-to-noise ratio",
"A <b>mixed glottal-ventricular phonation</b> pattern may occur, where both true and false folds vibrate simultaneously, "
"producing diplophonia",
"Chronic supraglottic overloading generates a vicious cycle: increased tension → ventricular fold hypertrophy → "
"further obscuration of true folds → worsening phonation",
]:
story.append(bullet(item))
# Add laryngoscopy image
if IMG_PATH and os.path.exists(IMG_PATH):
from reportlab.platypus import Image as RLImage
img = RLImage(IMG_PATH, width=10*cm, height=7*cm)
story.append(spacer(6))
story.append(KeepTogether([
img,
Paragraph(
"Fig. 1: Flexible laryngoscopy. Panel 1A/1B: normal true fold adduction and abduction (control). "
"Panel 2A (white arrow): compensatory medial activation of the false (ventricular) folds during "
"phonation when true vocal fold adduction is insufficient. Panel 2B: incomplete abduction.",
caption_style
)
]))
# ─── CLINICAL FEATURES ───────────────────────────────────────────────────────
story += section_header("5. Clinical Features")
story += sub_header("5.1 Symptoms")
symptoms = [
"<b>Voice quality</b>: Constantly harsh, rough, low-pitched, strained — often described as a 'stage whisper,' "
"'croaky,' or 'throttled' quality",
"<b>Pitch</b>: Abnormally low due to the greater mass of false folds (comparable acoustically to Louis Armstrong's singing)",
"<b>Diplophonia</b>: Two simultaneous pitches when both true and false folds vibrate",
"<b>Vocal fatigue</b>: Disproportionate effort; early fatigue with extended voicing",
"<b>Breaks and inconsistency</b>: Intermittent voice loss or pitch breaks",
"<b>Neck discomfort or pain</b>: From extrinsic laryngeal muscle overuse",
"<b>Normal cough</b>: A key clinical feature — cough reflex closes the glottis using true fold reflexes, "
"so cough sounds normal (distinguishes DPV from true organic hoarseness)",
"<b>Sudden onset</b>: Particularly in psychogenic type, often following an URTI or emotional event",
]
for s in symptoms:
story.append(bullet(s))
story += sub_header("5.2 Signs on Examination")
signs = [
"<b>Neck palpation</b>: Tenderness over the thyrohyoid space and suprahyoid muscles; larynx may sit elevated",
"<b>Larynx elevation</b> on phonation (from strap muscle hypertension)",
"<b>Laryngoscopy</b>: False folds closely approximated on phonation, partially or completely obscuring the true vocal folds",
"<b>Videostroboscopy</b>: May reveal partial or complete false fold adduction with disturbed or absent mucosal wave of true folds",
]
for s in signs:
story.append(bullet(s))
# ─── DIAGNOSIS ───────────────────────────────────────────────────────────────
story += section_header("6. Diagnosis")
story.append(body(
"A thorough multimodal assessment is essential. The following are the key components:"
))
diag_items = [
("History",
"Onset (sudden vs. gradual), precipitating event (URTI, stress, surgery); prior laryngeal disease or surgery; "
"vocal demands (professional voice user?); psychosocial history"),
("Perceptual Voice Assessment",
"GRBAS scale: Grade, Roughness, Breathiness, Asthenia, Strain — DPV typically scores high on G, R, and S"),
("Laryngoscopy",
"Flexible transnasal laryngoscopy (gold standard for functional assessment); rigid 70°/90° telescope with "
"stroboscopy (best magnification and mucosal wave); videostroboscopy identifies false fold adduction pattern"),
("Acoustic Analysis",
"Fundamental frequency (F0) — typically low; Jitter and shimmer — elevated; Harmonics-to-noise ratio (HNR) — "
"reduced; Spectrographic analysis shows aperiodic, noisy pattern"),
("Aerodynamic Evaluation",
"Increased phonation threshold pressure; reduced maximum phonation time (MPT)"),
("Laryngeal EMG",
"Differentiates DPV from vocal fold paralysis and neurogenic disorders"),
("HSVL / LHSV",
"High-speed video laryngoscopy can differentiate adductor spasmodic dysphonia from muscle tension dysphonia"),
]
for title, desc in diag_items:
story.append(Paragraph(f"<b>{title}:</b> {desc}", key_style))
story.append(spacer(3))
story += sub_header("6.1 Differential Diagnosis")
diff_data = [
["Condition", "Distinguishing Feature"],
["Adductor spasmodic dysphonia", "Neurological; strained-strangled voice with breaks; responds to botulinum toxin"],
["Bilateral vocal fold paralysis", "EMG/laryngoscopy shows immobile true folds; cough abnormal"],
["Puberphonia (mutational falsetto)", "High-pitched (not low-pitched); adolescent males; responds to Gutzmann test"],
["Laryngeal carcinoma", "Mucosal irregularity; must always be excluded"],
["Psychogenic aphonia", "Complete voice loss (not low-pitched dysphonia); laryngoscopy normal"],
["Reinke's oedema", "Bilateral polypoid degeneration; more typical in smokers"],
]
diff_table = Table(diff_data, colWidths=[6.5*cm, 9*cm])
diff_table.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), colors.HexColor('#2e6da4')),
('TEXTCOLOR', (0,0), (-1,0), colors.white),
('FONTNAME', (0,0), (-1,0), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,-1), 9),
('ROWBACKGROUNDS', (0,1), (-1,-1), [colors.white, colors.HexColor('#f0f4f8')]),
('GRID', (0,0), (-1,-1), 0.5, colors.HexColor('#aaaaaa')),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('LEFTPADDING', (0,0), (-1,-1), 6),
('RIGHTPADDING', (0,0), (-1,-1), 6),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
]))
story.append(diff_table)
story.append(spacer(6))
# ─── TREATMENT ───────────────────────────────────────────────────────────────
story += section_header("7. Treatment")
story.append(body(
"Management is tailored to the underlying type of DPV."
))
story += sub_header("A. Treat Underlying Cause (Vicarious Type)")
for item in [
"Voice rest, hydration, mucolytics, PPI therapy for laryngitis",
"Surgical correction of nodules, polyps, cysts, webs → once organic cause removed, compensatory activity often resolves with voice therapy",
"Medialization procedures for vocal fold paralysis (injection laryngoplasty, type I thyroplasty)",
]:
story.append(bullet(item))
story += sub_header("B. Voice Therapy (Primary Treatment for Non-Compensatory Type)")
story.append(body(
"<b>Goal:</b> Suppress false fold activity and restore habitual true fold phonation. This is the cornerstone "
"of management and is curative in the majority of cases. Techniques include:"
))
for item in [
"<b>Pushing/pulling exercises</b> to elicit true fold phonation",
"<b>Yawn-sigh technique</b>: Relaxes supraglottic tension",
"<b>Resonant voice therapy</b> and Lessac-Madsen Resonance Therapy (LMRT)",
"<b>Manual circumlaryngeal massage</b> (Aronson; Mathieson): Downward mobilisation of elevated larynx; "
"reduces extrinsic muscle tension",
"<b>Vegetative voicing</b>: Using reflexive sounds (laughing, sighing, coughing) to trigger true fold closure habitually",
"<b>Confidential voice technique</b>",
"<b>Humming</b>: Encourages forward oral resonance, reduces posterior laryngeal tension",
"<b>Respiratory re-education</b>: Diaphragmatic support; avoid low lung volume phonation (characteristic in DPV)",
"Duration: Usually 6–10 weekly sessions; outcomes generally good for habitual type",
]:
story.append(bullet(item))
story += sub_header("C. Psychotherapy / Psychological Support")
for item in [
"For psychogenic DPV, combined psychological counselling with voice therapy is essential",
"Cognitive-behavioural therapy (CBT) addresses underlying anxiety, conversion dynamics, or emotional precipitants",
"Sudden-onset cases following URTI + stress often resolve quickly with one or a few voice therapy sessions",
]:
story.append(bullet(item))
story += sub_header("D. Pharmacological Adjuncts")
for item in [
"<b>Botulinum toxin (Botox) injection</b> into ventricular fold musculature: Used for refractory cases — reduces hyperfunctional adduction",
"<b>Local anaesthetic injection</b> into the false folds: May transiently relieve false fold spasm and 'reset' phonatory pattern",
"Treat co-existent reflux (PPIs) and allergy (antihistamines, topical steroids)",
]:
story.append(bullet(item))
story += sub_header("E. Surgery (Reserved for Refractory Cases)")
for item in [
"<b>CO₂ laser ventriculoplasty / laser resection</b> of hypertrophied false folds: Used when ventricular fold "
"hypertrophy is the primary obstruction and fails conservative management (PMID 3813385)",
"Not performed for psychogenic type",
"Goal: Reduce bulk of false folds, allowing true fold visualisation and phonation",
]:
story.append(bullet(item))
# ─── PROGNOSIS ───────────────────────────────────────────────────────────────
story += section_header("8. Prognosis")
prog_data = [
["Type", "Prognosis"],
["Vicarious (compensatory)", "Excellent once underlying true fold pathology is treated"],
["Habitual non-compensatory", "Good to excellent with voice therapy"],
["Psychogenic", "Good with combined voice and psychological therapy; sudden-onset cases may resolve in 1–2 sessions"],
["Idiopathic / refractory", "May require botulinum toxin or CO₂ laser; prognosis guarded"],
]
prog_table = Table(prog_data, colWidths=[6.5*cm, 9*cm])
prog_table.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), colors.HexColor('#1a3a5c')),
('TEXTCOLOR', (0,0), (-1,0), colors.white),
('FONTNAME', (0,0), (-1,0), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,-1), 9),
('ROWBACKGROUNDS', (0,1), (-1,-1), [colors.white, colors.HexColor('#f0f4f8')]),
('GRID', (0,0), (-1,-1), 0.5, colors.HexColor('#aaaaaa')),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('LEFTPADDING', (0,0), (-1,-1), 6),
('RIGHTPADDING', (0,0), (-1,-1), 6),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
]))
story.append(prog_table)
story.append(spacer(6))
# ─── KEY POINTS ──────────────────────────────────────────────────────────────
story += section_header("9. Key Points for the Examination")
key_points = [
("Definition", "False fold phonation in place of true fold phonation — the essence of DPV."),
("Two types", "Vicarious (compensatory, due to organic true fold disease) vs. Usurpative/Non-compensatory (habitual, psychogenic, idiopathic)."),
("Voice quality", "Rough, low-pitched, strained, harsh — heavy mass of false folds slows vibration → low F0; aperiodic vibration → roughness."),
("Normal cough", "Classical clinical clue — true fold reflex closure is preserved despite dysphonic voice."),
("Koufman Class II MTD", "DPV in its most severe form represents Class II in the Koufman classification of muscle tension dysphonia."),
("Gold standard investigation", "Flexible videolaryngoscopy / videostroboscopy."),
("Treatment", "Voice therapy is first-line for non-compensatory type; treat the cause for vicarious type; CO₂ laser or Botox for refractory cases."),
("Key differential", "Adductor spasmodic dysphonia — distinguished by neurological basis, specific voice break pattern, and response to botulinum toxin."),
("Psychogenic subtype", "Predominantly female; sudden onset; often triggered by URTI in context of emotional stress."),
]
kp_data = [[f"{i+1}. {k}", v] for i, (k, v) in enumerate(key_points)]
kp_table = Table(kp_data, colWidths=[5*cm, 10.5*cm])
kp_table.setStyle(TableStyle([
('FONTNAME', (0,0), (0,-1), 'Helvetica-Bold'),
('FONTNAME', (1,0), (1,-1), 'Helvetica'),
('FONTSIZE', (0,0), (-1,-1), 9),
('ROWBACKGROUNDS', (0,0), (-1,-1), [colors.HexColor('#dce8f5'), colors.HexColor('#f0f4f8')]),
('GRID', (0,0), (-1,-1), 0.5, colors.HexColor('#aaaaaa')),
('VALIGN', (0,0), (-1,-1), 'TOP'),
('LEFTPADDING', (0,0), (-1,-1), 6),
('RIGHTPADDING', (0,0), (-1,-1), 6),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
]))
story.append(kp_table)
story.append(spacer(8))
# ─── SUMMARY ─────────────────────────────────────────────────────────────────
story += section_header("10. Summary")
story.append(body(
"Dysphonia plica ventricularis is a clinically distinctive voice disorder characterised by abnormal ventricular "
"fold participation in phonation, producing a rough, low-pitched, strained voice with a paradoxically <b>normal "
"cough reflex</b>. It ranges from a compensatory response to organic laryngeal disease to a purely functional or "
"psychogenic pattern. Diagnosis requires comprehensive laryngological and voice assessment including "
"videostroboscopy, acoustic analysis, and aerodynamics. <b>Voice therapy remains the cornerstone of treatment</b> "
"for the non-compensatory type, while management of the underlying pathology addresses the vicarious form. "
"Surgical intervention with CO₂ laser resection of hypertrophied false folds is reserved for those who fail "
"conservative measures."
))
# ─── SOURCES ─────────────────────────────────────────────────────────────────
story.append(HRFlowable(width="100%", thickness=1, color=colors.HexColor('#aaaaaa')))
story.append(Paragraph(
"<i>Sources: Cummings Otolaryngology Head and Neck Surgery; Kaplan & Sadock's Comprehensive Textbook of Psychiatry; "
"Ventricular dysphonia: clinical aspects and therapeutic options (PMID 12792323); "
"Laser therapy of dysphonia plica ventricularis (PMID 3813385)</i>",
source_style
))
# Build PDF
doc.build(story)
print(f"PDF saved to: {OUTPUT_PATH}")
Running Command
cd /home/daytona/workspace/dysphonia-essay && python generate_pdf.py 2>&1
Running Command
ls -lh /home/daytona/workspace/dysphonia-essay/Dysphonia_Plica_Ventricularis.pdf
Your PDF is ready. Here's the download link:
Dysphonia Plica Ventricularis
PDF Document · PDF
The PDF includes:
- Formatted title page with full essay heading
- All 10 sections — Definition, Anatomy, Aetiology & Classification, Pathophysiology, Clinical Features, Diagnosis, Treatment, Prognosis, Key Points, and Summary
- Koufman MTD classification table with Class II highlighted
- Differential diagnosis table
- Prognosis table
- Key examination points table
- Laryngoscopy image (Fig. 1 showing ventricular fold compensation)
- Source citations at the footer
This is a shared conversation. Sign in to Orris to start your own chat.