Inflammatory bowel syndrome
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"inflammatory bowel disease"[MeSH Terms] AND ("Crohn disease"[MeSH Terms] OR "colitis, ulcerative"[MeSH Terms])
Searching the Web
inflammatory bowel disease IBD Crohn's ulcerative colitis overview 2025
Reading File
Searching Images
inflammatory bowel disease Crohn's ulcerative colitis pathology comparison
Searching PubMed
"inflammatory bowel disease" AND treatment
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of Inflammatory Bowel Disease (IBD).
Inflammatory Bowel Disease (IBD)
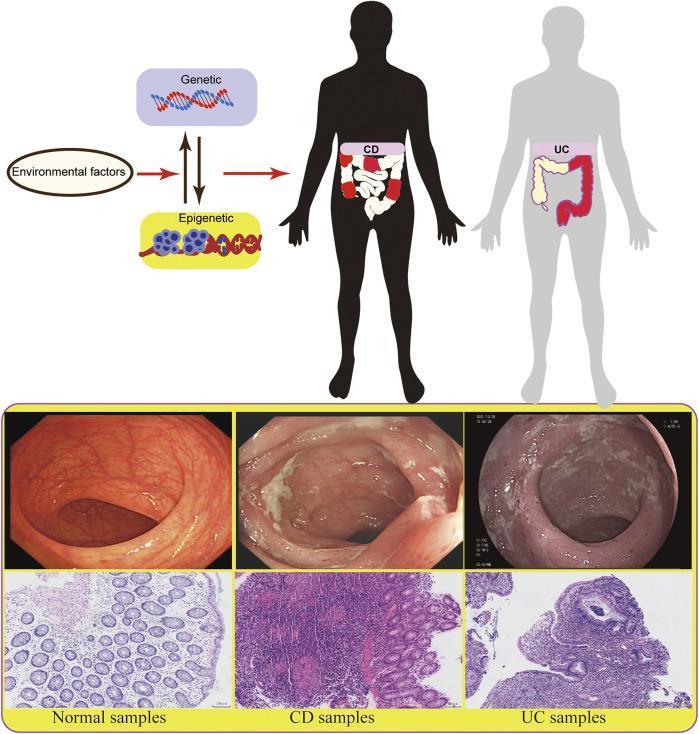
IBD is a chronic, relapsing-remitting inflammatory condition of the gastrointestinal tract. It comprises two main subtypes — Crohn's disease (CD) and Ulcerative colitis (UC) — plus a less common category, indeterminate colitis, used when histology doesn't clearly distinguish the two.
Epidemiology & Etiology
IBD results from a dysregulated immune response in a genetically susceptible host, triggered by environmental and microbial factors. Key contributors:
- Genetics: >200 susceptibility loci identified; NOD2 mutations are the strongest known risk factor for CD
- Microbiome: Dysbiosis with reduced microbial diversity
- Environmental triggers: Western diet, smoking (protective in UC, harmful in CD), appendectomy (protective in UC), NSAIDs, antibiotics
- Peak onset: CD — ages 15–30 (with a second peak in the 7th decade); UC — ages 20–40
Key Distinguishing Features
| Feature | Crohn's Disease | Ulcerative Colitis |
|---|---|---|
| GI extent | Esophagus to anus ("mouth to anus") | Colon only |
| Pattern | Skip lesions (discontinuous) | Continuous, starting from rectum |
| Depth | Transmural (all bowel layers) | Mucosal/submucosal only |
| Ulceration | Discrete, aphthous → cobblestoning | Continuous, diffuse erythema |
| Fistulas/strictures | Common | Rare |
| Perianal disease | Common (20–40%) | Absent |
| Rectal involvement | ~60% | Always (hallmark) |
| Granulomas | Noncaseating (pathognomonic if present) | Absent |
(Goldman-Cecil Medicine, Table 127-1)
Clinical Manifestations
Crohn's Disease
The terminal ileum is affected in ~70% of patients. Presentations:
- Ileocolonic (most common, 40%): RLQ pain, diarrhea, weight loss, hematochezia
- Ileal only (30%): Obstructive symptoms — distension, nausea, cramping
- Perianal (up to 30%): Fistulas, abscesses, fissures, skin tags with pain and discharge
- Upper GI (<5%): Dysphagia, odynophagia, heartburn
- Fistulas (enterocutaneous, rectovaginal, enterovesicular) occur in 20–40% of patients
Ulcerative Colitis
- Hematochezia, bloody diarrhea, tenesmus, urgency, excessive mucus production
- In proctitis/proctosigmoiditis: paradoxical constipation with difficulty defecating
- Severe/extensive disease: weight loss, fever, hypoalbuminemia, peripheral edema
- At diagnosis: ~14–37% have pancolitis; ~44–49% have proctosigmoiditis
Extraintestinal Manifestations
| System | Manifestations |
|---|---|
| Musculoskeletal | Peripheral arthritis/arthralgia, ankylosing spondylitis, sacroiliitis (10–20%) |
| Dermatologic | Erythema nodosum (10–15%), pyoderma gangrenosum (1–2%) |
| Ocular | Uveitis, episcleritis (5–15%) |
| Hepatobiliary | Primary sclerosing cholangitis (2–7.5% of IBD; 70–80% of PSC patients have underlying IBD) |
| Renal | Calcium oxalate stones (fat malabsorption in CD), uric acid stones |
(Goldman-Cecil Medicine, Table 127-2)
Diagnosis
Endoscopy + biopsy is the cornerstone. Key findings:
- Crohn's: Aphthous ulcers early → deep linear/serpiginous ulcers → cobblestoning; skip areas; possible small bowel or upper GI involvement. Noncaseating granulomas on biopsy (rarely seen on endoscopic samples, but pathognomonic)
- UC: Diffuse mucosal erythema starting at the rectum → granular, edematous mucosa → friability → ulceration; continuous proximal spread; pseudopolyps in long-standing disease
- Histology (UC): Crypt distortion, lymphocytic infiltrate, crypt abscesses
- Imaging: CT/MR enterography for small bowel involvement in CD; can show mural thickening, "comb sign" (engorged mesenteric vessels), fat stranding
Treatment
Step-Up Approach
| Tier | Agents | Use |
|---|---|---|
| Aminosalicylates (5-ASA) | Mesalamine, sulfasalazine | Mild–moderate UC; maintenance |
| Corticosteroids | Prednisone, budesonide | Induction of remission (not maintenance) |
| Immunomodulators | Azathioprine, 6-MP, methotrexate | Maintenance; steroid-sparing |
| Anti-TNF-α biologics | Infliximab, adalimumab, certolizumab (CD), golimumab (UC) | Moderate–severe disease; fistulizing CD |
| Anti-integrins | Vedolizumab | Gut-selective; moderate–severe UC & CD |
| IL-12/23 inhibitors | Ustekinumab | Moderate–severe CD (also UC) |
| JAK inhibitors | Tofacitinib, upadacitinib | Moderate–severe UC |
Anti-TNF Biologics (key pharmacology)
- Infliximab (IV): 5 mg/kg at 0, 2, 6 weeks → every 8 weeks maintenance; chimeric (25% mouse/75% human); t½ ~8–10 days
- Adalimumab (SC): 160 mg → 80 mg at wk 2 → 40 mg every 2 weeks; fully humanized; t½ ~2 weeks
- Certolizumab pegol (SC): PEGylated Fab fragment; 400 mg at 0, 2, 4 weeks → every 4 weeks
- Golimumab (SC): For UC; fully humanized; t½ ~14 days
- Major adverse effect: serious infections (including TB reactivation — screen before initiation); risk of lymphoma with long-term use
(Goodman & Gilman's Pharmacological Basis of Therapeutics)
Surgery
- UC: Colectomy is curative — indicated for refractory disease, toxic megacolon, dysplasia/cancer
- CD: Not curative; surgery for strictures, fistulas, abscesses, or medically refractory disease; bowel-preserving resection preferred
Complications & Cancer Risk
- Colorectal cancer (CRC): Risk begins after ~7 years of UC; rises ~10% per decade, reaching 15–34% at 30 years. Risk correlates with disease extent and duration. CD also increases CRC risk 4–20×
- Toxic megacolon: Severe, life-threatening complication primarily in UC
- Dysplasia surveillance: Colonoscopy every 1–2 years after 8–10 years of pancolitis
- Osteoporosis: From chronic corticosteroid use and malabsorption
- Thromboembolism: IBD is a prothrombotic state — increased DVT/PE risk during flares
Recent Evidence
A 2024 AGA network meta-analysis (PMID 39425738) synthesized comparative efficacy of advanced therapies for moderate-to-severe UC, supporting individualized biologic and small-molecule selection. The BSG IBD Guideline 2025 incorporates the latest network meta-analysis data on induction and maintenance agents for both CD and UC.
Sources: Goldman-Cecil Medicine 26e, Ch. 127 | Goodman & Gilman's Pharmacological Basis of Therapeutics, Ch. 55 | Sleisenger & Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.