Hyponatremia and Hypernatremia diagnosis and management? 10 marks for anesthesia DNB exam from standard source
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
I now have very comprehensive material from Miller's Anesthesia and Rosen's Emergency Medicine. Let me compile the full answer for the DNB exam.
Hyponatremia and Hypernatremia - Diagnosis and Management
(Miller's Anesthesia 10e; Rosen's Emergency Medicine 10e)
HYPONATREMIA
Definition and Classification
Hyponatremia = serum Na⁺ <135 mEq/L. Classified as:
| Severity | Na⁺ Level |
|---|---|
| Mild | 130-134 mEq/L |
| Moderate | 120-130 mEq/L |
| Severe | <120 mEq/L |
Moderate-to-severe hyponatremia, especially of acute onset, is associated with significant perioperative morbidity and mortality.
Pathophysiology
Na⁺ is the primary determinant of serum osmolality. Hyponatremia results from imbalanced gains or losses of total body water (TBW) and Na⁺ such that serum Na⁺ concentration falls. Three broad mechanisms:
- Decreased TBW and Na⁺ with relatively greater loss of Na⁺ - hypovolemic
- Increased TBW with near-normal Na⁺ - euvolemic
- Increased TBW and Na⁺ with relatively greater increase in TBW - hypervolemic
Diagnosis - The Diagnostic Algorithm
The key diagnostic approach uses three sequential steps:
Step 1 - Serum Osmolality
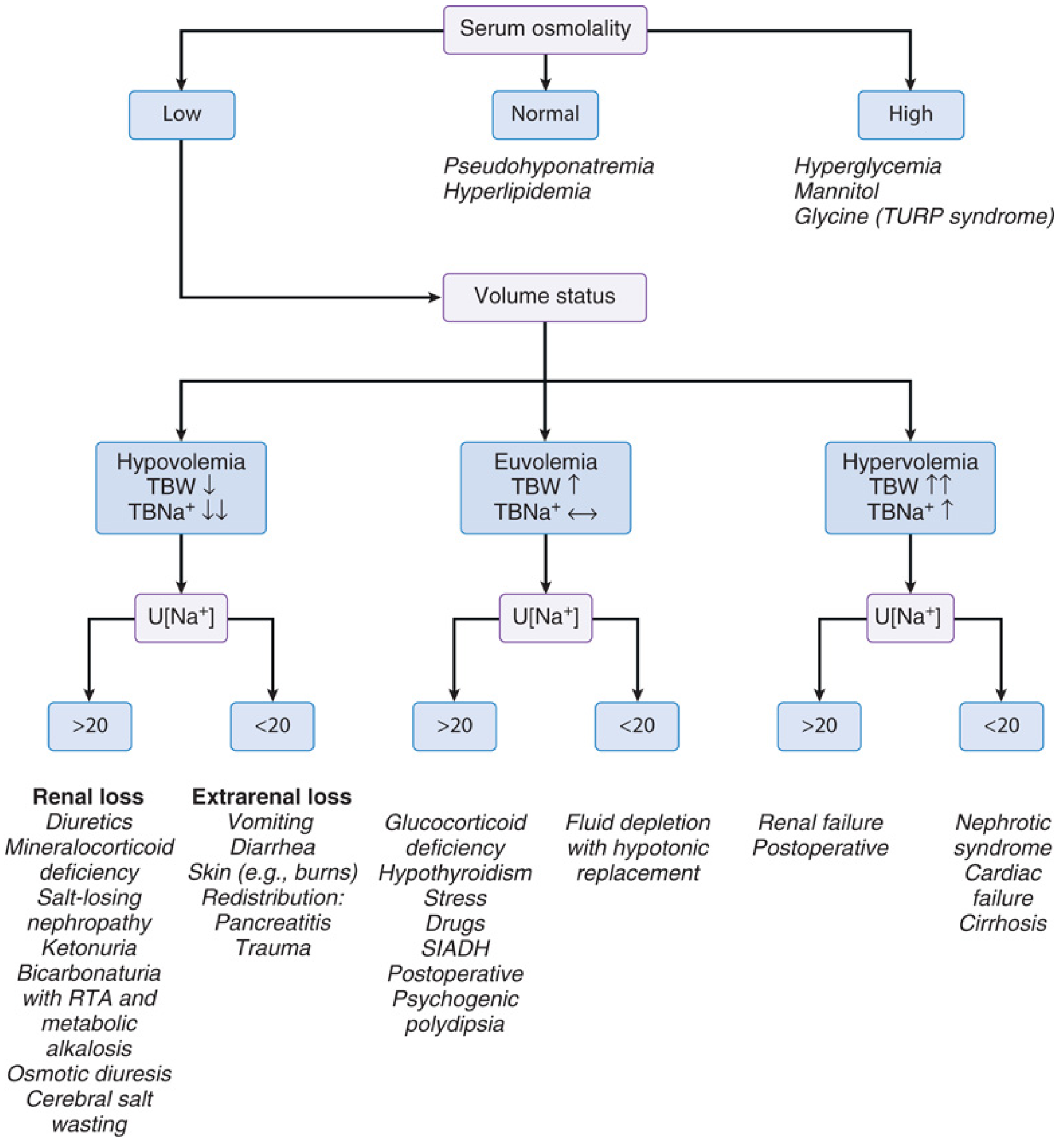
(Fig. 43.3 - Miller's Anesthesia 10e)
- Normal osmolality (280-295 mOsm/kg) - Pseudohyponatremia (hyperlipidemia, hyperproteinemia)
- High osmolality (>295 mOsm/kg) - Dilutional: hyperglycemia, mannitol, glycine (TURP syndrome)
- Low osmolality (<280 mOsm/kg) - True hyponatremia; proceed to Step 2
Step 2 - Volume Status (TBW assessment)
Assess clinically: skin turgor, mucous membranes, JVP, edema, orthostasis
Step 3 - Urinary Na⁺ Concentration
| Volume Status | U[Na⁺] <20 mEq/L | U[Na⁺] >20 mEq/L |
|---|---|---|
| Hypovolemic | Extrarenal loss (vomiting, diarrhea, burns, pancreatitis) | Renal loss (diuretics, mineralocorticoid deficiency, salt-losing nephropathy, RTA, osmotic diuresis, cerebral salt wasting) |
| Euvolemic | Fluid depletion with hypotonic replacement, psychogenic polydipsia | SIADH, hypothyroidism, glucocorticoid deficiency, stress, drugs, postoperative |
| Hypervolemic | Nephrotic syndrome, cardiac failure, cirrhosis | Renal failure, postoperative |
SIADH Diagnostic Criteria:
- Serum hypoosmolality (<270 mOsm/kg)
- Clinical euvolemia
- Urinary Na⁺ inappropriately elevated despite normal water/salt intake
- Inappropriate urinary concentration (>100 mOsm/kg)
- Exclude: adrenal, thyroid, renal disease, diuretic use
- Characteristic response to water restriction: 2-3 kg fall in weight + reduction in salt wasting over 2-3 days
Clinical Features
Symptoms are related to cerebral edema and increased ICP, highly dependent on rate of development:
- Na⁺ 120-125 mEq/L (acute): Headache, confusion, agitation, nausea, vomiting, lethargy (threshold lower in children and premenopausal females - symptoms may occur at Na⁺ as high as 128 mEq/L)
- Na⁺ <110 mEq/L: Seizures, coma, brainstem herniation
- Chronic hyponatremia: May be asymptomatic even at Na⁺ <120 mEq/L due to brain osmotic adaptation
Anesthesia-Specific Considerations
Preoperative Hyponatremia:
- Even mild preoperative hyponatremia is associated with increased 30-day mortality, major cardiac events, wound infection, and pneumonia - even in ASA class 1-2 patients
- Correcting preoperative hyponatremia does NOT clearly improve outcomes; it should prompt a search for underlying disease
- Moderate-to-severe hyponatremia: postpone non-urgent surgery for gradual correction
Postoperative Hyponatremia:
- Incidence: 1-5%
- Mechanism: Surgical stress response causes Na⁺ and water retention (SIADH-like state) + administration of hypotonic IV fluids
- Children and premenopausal females are at highest risk for neurologic symptoms (symptoms at Na⁺ as high as 128 mEq/L)
- 8% of hyponatremic patients develop encephalopathy; 52% of those suffer permanent neurologic sequelae or death
- Prevention: Limit free water to 1-1.2 mL/kg/h, replace GI losses with isotonic solution, stop IV therapy when oral route is available, monitor electrolytes frequently
TURP Syndrome (anesthesia-specific):
- Symptomatic hyponatremia + excessive intravascular volume from absorption of hypotonic irrigation fluid (glycine, sorbitol, mannitol) during TURP, bladder resection, hysteroscopy
- Complicates 10-15% of TURP procedures; onset 15 min to 24 hours post-resection
- Risk factors: increased intravesical pressure, prolonged resection, hypotonic irrigants, open venous sinuses
- Prevention: bipolar diathermy with isotonic saline irrigant; monitor fluid absorption (intake vs. output)
Management
Core principle: Rate of Na⁺ correction must not exceed 10 mEq/L in the first 24 hours (to prevent osmotic demyelination syndrome / central pontine myelinolysis).
Osmotic Demyelination Syndrome (ODS):
- Caused by rapid correction of chronic hyponatremia
- Neurons depleted of Na⁺ and K⁺ to limit intracellular osmolality; rapid rise in ECF Na⁺ causes fluid to shift OUT of neurons causing diffuse demyelination
- Risk factors: chronic hyponatremia >48 hours, hypokalemia, malnutrition, alcoholism, liver disease
| Type | Management |
|---|---|
| Hypovolemic hyponatremia | Restore ECF volume with isotonic saline (reduces ADH release; symptoms unusual as brain adaptation limits edema) |
| Hypervolemic hyponatremia | Water restriction + treat underlying disease (ACE inhibitors for cardiac failure); loop diuretics (NOT thiazides) to excrete free water |
| Euvolemic/SIADH - chronic asymptomatic | Fluid restriction; treat underlying cause; ADH antagonists (demeclocycline, lithium); loop diuretics; tolvaptan (V2 receptor antagonist) |
| Moderate symptomatic (confusion, nausea) | 3% hypertonic saline at 1 mL/kg/h - aim to raise Na⁺ by 1 mEq/L/h for 3-4 hours; then reassess; limit total rise to ≤10 mEq/L/24h |
| Severely symptomatic (seizures, coma, Na⁺ <120 mEq/L) | Bolus 100 mL of 3% saline - aim to raise Na⁺ by 2-3 mEq/L acutely; repeat once or twice at 10-min intervals if no neurological improvement; then continue as moderate symptomatic protocol (≤10 mEq/L/24h); recheck electrolytes and osmolality every few hours |
HYPERNATREMIA
Definition and Classification
Hypernatremia = serum Na⁺ >145 mEq/L
- Affects up to 10% of critically ill patients
- Severe (Na⁺ >160 mEq/L): associated with 75% mortality (dependent on severity of underlying disease)
Pathophysiology - Three Mechanisms
- Excessive water loss with inadequate compensatory intake (most common)
- Lack of ADH action - Diabetes Insipidus (DI)
- Exogenous sodium administration
Types by Volume Status:
| Type | TBW | TBNa⁺ | Causes |
|---|---|---|---|
| Hypovolemic (dehydration + low TBNa⁺) | Decreased | Decreased more | Heatstroke, burns, sweating, GI losses, osmotic diuresis |
| Euvolemic (normal TBNa⁺) | Decreased | Normal | Diabetes insipidus (central or nephrogenic), insensible losses, fever |
| Hypervolemic (increased TBNa⁺) | Increased | Increased more | Hypertonic saline, NaHCO₃ administration, mineralocorticoid excess |
Diabetes Insipidus:
- Central DI: Impaired ADH production or release - pituitary surgery, subarachnoid hemorrhage, traumatic brain injury (skull base fractures), brainstem death
- Nephrogenic DI: Reduced renal sensitivity to ADH - renal disease, electrolyte disorders, drugs (lithium, foscarnet, amphotericin B, demeclocycline)
Diagnosis
Step 1 - Assess clinical volume status (hypovolemic/euvolemic/hypervolemic)
Step 2 - Calculate Water Deficit
TBW deficit = TBW × (serum Na⁺ - 140) / 140
Where TBW (L) = body weight (kg) × correction factor:
- Adult males: 0.6
- Adult females: 0.5
- Elderly males: 0.5
- Elderly females: 0.45
Step 3 - Urine Studies
- Serum osmolality, urine osmolality, urine Na⁺ concentration
- In DI: Urine output >100 mL/h + urine osmolality <300 mOsm/kg with high serum osmolality >305 mOsm/kg
- Urine specific gravity <1.005 + hypernatremia = consistent with DI
- Central vs. Nephrogenic DI: Administer desmopressin (DDAVP) - central DI responds with urine concentration; nephrogenic DI does not respond
Clinical Features
- Altered mental status, lethargy, irritability
- Seizures, hyperreflexia, spasticity
- Polyuria, polydipsia (in DI)
- Risk groups: elderly (impaired thirst), infants, comatose patients, intubated/paralyzed patients
Management
Core principle: Correct Na⁺ by no more than 10 mEq/L/day (same as hyponatremia) - rapid correction can cause cerebral edema as neurons have adapted by accumulating osmoles.
Three Interdependent Goals:
- Rapidly correct underlying shock/hypoperfusion with normal (isotonic) saline first
- Treat the underlying cause (insulin for hyperglycemia; DDAVP for central DI)
- Carefully lower serum Na⁺ by replacing total water deficit
| Type | Management |
|---|---|
| Hypovolemic hypernatremia | First: isotonic saline to correct intravascular volume deficit and treat underlying cause (e.g., insulin for hyperglycemia); Then: replace water deficit with 0.45% saline, 5% dextrose, or enteral water |
| Euvolemic hypernatremia | Replace water deficit with 0.45% saline, 5% dextrose, or enteral water to cover deficit + ongoing losses. For central DI with urine output >250 mL/h: titrated IV desmopressin (DDAVP) 0.4-1 mcg - caution with higher doses (prolonged effect, risk of water intoxication) |
| Hypervolemic hypernatremia | Stop exogenous Na⁺ source; give furosemide + 5% dextrose or enteral water. Dialysis if renal failure present |
Disposition: Almost all hypernatremic patients require hospitalization. Mild cases with intact thirst and access to water may be managed with increased oral water intake.
KEY MNEMONICS AND EXAM POINTS
Hyponatremia - "3 Osmolality, 3 Volumes, 20 mEq Rule"
- Measure serum osmolality first to exclude pseudo/dilutional
- Assess volume status (hypo/eu/hypervolemic)
- Urine Na⁺ cut-off: 20 mEq/L (renal vs. extrarenal)
Rate of Correction - "10/24 Rule"
- Maximum 10 mEq/L in first 24 hours for BOTH hypo and hypernatremia
- Severe symptomatic hyponatremia: initial rapid bolus 100 mL 3% saline to raise by 2-3 mEq/L, then slow
3% Saline Formula:
- 1 mEq/L rise in Na⁺ per 1 mL/kg of 3% saline (approximately)
SIADH vs. Cerebral Salt Wasting (CSW):
| Feature | SIADH | CSW |
|---|---|---|
| Volume status | Euvolemic | Hypovolemic |
| TBNa⁺ | Normal | Decreased |
| Treatment | Fluid restriction | Na⁺ + fluid replacement |
Perioperative Considerations Summary:
- Preop hyponatremia (even mild) → increased 30-day mortality; postpone elective surgery if moderate-severe
- Postop hyponatremia → premenopausal women and children most vulnerable; prevent with isotonic fluids
- TURP syndrome → treat like acute symptomatic hyponatremia
- Hypernatremia in ICU → check for DI, especially post-pituitary surgery or TBI
Sources: Miller's Anesthesia, 2-Volume Set, 10e (Chapter 43 - Fluid and Electrolyte Disorders); Rosen's Emergency Medicine, 10e (Chapter 114 - Sodium Disorders)
This is a shared conversation. Sign in to Orris to start your own chat.