I now have all the material needed. Let me write the complete learning note:
COMPLETE LEARNING NOTE
DRUG TREATMENT OF ALZHEIMER'S DISEASE
From Zero to MBBS Examination Mastery
SECTION 1: BIG PICTURE OVERVIEW
What Problem Do These Drugs Solve?
Imagine your brain as a giant library. Every room in the library is a memory, a skill, a personality. In Alzheimer's disease (AD), an invisible vandal quietly destroys each room, one by one. First the most recent rooms go - the things you learned yesterday. Then older rooms go. Eventually the vandal destroys the rooms that tell you who you are, how to speak, how to swallow, how to breathe.
Alzheimer's disease is the most common cause of dementia. It is a progressive, irreversible neurodegenerative disease. "Neurodegenerative" means neurons (brain cells) are slowly dying and not coming back. "Dementia" means a decline in memory and thinking severe enough to interfere with daily life.
The scale of the problem:
- About 3% of people aged 65-74 have it
- About 19% of people aged 75-84 have it
- About 47% of people over 84 have it
- It costs the US healthcare system $150-215 billion per year
What the drugs are trying to do:
There are two types of goals:
-
Symptomatic treatment - slow down the worsening, make the patient function a little better. These drugs do NOT cure the disease or stop it. They are like putting a better lock on the door while the vandal is still inside.
-
Disease-modifying treatment - actually target the underlying cause (the amyloid plaques) and try to slow or halt the actual destruction. This is newer and more exciting but only works in early stages.
The key neurotransmitters being targeted:
- Acetylcholine (ACh) - the "learning and memory" chemical that is being lost
- Glutamate - the "excitement" chemical that, when overactive, kills neurons
SECTION 2: BUILD THE FOUNDATION
Step 1 - Normal Brain Function (What Should Be Happening)
The Cholinergic System - Your Brain's Memory Network
Think of the brain as having many different "phone lines." The cholinergic phone line uses a chemical called acetylcholine (ACh) as its signal.
Acetylcholine (ACh):
- Made by neurons in the brain (especially in an area called the nucleus basalis of Meynert)
- Released into the synapse (the tiny gap between two neurons)
- Travels across the gap and binds to receptors on the next neuron
- Triggers that neuron to fire
- Then it gets broken down by an enzyme called acetylcholinesterase (AChE) so the signal stops
This system is critical for:
- Forming new memories
- Learning
- Attention and concentration
The normal acetylcholine cycle:
Neuron fires
↓
ACh released into synapse
↓
ACh binds to receptors on next neuron → signal transmitted
↓
AChE breaks down ACh → signal ends
↓
Choline is recycled back into neuron → more ACh made
The Glutamate System - Your Brain's Accelerator
Glutamate is the main excitatory neurotransmitter in the brain. Think of it as the accelerator pedal in a car. In normal amounts, it helps neurons fire and helps you learn and remember things. It does this by binding to NMDA receptors (N-methyl-D-aspartate receptors) on neurons, opening calcium channels, and allowing calcium to flow in - this triggers the neuron to fire and creates memories.
Under normal resting conditions, the NMDA channel is blocked by a magnesium ion (Mg²+). This Mg²+ block is like a safety plug - it prevents random, unwanted activation. The channel only opens properly when:
- Glutamate binds to the receptor, AND
- The neuron is already slightly activated (depolarized)
Step 2 - What Goes Wrong in Alzheimer's Disease
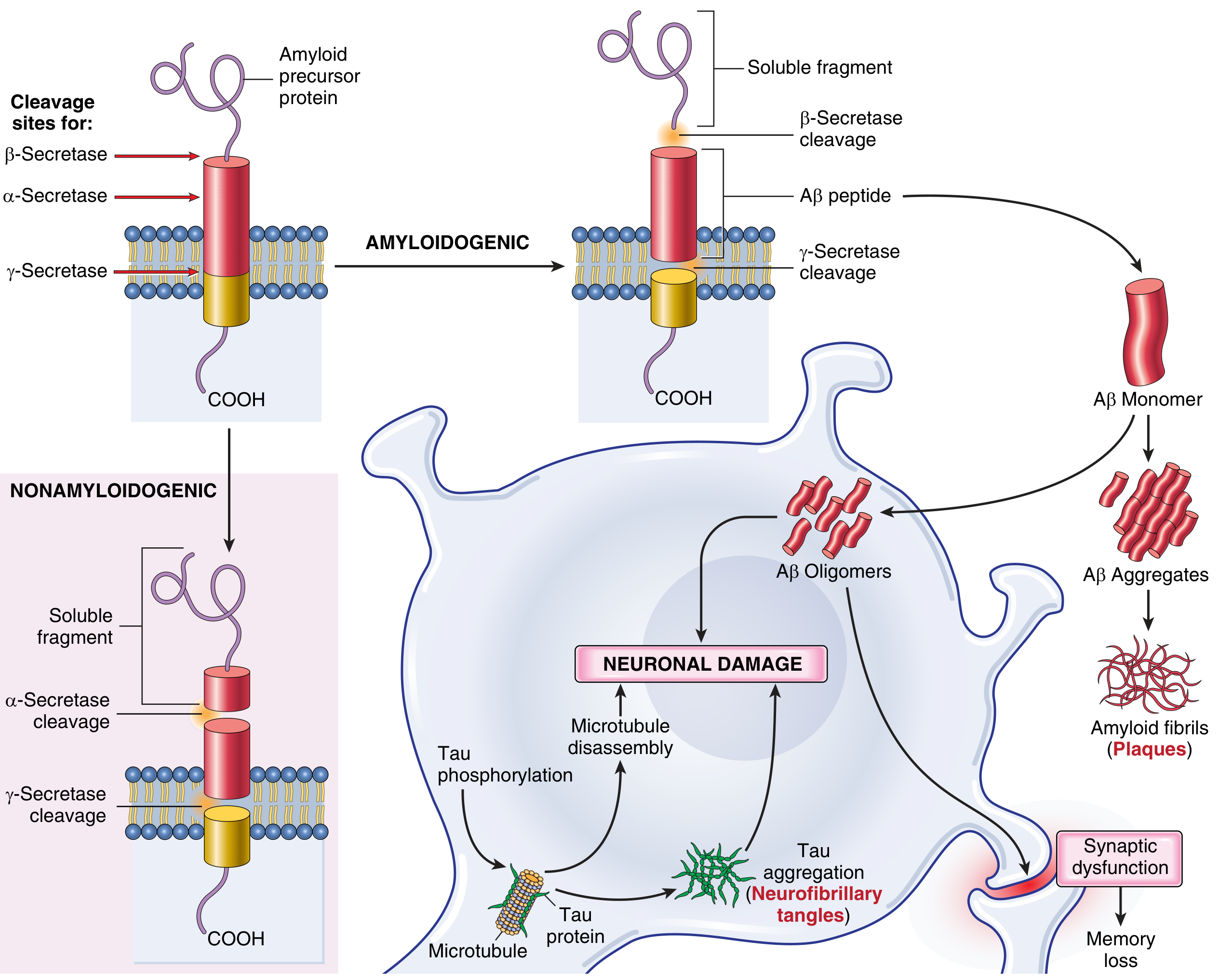
The Two Main Criminals: Amyloid Plaques and Tau Tangles
Pathogenesis of Alzheimer's Disease: Amyloid precursor protein (APP) cleavage by α-secretase produces harmless fragments; β+γ-secretase cleavage produces toxic Aβ peptides that form oligomers and plaques, while tau tangles form inside neurons. Both lead to neuronal damage and memory loss. (Robbins & Kumar Basic Pathology)
Criminal 1: Amyloid Beta (Aβ) Plaques
There is a protein embedded in neuron membranes called Amyloid Precursor Protein (APP). APP is a normal protein - everyone has it. The problem is how it gets cut up (processed).
APP can be cut in two ways:
The safe pathway (non-amyloidogenic):
APP
↓ cut by α-secretase (in the middle)
Harmless soluble fragment → excreted safely
The dangerous pathway (amyloidogenic):
APP
↓ cut by β-secretase (BACE)
↓ then cut again by γ-secretase
Aβ42 peptide released (a small, sticky protein fragment)
↓
Aβ42 monomers stick together → oligomers (clumps of 2-10)
↓
Oligomers are TOXIC to synapses - they directly damage memory formation
↓
More oligomers stick together → amyloid fibrils
↓
Fibrils accumulate → AMYLOID PLAQUES (extracellular deposits in brain tissue)
The Aβ42 form is more dangerous than Aβ40 because it sticks together more easily. Think of Aβ42 as a very sticky piece of chewing gum - even a small amount will stick to everything and build up into a large mess.
Why does this happen in some people?
- Gene mutations in APP (chromosome 21) - more APP = more Aβ
- Gene mutations in Presenilin-1 (chromosome 14) and Presenilin-2 (chromosome 1) - these are parts of the γ-secretase enzyme; mutations change the ratio of Aβ42 to Aβ40, making more of the sticky 42 form
- ApoE ε4 allele (chromosome 19) - impairs clearance of Aβ from the brain
- Trisomy 21 (Down syndrome) - extra copy of chromosome 21 = extra APP gene = more Aβ
Criminal 2: Tau (Neurofibrillary Tangles)
Inside neurons, there are tiny "railway tracks" called microtubules that transport nutrients and molecules from the cell body to the tip of the axon. The tau protein is like the railway sleepers - it stabilizes and maintains these tracks.
In AD:
Aβ oligomers activate abnormal kinases (enzymes)
↓
These kinases add too many phosphate groups to tau protein
↓
Hyperphosphorylated tau detaches from microtubules
↓
Microtubules collapse → transport inside neuron fails
↓
Tau clumps together → neurofibrillary tangles (inside neurons)
↓
Neuron eventually dies
↓
Tangles persist extracellularly even after neuron death (ghost tangles)
Important fact for exams: The NUMBER of neurofibrillary tangles correlates better with the DEGREE OF DEMENTIA than the number of plaques. The Braak and Braak staging system grades AD by the spread of tangles from the entorhinal cortex outward.
The Cascade of Consequences
Aβ plaques + tau tangles
↓
Synapse dysfunction (memory formation fails)
↓
Neuroinflammation (microglia and astrocytes become activated)
↓
Oxidative stress (free radical damage)
↓
Progressive neuron death
↓
Loss of CHOLINERGIC neurons (especially from nucleus basalis of Meynert)
↓
↓↓ Acetylcholine levels in the brain
↓
Memory loss, confusion, language problems
↓
Loss of GLUTAMATERGIC regulation
↓
Excess glutamate → overactivated NMDA receptors → excitotoxicity
↓
More neuron death
↓
Eventually: complete vegetative state
Excitotoxicity - The Runaway Accelerator
"Excitotoxicity" - let's define this. "Excito" = excitement (neuronal firing). "Toxic" = harmful. When NMDA receptors are chronically overactivated, too much Ca²+ floods into neurons continuously.
This excess calcium:
- Activates destructive enzymes (proteases, lipases, nucleases)
- Triggers free radical production
- Activates apoptosis (programmed cell death)
- Destroys the neuron from the inside
Think of it like this: a normal engine runs great at normal speed. But if you jam the accelerator to the floor and it never comes back, the engine eventually burns itself out. Excitotoxicity is neurons burning themselves out because glutamate keeps their "accelerator" stuck to the floor.
What Can Drugs Target?
TARGET 1: Low ACh levels → AChE inhibitors (don't destroy what's left)
TARGET 2: Excitotoxic glutamate → NMDA antagonists (block the runaway accelerator)
TARGET 3: Amyloid plaques → Anti-amyloid monoclonal antibodies (remove the plaques)
TARGET 4 (future): Tau tangles → Anti-tau therapies (in development)
TARGET 5 (future): β-secretase → BACE inhibitors (reduce Aβ production)
SECTION 3: DRUG CLASS FRAMEWORK
CLASS 1: ACETYLCHOLINESTERASE (AChE) INHIBITORS
Definition
AChE inhibitors are drugs that block the enzyme acetylcholinesterase. Because this enzyme normally breaks down ACh in the synapse, blocking it means ACh stays in the synapse longer, stimulating receptors for longer, partially compensating for the loss of cholinergic neurons.
They do NOT stop neuron death. They just make the most of what neurons remain.
Why It Works - Step by Step
Normal: ACh released → binds receptor → AChE destroys ACh → signal ends
In AD: ↓↓ ACh (fewer neurons making it) → weak signals → poor memory
With AChEI: ↓↓ ACh (fewer neurons) BUT AChE is blocked → ACh stays longer
→ longer/stronger signal → better memory function
The Three Approved AChE Inhibitors
| Feature | Donepezil | Rivastigmine | Galantamine |
|---|
| Brand name | Aricept | Exelon | Razadyne |
| Enzyme blocked | AChE only | AChE + BuChE | AChE only |
| Extra action | None | None | Also allosteric modulator of nicotinic ACh receptors |
| Route | Oral (tablet) | Oral OR transdermal patch | Oral (tablet/liquid/extended-release) |
| Dosing frequency | Once daily | Twice daily (oral); once daily (patch) | Twice daily or once daily (ER) |
| Stage of AD | All stages (mild/moderate/severe) | All stages; only agent approved for Parkinson's disease dementia | Mild to moderate |
| CYP450 metabolism | Yes (2D6, 3A4) | No (hydrolyzed by AChE itself) | Yes (2D6, 3A4) |
| Drug interactions | Higher risk | Lower risk (no CYP450) | Higher risk |
Note on BuChE (butyrylcholinesterase): This is a second type of cholinesterase enzyme, less important than AChE but still breaks down ACh. Rivastigmine blocks both AChE and BuChE, making it a "dual inhibitor." In AD brains, as disease progresses, AChE activity falls but BuChE rises - theoretically making rivastigmine more useful in moderate-severe disease.
Note on galantamine's nicotinic receptor action: By allosterically modulating nicotinic ACh receptors, galantamine makes these receptors more sensitive to whatever ACh is present. Think of it as fine-tuning a radio to pick up a weak signal better.
Mechanism of Action - Detailed
Mechanism of donepezil (prototype):
1. Donepezil is a piperidine-based reversible inhibitor
2. It binds to the active site of AChE (non-covalent, reversible binding)
3. AChE cannot break down ACh while donepezil is bound
4. ACh accumulates in the synapse
5. ACh binds to muscarinic and nicotinic receptors more extensively
6. Cholinergic neurotransmission is enhanced
7. Cognitive function modestly improves
Selectivity: These drugs have some selectivity for brain AChE over peripheral AChE (though not perfect). This is why they don't cause the same intensity of peripheral cholinergic side effects as neostigmine or pyridostigmine (which are peripheral AChE inhibitors used in myasthenia gravis).
Key distinction from peripheral AChE inhibitors:
| Feature | Central AChEI (AD drugs) | Peripheral AChEI (MG drugs) |
|---|
| Drugs | Donepezil, rivastigmine, galantamine | Neostigmine, pyridostigmine |
| Cross BBB? | YES | NO |
| Use | Alzheimer's, Parkinson's dementia | Myasthenia gravis, post-op bowel atony |
| Selectivity | CNS > peripheral | Peripheral only |
Clinical Effectiveness
- On average, a patient on an AChE inhibitor maintains their MMSE (Mini Mental State Examination) score for close to one year, while a placebo-treated patient declines 2-3 MMSE points over the same period
- They do NOT stop the disease or reverse damage
- They are approved for mild, moderate, and (donepezil/rivastigmine patch) severe AD
- They do NOT work for MCI (Mild Cognitive Impairment) - clinical trials showed no benefit
Adverse Effects - Each Explained by Mechanism
Since AChE inhibitors increase ACh everywhere ACh is active, their side effects are all cholinergic ("DUMBELS" effects, especially GI and cardiac):
| Adverse Effect | Mechanism | Explanation |
|---|
| Nausea, vomiting | ACh stimulates M3 receptors in gut → ↑ gut motility and secretion | The gut has lots of ACh receptors. More ACh = more gut activity |
| Diarrhea | Same mechanism - ↑ intestinal peristalsis | GI smooth muscle is stimulated |
| Anorexia (loss of appetite) | Central and peripheral mechanisms | Partly due to nausea, partly central |
| Bradycardia | ACh stimulates M2 receptors in the SA node → slows heart rate | Vagotonic effect on the heart - the single most important cardiac risk |
| Syncope (fainting) | Secondary to bradycardia and hypotension | Clinically significant - can cause falls and fractures in elderly |
| Muscle cramps | ↑ ACh at neuromuscular junction → excess muscle stimulation | Peripheral nicotinic receptor activation |
| Insomnia / vivid dreams | Central cholinergic activation during sleep | REM sleep enhancement - ACh is active during REM |
| Urinary incontinence | ACh stimulates M3 receptors in bladder → ↑ detrusor contraction | Increases urge to urinate |
The most dangerous and clinically important adverse effect is BRADYCARDIA. This is especially dangerous in patients with:
- Sick sinus syndrome
- Sinoatrial block
- Atrioventricular block
- Patients also on digoxin or beta-blockers (additive bradycardia)
A critical clinical trap: When patients develop GI side effects (nausea, diarrhea), doctors sometimes prescribe anticholinergic drugs to counteract them (e.g., antispasmodics). This is counterproductive - the anticholinergic drug crosses the BBB and blocks the very ACh that the AChE inhibitor is trying to preserve. The treatment for the side effect undoes the treatment for the disease.
Contraindications
- Active peptic ulcer disease (↑ gastric acid secretion)
- Sick sinus syndrome or AV block (without a pacemaker)
- Severe hepatic impairment (donepezil and galantamine)
- Concurrent use with other cholinomimetics
- Known hypersensitivity to carbamate compounds (rivastigmine)
Drug Interactions
| Drug | Interaction | Mechanism |
|---|
| Digoxin | Additive bradycardia | Both slow heart rate |
| Beta-blockers | Additive bradycardia | Both slow heart rate |
| NSAIDs | ↑ risk of GI ulcers | Both increase GI secretion / irritation |
| Anticholinergic drugs | Reduced efficacy of AChEI | Competitive antagonism at ACh receptors |
| CYP2D6/3A4 inhibitors (e.g., fluoxetine, ketoconazole) | ↑ levels of donepezil and galantamine | Reduced metabolism |
| Succinylcholine | Prolonged neuromuscular blockade (rivastigmine less so) | Additive AChE inhibition |
Tolerability Ranking (from Maudsley Prescribing Guidelines)
Best tolerated first (fewest withdrawals due to adverse effects):
- Donepezil (best tolerated overall)
- Galantamine
- Rivastigmine patch
- Rivastigmine oral (most likely to cause nausea/vomiting)
CLASS 2: NMDA RECEPTOR ANTAGONIST - MEMANTINE
Definition
Memantine is the only NMDA (N-methyl-D-aspartate) receptor antagonist approved for Alzheimer's disease. It is indicated for moderate to severe AD.
Why It Was Developed - The Problem It Solves
In AD, as neurons degenerate, glutamate regulation goes wrong. Glutamate "leaks" out of damaged neurons tonically (continuously, at low levels). This chronic low-level glutamate keeps NMDA receptors slightly open at all times. Remember, normal NMDA channel opening requires proper physiological activation (for memory formation). This chronic, low-level, non-physiological activation means:
- Calcium continuously trickles into neurons
- Neurons are always slightly stressed
- The normal signal-to-noise ratio for memory formation is destroyed
- Eventually the excess calcium triggers apoptosis
This is excitotoxicity - not a dramatic sudden flood, but a slow drowning.
The Magnesium Analogy and How Memantine Works
Under normal resting conditions, Mg²+ ions sit inside the NMDA channel like a cork in a bottle, blocking it. When a neuron fires properly (strong physiological signal), the depolarization pushes Mg²+ out of the channel, the channel opens properly, Ca²+ flows in, and a memory is formed. After the firing stops, the Mg²+ plugs the channel again.
In AD, the tonic leaking of glutamate creates a weak, constant partial depolarization. This is just enough to dislodge the Mg²+ cork, but not enough to trigger proper memory-forming activity. The channel sits in a "half open" state, constantly leaking Ca²+.
Memantine acts like a better cork:
Memantine enters the NMDA channel during tonic (pathological) low-level opening
↓
Blocks the channel (like Mg²+, but better - stays in place)
↓
Tonic Ca²+ influx STOPS → less excitotoxicity → neurons protected
↓
BUT: When a strong physiological signal comes (proper memory formation)
↓
The strong depolarization is enough to push memantine out of the channel
↓
Proper Ca²+ influx occurs → memory formation proceeds normally
↓
After firing, memantine re-enters the channel → blocks again
This is why memantine is called an "uncompetitive, low-affinity, open-channel blocker" or a "voltage-dependent open-channel blocker."
- "Uncompetitive" = it doesn't compete with glutamate for the same binding site; it enters the channel pore
- "Low affinity" = it dissociates relatively easily from the channel when strong signals come
- "Open-channel blocker" = it only enters and blocks the channel when it is open
- "Voltage-dependent" = the strong voltage of physiological activation pushes it out
Comparison of Memantine vs Magnesium
| Feature | Magnesium (Mg²+) | Memantine |
|---|
| Blocks resting NMDA channel? | Yes | Yes |
| Displaced by physiological signals? | Yes | Yes |
| Displaced by tonic low-level pathological activation? | YES (this is the problem in AD) | NO (stays in place - this is the benefit) |
| Result in AD | Channel stays half-open → excitotoxicity | Channel properly blocked → neuroprotection |
Clinical Use of Memantine
- FDA approved for moderate to severe AD (NOT mild AD)
- Often used in combination with an AChE inhibitor for moderate-severe AD
- The combination of donepezil + memantine is a very common regimen
- Has modest effects: slows cognitive deterioration and decreases caregiver burden
- Not effective for MCI (Mild Cognitive Impairment)
Adverse Effects of Memantine
Memantine is generally better tolerated than AChE inhibitors. Its adverse effects are mild:
| Adverse Effect | Mechanism |
|---|
| Dizziness | CNS effect on glutamatergic pathways |
| Headache | CNS effect |
| Confusion / agitation | Often indistinguishable from AD symptoms themselves |
| Constipation | Reduced gut motility (opposite of AChEIs) |
| Somnolence | CNS sedation |
Notable: Memantine does NOT cause bradycardia or GI upset - in fact its GI effects (constipation) are the opposite of AChE inhibitors.
Pharmacokinetics of Memantine
- Oral bioavailability: ~100% (excellent)
- Not significantly metabolized by CYP450 (unlike donepezil/galantamine)
- Eliminated renally: 80% unchanged in urine
- Dose reduction required in renal impairment - important exam fact
- Half-life: 60-80 hours (once or twice daily dosing)
CLASS 3: ANTI-AMYLOID MONOCLONAL ANTIBODIES (Disease-Modifying Therapies)
The Big Idea
Instead of compensating for lost neurotransmitters (like AChE inhibitors and memantine do), anti-amyloid antibodies try to directly remove the cause - the amyloid plaques. They represent the first true disease-modifying therapies for AD.
The Three Key Agents
| Drug | Target | FDA Status | Route | Frequency |
|---|
| Lecanemab (Leqembi) | Aβ protofibrils (soluble oligomers) | Fully FDA approved (2023) | IV infusion | Every 2 weeks |
| Donanemab | Pyroglutamate-modified Aβ in plaques | Fully FDA approved (2024) | IV infusion | Monthly |
| Aducanumab (Aduhelm) | Aβ aggregates | Accelerated approval 2021 (withdrawn from market) | IV infusion | Every 4 weeks |
How They Work
Monoclonal antibody administered IV
↓
Antibody binds specifically to Aβ oligomers/protofibrils/plaques
↓
Immune system (microglia) recognizes the antibody-coated amyloid
↓
Microglia engulf and destroy the amyloid (phagocytosis)
↓
Amyloid plaque burden reduced (measurable on amyloid PET scans)
↓
Fewer toxic Aβ oligomers → less tau phosphorylation → slower neurodegeneration
Clinical Evidence
- Lecanemab (CLARITY-AD trial): 27% slowing of cognitive decline vs. placebo over 18 months - first convincing clinical benefit of an anti-amyloid antibody
- Donanemab (TRAILBLAZER-ALZ 2 trial): ~35% slowing of decline in patients with low-to-moderate tau burden
- Aducanumab: Conflicting data in two Phase 3 trials - clinical benefit was ambiguous; drug was ultimately withdrawn from clinical use despite FDA approval
Key restriction: These drugs are ONLY approved for early-stage AD - patients with MCI or mild dementia who have BIOMARKER CONFIRMATION of amyloid pathology (by amyloid PET scan or CSF analysis showing low Aβ42 / high tau). They are NOT for moderate or severe AD.
The Major Adverse Effect: ARIA
ARIA = Amyloid-Related Imaging Abnormalities
This is the class-defining side effect. When antibodies cause rapid clearance of amyloid from blood vessel walls (where amyloid also deposits), it can cause:
- ARIA-E (Edema): Swelling of brain tissue around the cleared plaques - seen as white areas on FLAIR MRI
- ARIA-H (Hemorrhage): Small bleeds (microhemorrhages or superficial siderosis) in the brain - seen as dark spots on T2* or SWI MRI
ARIA is usually asymptomatic and self-limiting, but can occasionally cause:
- Headache
- Confusion
- Visual disturbances
- Seizures (severe cases)
ApoE ε4 carriers have a higher risk of ARIA - this is important for patient selection.
Management of ARIA: Regular MRI monitoring; dose reduction or temporary suspension if significant ARIA develops; in symptomatic/severe ARIA, treatment must stop.
Why These Drugs are Revolutionary (But Not Perfect)
They target the cause, not the symptom. But:
- They only slow progression - they do NOT reverse existing damage
- They need to be started VERY early
- Monitoring with repeated amyloid PET and MRI is expensive and burdensome
- ARIA risk requires careful patient selection
- Not all patients respond equally
- Cost is very high
DRUGS THAT DO NOT WORK (Important for Exams)
Many drugs have been tested and found to be ineffective or harmful:
| Drug | What Was Tried | Result |
|---|
| Vitamin E | Antioxidant - reduce oxidative stress | NO benefit proven |
| NSAIDs (e.g., ibuprofen) | Anti-inflammatory - reduce neuroinflammation | NO clinical benefit in trials |
| Estrogens/HRT | Neuroprotective (theoretical) | NO benefit; possible increased risk |
| Ginkgo biloba | Vascular/antioxidant effects | NOT proven efficacious |
| Selegiline (MAO-B inhibitor) | Reduce oxidative stress | NO clear benefit |
| Statins | ↓ Aβ production (theoretical) | NO proven benefit |
| Cerebral vasodilators | Improve blood flow | NOT effective |
| Piracetam derivatives | Cognitive enhancement | NOT proven |
| Solanezumab / bapineuzumab | Anti-amyloid antibodies | FAILED - no clinical benefit |
SUMMARY TABLE: ALL APPROVED DRUGS AT A GLANCE
| Drug | Class | Stage of AD | Mechanism | Key Feature |
|---|
| Donepezil | AChEI | All stages | Blocks AChE reversibly | Once daily; most prescribed |
| Rivastigmine | AChEI (dual) | All stages + Parkinson's dementia | Blocks AChE + BuChE | Patch available; no CYP450 |
| Galantamine | AChEI | Mild-moderate | Blocks AChE + nicotinic modulator | Dual mechanism |
| Memantine | NMDA antagonist | Moderate-severe | Blocks overactive NMDA receptors | Combines with AChEI |
| Lecanemab | Anti-amyloid mAb | MCI/mild only | Targets Aβ protofibrils | First FDA-approved DMT |
| Donanemab | Anti-amyloid mAb | MCI/mild only | Targets pyroglutamate-Aβ | Monthly IV dosing |
| Donepezil + Memantine (Namzaric) | Combination | Moderate-severe | Dual mechanism | Fixed-dose combination tablet |
SECTION 4: TEACH USING ANALOGIES
Analogy 1: AChE Inhibitors - The Leaking Dam
Think of the cholinergic synapse as a pool of water (ACh). Normally, water flows in (released by neuron) and drains out (destroyed by AChE). In AD, the pipes bringing water in are damaged (fewer neurons), so the pool is always low. You cannot fix the broken pipes - the neurons are dead. But what you CAN do is partially block the drain. AChE inhibitors are like putting a stopper in the drain. The amount of water coming in is the same (or less), but by blocking the drain, the pool stays fuller longer. The pool isn't perfect, but it works better than before. The problem is that blocking the drain affects ALL the drains in your house - including in the gut (diarrhea), in the heart (bradycardia), and in the bladder (urgency).
Analogy 2: Memantine - The Smart Traffic Light
Imagine NMDA receptors as traffic lights at an intersection. Under normal conditions, the lights work perfectly: they turn green when there is a proper reason (cars waiting = physiological signals), allow traffic (Ca²+) through, then turn red again. In AD, a traffic system failure causes the lights to stick on a permanent low-level "amber" - not fully green, but never fully red either. Cars (Ca²+) trickle through constantly. The intersection gets congested and damaged over time.
Memantine is like installing a smart override system. It holds the light firmly on red during the abnormal amber (tonic glutamate leak). But when a real emergency vehicle comes (strong physiological memory-formation signal), the override steps aside and allows proper green light. After the emergency, the override kicks back in. The intersection stays functional for important signals but is protected from the constant damaging trickle.
Analogy 3: Anti-Amyloid Antibodies - Garbage Collectors for Protein Waste
In AD, amyloid plaques are like a mountain of rubbish that has built up in the city (brain) because the sanitation workers (natural clearance mechanisms) couldn't keep up. The rubbish blocks roads, poisons the environment, and causes the city to decay.
Anti-amyloid antibodies are like hiring an elite specialized garbage collection team. You show them exactly what rubbish to collect (by attaching a specific "tag" - the antibody binds to Aβ). The local immune cells (microglia) see the tagged rubbish and cart it away. The city becomes cleaner. But: the rubbish has already damaged some roads (neurons are already dead), so clearing the rubbish won't fix what was already destroyed. And occasionally, when collecting the rubbish from near water pipes (blood vessels), some pipes get nicked - causing small bleeds or swelling (ARIA).
Analogy 4: The AD Pathology Story for a 9-Year-Old
Imagine neurons as builders who work in a town (your brain), building and maintaining the roads (memories). Each builder uses a special cement called acetylcholine to communicate with others and also has little train tracks inside called microtubules to carry supplies.
One day, a sticky gum (Aβ42) starts falling from the sky. The builders can't clean it up fast enough. It sticks to everything. Some builders slip on it and get hurt. Their train tracks collapse (tau tangles). Builders start dying.
The remaining builders try harder but they run out of cement (ACh). The AChE inhibitor drugs are like making the cement dry slower, so it can be used twice. Memantine is like teaching builders to wear earplugs against the noise pollution (excess glutamate) that was also confusing them. The new antibody drugs are like sending in a cleaning crew to finally remove the sticky gum.
SECTION 5: STEP-BY-STEP CLINICAL REASONING
Clinical Scenario: An 82-year-old woman is brought by her daughter, who reports her mother has been forgetting names and getting lost in familiar places for 2 years. She now repeats herself in conversation and cannot manage her finances independently. MMSE = 19/30.
Step 1: What is the diagnosis?
- MMSE of 19/30 = moderate cognitive impairment (mild = 20-24, moderate = 10-19)
- Progressive memory loss + functional impairment + age = probable Alzheimer's disease
- Confirm: rule out reversible causes (thyroid disease, B12 deficiency, depression, NPH, SDH)
- Brain imaging (CT/MRI) to exclude structural lesions
Step 2: What stage of AD is this?
- MMSE 19 = mild to moderate AD
- Still functioning to some degree but needs supervision
Step 3: Which drugs are appropriate at this stage?
- AChE inhibitors: appropriate (all three are approved for mild-moderate AD)
- Memantine: borderline - primarily indicated for moderate-severe; can consider adding
- Anti-amyloid antibodies: NOT appropriate - too late in disease; these are for MCI/mild AD with biomarker confirmation
Step 4: Which AChE inhibitor to choose?
Ask the following questions:
- Can she use a patch? → Consider rivastigmine patch if she has swallowing difficulties or adherence issues
- Does she have Parkinson's? → Rivastigmine is the only AChE inhibitor approved for Parkinson's dementia
- Any cardiac history (bradycardia, heart block)? → Use with caution; avoid if significant conduction abnormality
- Liver disease? → Rivastigmine preferred (no CYP450 interaction)
- Simplicity of dosing? → Donepezil once daily is easiest
Most commonly chosen first-line: Donepezil 5 mg once daily (titrate to 10 mg after 4-6 weeks).
Step 5: What to monitor after starting donepezil?
- GI side effects (nausea, diarrhea) - especially in first 4-6 weeks
- Heart rate (bradycardia risk)
- Sleep disturbances (take in the morning, not at night, if causing vivid dreams)
- Cognitive function (MMSE every 6 months)
- Falls (syncope/bradycardia → falls → fractures in elderly)
Step 6: When to add memantine?
- When patient progresses to moderate-severe AD (MMSE falls below 15-18)
- Add memantine 5 mg daily, titrate over 4 weeks to target dose of 10 mg twice daily
- Combination is more effective than either drug alone in moderate-severe disease
Step 7: What to tell the family?
- These drugs slow decline, they do NOT cure or reverse the disease
- Average benefit is 6-12 months of stabilization/slower decline
- Discuss long-term care planning
- Treat behavioral symptoms (depression, agitation, psychosis) if they emerge
- Screen for caregiver burnout
Clinical Reasoning: Drug Selection for Behavioral Symptoms in AD
| Symptom | Drug of Choice | Notes |
|---|
| Depression | SSRI (sertraline, citalopram) | Avoid TCAs - anticholinergic |
| Agitation | Low-dose quetiapine or risperidone | Use with caution - mortality risk in elderly with dementia |
| Psychosis (delusions, hallucinations) | Atypical antipsychotics | Black box warning in elderly |
| Sleep disturbance | Melatonin | Avoid benzodiazepines - worsen cognition |
| Anxiety | SSRI | Avoid benzodiazepines |
Critical drug to AVOID in AD patients: Anticholinergic drugs of any kind - they worsen cognition dramatically because AD patients are "exquisitely sensitive" to anticholinergic effects due to their already-depleted ACh.
SECTION 6: MEMORY TOOLS
Mnemonic 1: Approved Drugs - "Don't Give Me Regret" (D-G-M-R)
Donepezil
Galantamine
Memantine
Rivastigmine
Mnemonic 2: AChE Inhibitor Side Effects - "DUMB"
D - Diarrhea
U - Urinary incontinence
M - Muscle cramps / myalgia
B - Bradycardia (the big dangerous one)
Add: Nausea, Anorexia, Vivid dreams, insomnia
Mnemonic 3: Memantine's Adverse Effects - "DCHS"
D - Dizziness
C - Confusion (hard to distinguish from AD itself)
H - Headache
S - Somnolence + constipation
Mnemonic 4: Stages and Drug Use
"Mild = Monotherapy" → AChE inhibitor alone
"Moderate-Severe = Memantine Starts" → Add memantine
Mnemonic 5: Rivastigmine is SPECIAL because:
S - Skin patch available
P - Parkinson's dementia (only AChEI approved)
E - enzyme it blocks: both AchE and ButyrylcholinEsterase (dual)
C - CYP450: NOT metabolized by CYP450
I - Independent of CYP450 drug interactions
A - All stages of AD approved
L - Less systemic side effects with patch
Mnemonic 6: Galantamine is "DUAL ACTION"
Blocks AChE + Allosteric modulator of Nicotinic receptors
Remember: GalanTAMINe → "TAMING" two targets
Memory Story: The Alzheimer's Pharmacology Courtroom
Imagine a courtroom fighting the "Case of the Lost Memory":
-
Three lawyers (AChE inhibitors) - Donepezil, Galantamine, and Rivastigmine - try to preserve evidence (ACh) by preventing its destruction. The paralegal Rivastigmine also blocks a second destruction pathway (BuChE) and even comes to court via a skin patch.
-
The security guard (Memantine) stands at the back door (NMDA channel), stopping dangerous calcium floods from entering. He's smart enough to step aside when VIP signals (real memories) need to enter, but blocks the riffraff (tonic glutamate).
-
The new elite cleaners (Lecanemab, Donanemab) just arrived to clean up the amyloid mess, but they can only work when the mess is small (early disease) and they occasionally bump into pipes (ARIA).
Comparison Table: AChE Inhibitors Side-by-Side
| Feature | Donepezil | Rivastigmine | Galantamine |
|---|
| Reversible inhibitor? | Yes | Yes (pseudo-irreversible) | Yes |
| Selectivity | AChE > BuChE | AChE = BuChE | AChE > BuChE |
| Additional mechanism | None | None | Nicotinic allosteric potentiation |
| CYP450 metabolism | Yes (2D6, 3A4) | No | Yes (2D6, 3A4) |
| Patch formulation | No | Yes | No |
| Parkinson's dementia approved | No | YES | No |
| AD stages approved | All | All | Mild-moderate |
| Most common side effect | GI symptoms | GI symptoms | GI symptoms |
| Most dangerous side effect | Bradycardia | Bradycardia | Bradycardia (mortality warning in MCI) |
Rapid Review Box: Stage-Based Treatment
+---------------------------+----------------------------+------------------------------+
| MILD AD | MODERATE AD | SEVERE AD |
| (MMSE 20-26) | (MMSE 10-19) | (MMSE <10) |
+---------------------------+----------------------------+------------------------------+
| Start AChE inhibitor | Continue AChE inhibitor | Continue AChE inhibitor |
| (Donepezil preferred) | ADD Memantine | + Memantine |
| | | |
| Anti-amyloid mAb if: | Anti-amyloid mAb: usually | Anti-amyloid mAb: |
| - biomarker confirmed | NOT appropriate (too late) | NOT appropriate |
| - early stage confirmed | | |
+---------------------------+----------------------------+------------------------------+
SECTION 7: EXAMINER'S CORNER
Most Tested Facts in MBBS Examinations
- Donepezil is the most commonly used first-line drug for AD - once daily dosing
- Memantine is used for moderate-to-severe AD - NMDA receptor antagonist
- The mechanism of AChE inhibitors - block acetylcholinesterase → ↑ ACh at synapse
- Rivastigmine is the only drug approved for Parkinson's dementia AND has a patch formulation
- Rivastigmine is the only AChE inhibitor that does NOT use CYP450 for metabolism
- The most dangerous adverse effect of AChE inhibitors is BRADYCARDIA
- Memantine's mechanism: uncompetitive, voltage-dependent, open-channel NMDA blocker
- Anti-amyloid antibodies cause ARIA (brain edema and microhemorrhages)
- Galantamine has a mortality warning in MCI patients (cardiovascular deaths in trials)
- Anticholinergic drugs worsen AD - treating AChEI side effects with anticholinergics is counterproductive
Most Likely Essay Questions
- "Write a pharmacological note on the drug treatment of Alzheimer's disease."
- "Discuss the role of acetylcholinesterase inhibitors in the management of Alzheimer's disease, including their mechanisms, clinical uses, and adverse effects."
- "Describe the pathophysiology of Alzheimer's disease and explain how current pharmacological agents target these mechanisms."
- "Compare and contrast donepezil and memantine in the treatment of Alzheimer's disease."
Most Likely Short Notes
- Donepezil
- Memantine - mechanism and clinical use
- Disease-modifying therapy in Alzheimer's disease
- Adverse effects of AChE inhibitors
- Rivastigmine - why is it special?
Most Likely Viva Questions
Q: What is the mechanism of action of donepezil?
A: Donepezil is a reversible, selective inhibitor of acetylcholinesterase (AChE) in the CNS. It prevents the enzymatic breakdown of acetylcholine in the synaptic cleft, thereby increasing the concentration and duration of ACh available to bind to muscarinic and nicotinic receptors. This partially compensates for the progressive loss of cholinergic neurons in the nucleus basalis of Meynert that characterizes Alzheimer's disease.
Q: Why is memantine used only in moderate-to-severe AD and not mild AD?
A: Clinical trials have shown that memantine is efficacious only in patients with moderate-to-severe AD (MMSE < 15-20). In mild AD, there is insufficient tonic NMDA receptor activation to make blocking these receptors clinically meaningful. Furthermore, clinical trials in mild AD and MCI did not demonstrate significant benefit.
Q: Which AChE inhibitor is approved for Parkinson's disease dementia, and why?
A: Rivastigmine. It is the only AChE inhibitor with FDA approval for dementia associated with Parkinson's disease. This may be partly because Parkinson's disease involves cholinergic dysfunction in different brain regions compared to AD, and rivastigmine's dual blockade of both AChE and BuChE may provide an advantage.
Q: What is ARIA, and which drugs cause it?
A: ARIA (Amyloid-Related Imaging Abnormalities) is a class-specific adverse effect of anti-amyloid monoclonal antibodies (lecanemab, donanemab). It manifests as ARIA-E (edema on FLAIR MRI) or ARIA-H (microhemorrhages on T2* MRI). It occurs because rapid clearance of amyloid from vessel walls can cause local inflammatory changes. Most cases are asymptomatic, but symptomatic ARIA requires treatment discontinuation.
Q: A patient on donepezil develops severe bradycardia. What do you do?
A: Reduce the dose or discontinue the AChE inhibitor. Assess for concurrent bradycardia-inducing medications (beta-blockers, digoxin, CCBs). Arrange cardiology review. If symptomatic bradycardia persists, permanent discontinuation of the AChE inhibitor may be necessary, with possible consideration of pacemaker if the bradycardia is independent of the drug.
Most Likely MCQs
MCQ 1: Which drug is used for the treatment of moderate-to-severe Alzheimer's disease and acts by blocking NMDA receptors?
a) Donepezil
b) Rivastigmine
c) Memantine ← Correct
d) Galantamine
MCQ 2: Which of the following AChE inhibitors does NOT use the CYP450 enzyme system for its metabolism?
a) Donepezil
b) Galantamine
c) Rivastigmine ← Correct
d) All of the above
MCQ 3: The most serious cardiovascular adverse effect of AChE inhibitors in Alzheimer's disease is:
a) Hypertension
b) QT prolongation
c) Ventricular tachycardia
d) Bradycardia ← Correct
MCQ 4: Rivastigmine differs from other AChE inhibitors in AD because it:
a) Crosses the blood-brain barrier
b) Inhibits both AChE and butyrylcholinesterase ← Correct
c) Is used only in severe AD
d) Causes no GI side effects
MCQ 5: The mechanism of memantine in Alzheimer's disease is best described as:
a) Inhibiting acetylcholinesterase
b) Blocking muscarinic receptors
c) Uncompetitive, voltage-dependent NMDA receptor antagonism ← Correct
d) Inhibiting beta-secretase
MCQ 6: Which of the following is TRUE about lecanemab?
a) It inhibits acetylcholinesterase
b) It is used in severe Alzheimer's disease
c) It is a monoclonal antibody that targets Aβ protofibrils and was fully FDA-approved in 2023 ← Correct
d) It does not cause brain edema
MCQ 7: A patient with mild-moderate AD is started on a drug. The patient develops vivid dreams and insomnia. These side effects are best explained by:
a) NMDA receptor activation
b) Increased CNS acetylcholine (ACh) causing REM sleep enhancement ← Correct
c) Serotonergic effects
d) Antihistaminergic effects
Common Traps Students Fall Into
Trap 1: "Memantine is used in mild AD."
Truth: Memantine is approved for MODERATE-TO-SEVERE AD. It is NOT approved for mild AD.
Trap 2: "All AChE inhibitors are used only in mild AD."
Truth: Donepezil (all stages), rivastigmine patch (all stages) are approved for SEVERE AD too.
Trap 3: "Rivastigmine uses CYP450 metabolism."
Truth: Rivastigmine is metabolized by AChE itself (carbamylation), NOT by CYP450. This makes it safer in patients on multiple medications.
Trap 4: "Anticholinergics can be safely given to manage AChE inhibitor side effects."
Truth: Anticholinergics that cross the BBB will UNDO the cognitive benefit of the AChE inhibitor. This is a major prescribing error.
Trap 5: "Aducanumab is the current standard anti-amyloid therapy."
Truth: Aducanumab was withdrawn from clinical use due to ambiguous clinical trial results. Lecanemab and donanemab are the current approved disease-modifying therapies.
Trap 6: "AChE inhibitors work well in MCI."
Truth: Clinical trials have shown NO benefit of AChE inhibitors in MCI. They are only used for established AD dementia.
Trap 7: "The number of amyloid plaques directly determines the degree of dementia."
Truth: The NUMBER OF NEUROFIBRILLARY TANGLES correlates BETTER with degree of dementia than the number of amyloid plaques.
SECTION 9: HIGH-YIELD REVISION SHEET
ONE-PAGE REVISION SUMMARY: DRUG TREATMENT OF ALZHEIMER'S DISEASE
PATHOPHYSIOLOGY IN 5 LINES
- Aβ42 forms from APP via β+γ-secretase cleavage → aggregates → plaques + toxic oligomers
- Oligomers → tau hyperphosphorylation → neurofibrillary tangles → neuron death
- Loss of cholinergic neurons (nucleus basalis of Meynert) → ↓ACh → memory failure
- Damaged neurons release tonic glutamate → chronic NMDA activation → excitotoxicity
- Targets: ACh preservation (AChEI), NMDA blockade (memantine), amyloid clearance (mAbs)
MUST-KNOW DRUGS
| Drug | Class | Stage | Key Fact |
|---|
| Donepezil | AChEI | All | Once daily; first-line |
| Rivastigmine | AChEI (dual + patch) | All + PD | Only drug for PD dementia; no CYP450 |
| Galantamine | AChEI + nicotinic | Mild-moderate | Mortality warning in MCI |
| Memantine | NMDA antagonist | Moderate-severe | Renal elimination; combine with AChEI |
| Lecanemab | Anti-Aβ mAb | MCI/mild | Full FDA approval 2023; ARIA risk |
| Donanemab | Anti-Aβ mAb | MCI/mild | Full FDA approval 2024; ARIA risk |
MUST-KNOW MECHANISMS
- AChEI: Block AChE → ↑ACh in synapse (symptomatic only)
- Memantine: Uncompetitive, voltage-dependent, open-channel NMDA receptor blocker (neuroprotective)
- Anti-amyloid mAbs: Bind Aβ → microglial phagocytosis → amyloid clearance (disease-modifying)
MUST-KNOW TOXICITIES
- AChEI: BRADYCARDIA (most dangerous), nausea, diarrhea, muscle cramps, vivid dreams, urinary incontinence
- Memantine: Dizziness, confusion, headache, constipation, somnolence (well tolerated)
- Anti-amyloid mAbs: ARIA (edema + microhemorrhages) - requires MRI monitoring
MUST-KNOW CLINICAL USES
- Mild AD: AChE inhibitor alone
- Moderate-severe AD: AChE inhibitor + Memantine
- PD dementia: Rivastigmine only
- MCI/early AD (biomarker-confirmed): Lecanemab or Donanemab
- MCI (uncomplicated): NO approved drug treatment
EXAM EMERGENCY FACTS
- Memantine = moderate-to-severe only
- Rivastigmine = ONLY drug for PD dementia = ONLY AChEI with a patch = ONLY AChEI with no CYP450 metabolism
- Donepezil = once daily = approved for ALL stages = most prescribed
- Most dangerous AChEI adverse effect = BRADYCARDIA
- AChEI + anticholinergic = counterproductive combination
- ARIA = class adverse effect of anti-amyloid antibodies
- Tangles correlate better with dementia severity than plaques
- Galantamine has mortality warning in MCI (cardiovascular)
- Lecanemab/donanemab = ONLY for early AD + biomarker confirmation
- AChE inhibitors do NOT work in MCI
SECTION 10: SELF-ASSESSMENT
10 Short-Answer Questions with Explanations
Q1: A 78-year-old man has mild Alzheimer's disease (MMSE = 22/30). His cardiologist confirms he has no significant cardiac disease. Which drug class should be started, and what is the mechanism of action?
Answer: Start a cholinesterase (AChE) inhibitor - most commonly donepezil 5 mg once daily. The mechanism is reversible inhibition of acetylcholinesterase in the CNS, preventing the breakdown of acetylcholine in the synaptic cleft. This increases the amount and duration of ACh available to bind muscarinic and nicotinic receptors, partially compensating for the progressive loss of cholinergic neurons characteristic of AD.
Q2: Why does memantine have a neuroprotective mechanism, and why is it specifically used in moderate-to-severe AD?
Answer: Memantine is an uncompetitive, low-affinity, voltage-dependent open-channel blocker of NMDA receptors. In AD, dying neurons release tonic (continuous, low-level) glutamate, causing chronic partial NMDA receptor opening. This results in continuous Ca²+ influx - excitotoxicity - that kills more neurons. Memantine blocks this pathological tonic NMDA activation while preserving normal physiological NMDA activation (needed for memory formation). It is neuroprotective because it reduces this Ca²+-mediated neuronal death. It is used in moderate-to-severe AD because that is where sufficient tonic glutamate activity exists to make blocking NMDA receptors clinically meaningful; trials in mild AD showed no significant benefit.
Q3: What makes rivastigmine unique among AChE inhibitors used in Alzheimer's disease? List three features.
Answer:
- Dual enzyme inhibition: Rivastigmine inhibits BOTH acetylcholinesterase (AChE) AND butyrylcholinesterase (BuChE), unlike donepezil and galantamine which mainly inhibit AChE
- No CYP450 metabolism: Rivastigmine is hydrolyzed by AChE itself (carbamylation) and does not use hepatic CYP450 enzymes, resulting in fewer drug-drug interactions
- Only AChE inhibitor approved for Parkinson's disease dementia
- Transdermal patch formulation available: The rivastigmine patch (Exelon patch) allows transdermal delivery, useful for patients with dysphagia or adherence issues, with lower peak plasma levels and thus potentially fewer GI side effects
Q4: A patient with Alzheimer's disease is started on donepezil. Three weeks later, he develops severe diarrhea. His physician prescribes oxybutynin (an anticholinergic drug) to control the diarrhea. Why is this a problematic prescribing decision?
Answer: Oxybutynin is an anticholinergic drug. While its primary indication is reducing bladder overactivity, it crosses the blood-brain barrier and blocks muscarinic ACh receptors in the CNS. The entire goal of donepezil therapy is to increase ACh activity in the brain by preventing its breakdown. By introducing an anticholinergic drug, the physician is directly counteracting the mechanism of donepezil - blocking the very ACh that donepezil worked to preserve. This will worsen cognition. Additionally, patients with AD are exquisitely sensitive to the central anticholinergic effects of drugs. A better solution would be to reduce the donepezil dose, consider switching to the rivastigmine patch (which has a lower peak plasma level and fewer GI side effects), or use non-anticholinergic agents to manage the diarrhea.
Q5: What is ARIA, and in which patient population is it most likely to occur?
Answer: ARIA (Amyloid-Related Imaging Abnormalities) is the major adverse effect of anti-amyloid monoclonal antibodies (lecanemab, donanemab). It occurs because rapid clearance of amyloid from cerebral blood vessel walls (where amyloid also deposits as cerebral amyloid angiopathy) triggers local inflammation. ARIA manifests as:
- ARIA-E (edema): Vasogenic edema seen as white hyperintensity on FLAIR MRI
- ARIA-H (hemorrhage): Microhemorrhages or superficial siderosis seen as dark spots on T2*/SWI MRI
Most cases are asymptomatic, but symptomatic cases can cause headache, confusion, focal neurological deficits, or seizures. ARIA is most likely to occur in:
- ApoE ε4 homozygotes (highest risk - up to 65% of patients)
- ApoE ε4 heterozygotes (intermediate risk)
- Patients with existing cerebral microhemorrhages or cerebral amyloid angiopathy
Q6: A 75-year-old woman with moderate Alzheimer's disease (MMSE = 14/30) is currently on donepezil 10 mg. Her family asks if her medications should be changed. What is the appropriate next step?
Answer: The appropriate next step is to ADD memantine to the existing donepezil therapy, not replace it. At the moderate stage of AD (MMSE 10-19), combining an AChE inhibitor with memantine is the evidence-based standard of care. Memantine targets a different mechanism (NMDA-mediated excitotoxicity) from donepezil (ACh preservation), and the two drugs are complementary. Clinical trials (notably the Howard et al. NEJM 2012 trial) have shown that the combination of donepezil plus memantine is more effective than either drug alone for moderate-to-severe AD. Start memantine at 5 mg once daily and titrate over 4 weeks to the target dose of 10 mg twice daily. Monitor for dizziness, confusion, and headache.
Q7: The number of which pathological feature correlates BEST with the severity of dementia in Alzheimer's disease - amyloid plaques or neurofibrillary tangles?
Answer: Neurofibrillary tangles (tau tangles) correlate better with the degree of dementia than the number of amyloid plaques. This is a classic high-yield exam fact from Robbins Pathology. The Braak staging system for AD grades the spread of neurofibrillary tangles from the entorhinal cortex (stages I-II) through the hippocampus (stages III-IV) to the neocortex (stages V-VI), and this staging correlates well with clinical severity. Amyloid plaque density can be high even in cognitively normal individuals (especially in early stages), while the pattern of tangle spread maps more closely to cognitive decline.
Q8: What is the clinical significance of the Apolipoprotein E (ApoE) genotype in Alzheimer's disease and its drug treatment?
Answer: ApoE has three common alleles: ε2 (protective), ε3 (neutral, most common), and ε4 (risk-increasing). ApoE ε4 is the strongest genetic risk factor for SPORADIC late-onset AD:
- ε4 heterozygotes have ~3x increased risk of AD
- ε4 homozygotes have ~10-15x increased risk
- ApoE ε4 impairs clearance of Aβ from the brain
Drug treatment relevance:
- ApoE ε4 carriers have a significantly higher risk of ARIA when treated with anti-amyloid monoclonal antibodies (lecanemab, donanemab). ε4 homozygotes may be excluded from or require closer monitoring during anti-amyloid therapy
- ApoE genotyping is therefore clinically relevant when considering anti-amyloid antibody therapy - it guides patient selection and risk stratification
Q9: For which indication is galantamine specifically NOT recommended despite being an AChE inhibitor, and why?
Answer: Galantamine is specifically NOT recommended and carries an FDA warning for use in Mild Cognitive Impairment (MCI). In clinical trials of galantamine in MCI patients, there was increased mortality in the galantamine group compared to placebo (1.5% vs. 0.5%), with cardiovascular deaths being the predominant cause. While the exact mechanism is not fully established (possibly cholinergic cardiovascular effects), this finding led the FDA to restrict galantamine use to established Alzheimer's dementia only. AChE inhibitors as a class have been shown to be ineffective for MCI and should not be used for this indication.
Q10: Explain the rationale for combining donepezil and memantine in moderate-to-severe Alzheimer's disease. Why is this combination logical from a pharmacological standpoint?
Answer: The combination is logical because the two drugs target completely different pathological mechanisms and different neurotransmitter systems:
- Donepezil targets the cholinergic deficit - it prevents breakdown of ACh, maximizing the signal from whatever cholinergic neurons remain
- Memantine targets glutamatergic excitotoxicity - it blocks the pathological tonic NMDA receptor activation that is killing neurons from the inside
These mechanisms are complementary and non-overlapping. There is no pharmacological antagonism between them. Their adverse effect profiles are also different and do not summate in a harmful way (AChEIs cause GI upset, bradycardia; memantine causes mild dizziness, constipation). The Howard et al. study (NEJM 2012) confirmed that patients with moderate-to-severe AD on donepezil who were randomized to add memantine showed significantly better outcomes on cognitive and functional scales compared to those who added placebo. A fixed-dose combination product (Namzaric = donepezil + memantine) exists for convenience.
Sources
- Robbins & Kumar Basic Pathology (10th ed.), Chapter 21 - Pathogenesis of Alzheimer disease
- Bradley and Daroff's Neurology in Clinical Practice (8th ed.) - Alzheimer disease diagnosis and treatment
- Lippincott Illustrated Reviews: Pharmacology (8th ed.) - Drugs for Alzheimer disease
- Katzung's Basic and Clinical Pharmacology (16th ed.) - Drugs used in Alzheimer disease
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry - Antidementia drugs
- The Maudsley Prescribing Guidelines in Psychiatry (15th ed.) - Cholinesterase inhibitors
- Harrison's Principles of Internal Medicine (22nd ed., 2025) - Therapies targeting amyloid-β