Hypertension , 65 year old , newly diagnosed , what to give
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypertension" AND "elderly" AND "antihypertensive"
Searching the Web
hypertension 65 year old first line treatment guidelines 2024 2025
Reading File
Reading File
Reading Web Page
https://dig.pharmacy.uic.edu/faqs/2025-2/december-2025-faqs/…
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a thorough, evidence-based answer. Here it is:
Hypertension in a 65-Year-Old - Newly Diagnosed: Management
Step 1 - Confirm the Diagnosis
Before prescribing anything, verify the diagnosis on at least 2-3 separate occasions (or by home/ambulatory BP monitoring). A single reading of 165/95 is not sufficient. White coat hypertension is common in older adults.
Step 2 - Classify and Assess Risk (2025 AHA/ACC Guidelines)
| Stage | BP Reading | Action |
|---|---|---|
| Elevated | SBP 120-129 / DBP <80 | Lifestyle only |
| Stage 1 | SBP 130-139 / DBP 80-89 | Lifestyle first; drugs if 10-yr CVD risk ≥7.5% |
| Stage 2 | SBP ≥140 / DBP ≥90 | Lifestyle + drugs simultaneously |
For a 65-year-old, 10-year CVD risk using the PREVENT calculator (2025 AHA/ACC update) almost certainly exceeds 7.5%, so pharmacotherapy is warranted even in Stage 1 once lifestyle has been tried (or immediately in Stage 2).
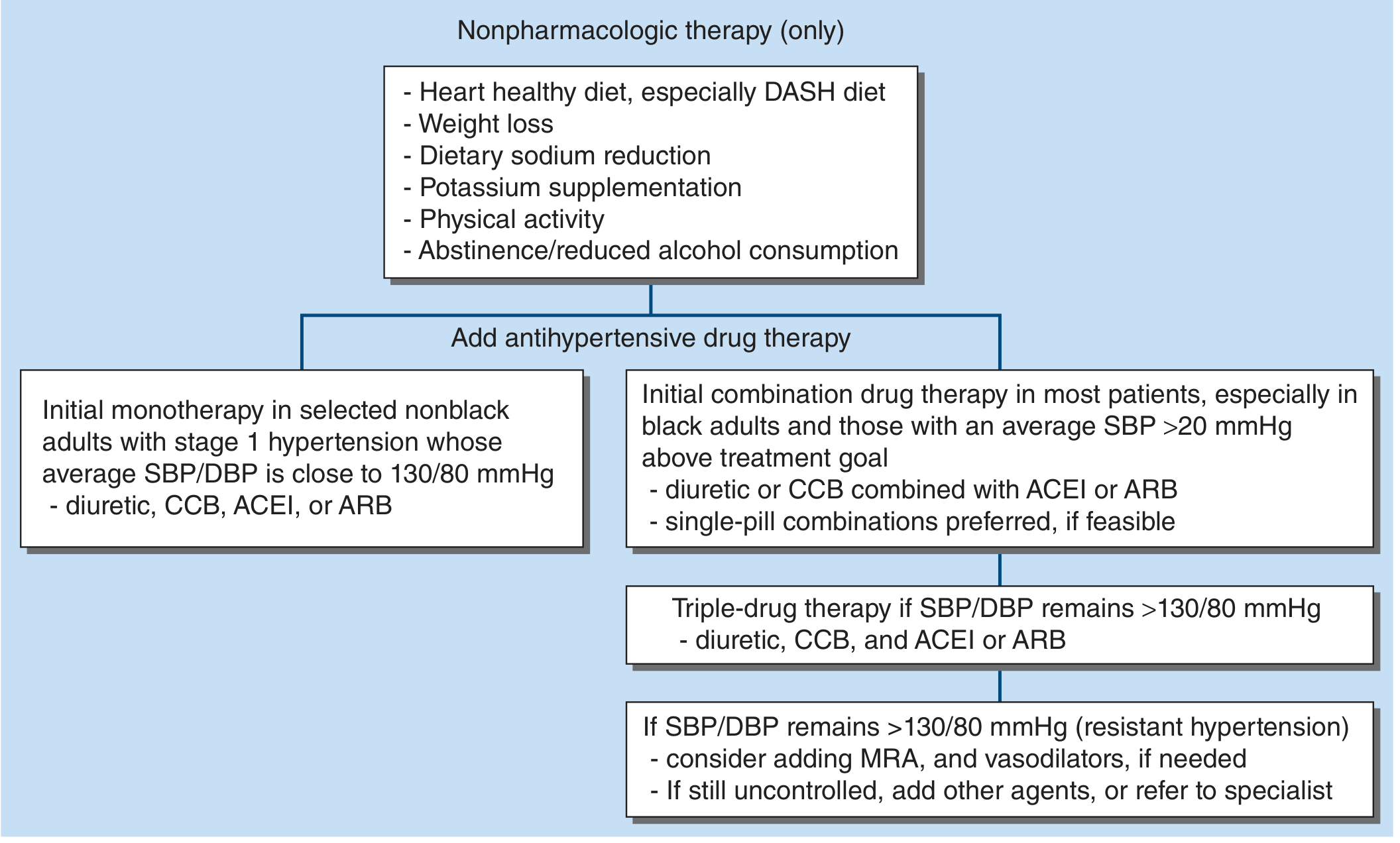
Step 3 - Lifestyle Modifications (Always First-Line, Always Maintained)
Per Harrison's (2025) and the 2025 AHA/ACC guideline:
- DASH diet (fruits, vegetables, low sodium, low saturated fat)
- Sodium restriction to <2.3 g/day (ideally <1.5 g/day)
- Weight loss if overweight
- Physical activity (150 min/week moderate aerobic)
- Limit alcohol
- Stop smoking
These can lower SBP by 4-11 mmHg independently.
Step 4 - First-Line Drug Choices
Four validated first-line drug classes (Goodman & Gilman, Harrison's 22e, Swanson's FM Review):
| Drug Class | Examples | Notes for Age 65 |
|---|---|---|
| Thiazide-type diuretics | Chlorthalidone 12.5-25 mg, Hydrochlorothiazide 12.5-25 mg | Excellent mortality data in elderly; preferred in isolated systolic HTN; watch K+ |
| CCB (dihydropyridine) | Amlodipine 2.5-5 mg | Very effective in elderly; well tolerated; good for isolated systolic HTN; start low |
| ACE inhibitor | Lisinopril 5-10 mg, Ramipril 2.5 mg | Preferred if CKD, diabetes, HFrEF; watch for cough (~10-15%); check K+ and Cr |
| ARB | Losartan 25-50 mg, Valsartan 80 mg | Use if ACEI not tolerated; same indications; no cough |
Beta-blockers are not first-line unless there is a compelling indication (CAD, prior MI, atrial fibrillation, HFrEF). Goodman & Gilman notes elderly patients tend to have a lesser antihypertensive response to beta-blockers.
Alpha-1 blockers (doxazosin, prazosin) are not recommended as monotherapy - associated with worse outcomes in the ALLHAT trial.
Step 5 - Monotherapy vs Combination?
- Stage 1 (SBP 130-139) with BP close to 130/80: start monotherapy (any one of the 4 classes above)
- Stage 2 (SBP ≥140) or SBP >20 mmHg above target: start two-drug combination - preferred is CCB + ACE inhibitor/ARB, or thiazide + ACE inhibitor/ARB in a single-pill combination if feasible (improves adherence, faster control)
Per Harrison's 22e: "Initial combination drug therapy has proven to be more effective for rapid achievement of target BP and medication adherence compared to the stepped-care approach."
Step 6 - BP Target in a 65-Year-Old
Per Harrison's 22e and the 2025 AHA/ACC guidelines:
- Target SBP <130 mmHg in community-dwelling older adults ≥65 years
- DBP <80 mmHg
- For frail elderly or those with significant comorbidities and limited life expectancy, use clinical judgment - aggressive lowering may cause orthostatic hypotension and falls
Practical Approach for a Typical Healthy 65-Year-Old
- Start with amlodipine 5 mg OD (well-tolerated, once-daily, no electrolyte issues, excellent evidence in elderly)
- OR chlorthalidone 12.5 mg OD if cost is a concern or if the patient has edema
- OR an ACE inhibitor/ARB if the patient has diabetes, CKD, or proteinuria
- Review in 4 weeks - titrate dose or add second agent if BP not at goal
- If BP still not controlled: add a second drug (CCB + ACE inhibitor/ARB, or thiazide + ACE inhibitor/ARB)
- Triple therapy if needed: diuretic + CCB + ACE inhibitor/ARB
Special Situations at 65
| Comorbidity | Preferred Class |
|---|---|
| Diabetes / CKD with albuminuria | ACE inhibitor or ARB (first choice) |
| Prior MI / Stable CAD | Beta-blocker + ACE inhibitor |
| Heart failure with reduced EF | ACE inhibitor/ARB + beta-blocker + diuretic |
| Atrial fibrillation (rate control) | Beta-blocker or rate-limiting CCB (diltiazem/verapamil) |
| Isolated systolic HTN | Thiazide or dihydropyridine CCB |
| BPH (enlarged prostate) | Alpha-blocker can be added (not monotherapy) |
| African American patients | CCB or thiazide preferred; ACE inhibitor less effective as monotherapy |
Treatment Algorithm (Harrison's 22e)
Recent Evidence Note
A 2025 Cochrane systematic review (PMID: 41065416) on antihypertensive treatment in adults ≥60 years confirmed benefit of treatment in reducing stroke, MI, and mortality. The 2025 AHA/ACC guideline adopted the PREVENT risk calculator to guide treatment initiation - nearly all 65-year-olds will cross the 7.5% 10-year CVD risk threshold, making drug treatment appropriate.
Sources: Harrison's Principles of Internal Medicine 22e (2025), Goodman & Gilman's Pharmacological Basis of Therapeutics, Swanson's Family Medicine Review, 2025 AHA/ACC Hypertension Guidelines.
45 year old male, Hba1c 8.6 , what to prescribe
Finding Sources
Searching PubMed
"type 2 diabetes" AND "glycemic control" AND "treatment"
Searching the Web
type 2 diabetes HbA1c 8.5 treatment guidelines 2024 2025 ADA first line
Finding Sources
Reading Article
PMID: 41842862
Reading Web Page
https://www.explorationpub.com/Journals/eemd/Article/101428
Finding Sources
Reading Web Page
https://www.wafp.org/assets/files/2025_ADA_Updates_All_Secti…
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive data from Harrison's 22e, Lippincott Pharmacology, the 2025 ADA Standards, the 2026 AACE algorithm, and recent PubMed evidence. Here is the full clinical answer:
Type 2 Diabetes - 45-Year-Old Male, HbA1c 8.6%: What to Prescribe
Interpreting the HbA1c
| HbA1c | Meaning |
|---|---|
| <5.7% | Normal |
| 5.7-6.4% | Prediabetes |
| ≥6.5% | Diabetes |
| 8.6% | Poorly controlled T2DM - ~1.6% above the standard target of <7% |
An HbA1c of 8.6% in a 45-year-old means he has had sustained hyperglycemia (estimated average glucose ~200 mg/dL). Lifestyle alone will not bring this to target. Dual therapy from the start is appropriate per current guidelines.
Step 1 - Always: Lifestyle Modification (Non-Negotiable)
- Diet: Low-calorie, low-carbohydrate or DASH-style diet; reduce refined sugars and processed carbs
- Exercise: At least 150 min/week aerobic activity + resistance training (2025 ADA emphasis)
- Weight loss: If overweight/obese - even 5-10% weight reduction significantly improves glycemia
- Smoking cessation if applicable
- Alcohol: Reduce or eliminate
These are foundational and must accompany all pharmacotherapy.
Step 2 - First Ask: Are There Comorbidities?
The 2025 ADA and 2026 AACE guidelines use a comorbidity-first approach - don't just chase glucose, treat the whole patient.
| Comorbidity Present? | Drug of Choice (independent of HbA1c) |
|---|---|
| Established ASCVD (prior MI, stroke, CAD) | GLP-1 RA (liraglutide, semaglutide) OR SGLT2i (empagliflozin, dapagliflozin) |
| Heart failure (HFrEF or HFpEF) | SGLT2 inhibitor first; GLP-1 RA for HFpEF + obesity |
| CKD (eGFR 20-60 or albuminuria ACR >30) | SGLT2 inhibitor (renoprotective) + ACE inhibitor/ARB |
| Obesity (the typical 45-yr-old T2DM patient) | GLP-1 RA or GIP/GLP-1 dual agonist (tirzepatide) |
| MASLD/fatty liver | GLP-1 RA or tirzepatide |
| No major comorbidity | Metformin + second agent as below |
Step 3 - For a Typical 45-Year-Old Male Without Major Comorbidity
HbA1c 8.6% = Combination therapy from day 1 (2025 ADA, 2026 AACE)
Recommended Regimen:
Option A - Best overall (obese or overweight, which most T2DM patients are):
Metformin + GLP-1 RA (or GIP/GLP-1 dual agonist)
| Drug | Dose | Notes |
|---|---|---|
| Metformin XR | Start 500 mg OD with dinner → titrate to 1000 mg BD over 4 weeks (max 2000 mg/day) | First-line backbone; reduces hepatic glucose output; weight neutral to modest weight loss; no hypoglycemia; cheap |
| + Semaglutide (Ozempic) | 0.25 mg SC weekly × 4 weeks → 0.5 mg → 1 mg → max 2 mg | Reduces HbA1c by 1.5-2%; weight loss 4-6 kg; CV protection; once weekly injection |
| OR + Tirzepatide (Mounjaro) | 2.5 mg SC weekly → titrate q4 weeks | Dual GIP/GLP-1 agonist; superior HbA1c reduction (~2.1%); significant weight loss (10-15 kg); 2026 AACE preferred |
| OR + Liraglutide (Victoza) | 0.6 mg SC daily → 1.2 mg → 1.8 mg | Proven CV mortality reduction (LEADER trial); daily injection |
Option B - If cost is a concern or patient prefers oral medications:
Metformin + SGLT2 inhibitor
| Drug | Dose | Notes |
|---|---|---|
| Metformin XR | As above | |
| + Empagliflozin (Jardiance) | 10 mg OD (can go to 25 mg) | CV and renal protection; weight loss 2-3 kg; lowers SBP; once daily oral |
| OR + Dapagliflozin (Forxiga) | 10 mg OD | CV/renal benefits; proven in HF |
| OR + Canagliflozin (Invokana) | 100 mg OD with first meal |
Option C - Most cost-effective (resource-limited setting):
Metformin + Sulfonylurea
| Drug | Dose | Notes |
|---|---|---|
| Metformin | As above | |
| + Glimepiride | 1-2 mg OD with breakfast | Risk of hypoglycemia + weight gain; very cheap; still reduces microvascular complications |
| OR + Gliclazide MR | 30-60 mg OD | Lower hypoglycemia risk than glibenclamide |
Note: 2025 ADA guidance explicitly states: "STOP sulfonylureas and DPP-4 inhibitors when initiating GLP-1 RA or SGLT2i - they add no CV/kidney/weight benefit and increase hypoglycemia risk."
Drug Class Summary Table
| Class | HbA1c Reduction | Weight Effect | Hypoglycemia | CV/Renal Benefit | Cost |
|---|---|---|---|---|---|
| Metformin | 1-1.5% | Neutral/mild loss | No | Neutral | Low |
| GLP-1 RA (semaglutide) | 1.5-2% | -4-6 kg | No | Yes (CV protection) | High |
| GIP/GLP-1 (tirzepatide) | 2-2.5% | -10-15 kg | No | Yes | High |
| SGLT2i (empagliflozin) | 0.5-1% | -2-3 kg | No | Yes (CV + renal) | High |
| DPP-4i (sitagliptin) | 0.5-0.8% | Neutral | No | Neutral | Medium |
| Sulfonylurea (glimepiride) | 1-1.5% | +1-2 kg | Yes | No | Low |
| Basal Insulin (glargine) | 1.5-2.5% | +2-4 kg | Yes | No | Medium |
When to Consider Adding Basal Insulin
- HbA1c remains >9-10% despite dual therapy, OR
- Patient is symptomatic (polyuria, polydipsia, significant weight loss), OR
- After 3 months of combination oral therapy with inadequate response
Basal insulin: Insulin glargine (Lantus/Toujeo) 0.1-0.2 U/kg at bedtime, titrate by 2 units every 3 days until fasting glucose 80-130 mg/dL. Continue metformin + SGLT2i/GLP-1 RA alongside insulin.
Harrison's 22e: "The addition of a GLP-1 RA can limit weight gain and reduce the dose of insulin needed."
HbA1c Target for This Patient
| Scenario | HbA1c Target |
|---|---|
| Typical 45-year-old, healthy, motivated | <7% |
| Long life expectancy, can tolerate tight control | <6.5% (AACE) |
| If adding agents with hypoglycemia risk (SFU/insulin) | <7% to minimize risk |
Monitoring Plan
- HbA1c: Every 3 months until at goal, then every 6 months
- Fasting glucose / home SMBG: Daily or as needed (CGM now recommended by 2025 ADA even on non-insulin agents)
- Renal function (eGFR, Cr, K+): Baseline and annually; before starting SGLT2i
- Urine ACR: Baseline - if >30 mg/g, prioritize SGLT2i + ACEi/ARB
- Lipid panel: Statin indicated if LDL >70 mg/dL (high CV risk with diabetes)
- BP: Target <130/80 mmHg
- Ophthalmology review: At diagnosis, then annually
- Foot exam: Annually
Practical Prescription for a Healthy 45-Year-Old Male, HbA1c 8.6%, No Comorbidities, Overweight
- Metformin XR 500 mg OD with dinner - increase by 500 mg every 2 weeks to 1000 mg BD
- + Semaglutide 0.25 mg SC weekly (if affordable) - titrate every 4 weeks up to 1 mg (or tirzepatide if available)
- OR Empagliflozin 10 mg OD (oral, once daily - if injectable not preferred)
- OR Glimepiride 1 mg OD (if cost is the limiting factor)
- Recheck HbA1c in 3 months - if still >7%, uptitrate or add third agent
- Screen and treat co-existing hypertension, dyslipidemia
Key Recent Evidence
- The 2026 AACE Consensus (PMID: 41842862) emphasizes a comorbidity-centric approach with GLP-1 RA or SGLT2i as central to T2DM management beyond glucose control.
- A 2025 JAMA network meta-analysis (PMID: 39899304) found age and sex differences in drug efficacy - middle-aged males respond well to GLP-1 RA and SGLT2i.
- The 2025 ADA Standards expanded GLP-1 RA indications to include MASLD/MASH, HFpEF with obesity, and CKD regardless of HbA1c level.
Sources: Harrison's Principles of Internal Medicine 22e (2025), Lippincott Illustrated Reviews Pharmacology, 2025 ADA Standards of Care, 2026 AACE T2DM Algorithm.
This is a shared conversation. Sign in to Orris to start your own chat.