scfe 10 marks ms ortho 3 easy handdrawn pencil diagrams
Hand-drawn pencil sketch diagram for medical exam showing SCFE (Slipped Capital Femoral Epiphysis) anatomy. Draw a proximal femur with the femoral head (epiphysis) displaced posteriorly and medially off the femoral neck at the growth plate (physis). Label: Femoral Head (Epiphysis), Physis (growth plate), Femoral Neck, Greater Trochanter, Lesser Trochanter. Show the direction of slip with an arrow labelled "Posterior & Inferior slip". Include a small inset showing normal hip next to SCFE hip for comparison. Style: rough pencil sketch on white paper, handwritten labels, educational anatomy diagram style
Hand-drawn pencil sketch diagram for medical exam showing SCFE X-ray findings on AP pelvis view. Draw a pelvis with two hip joints. On the normal side, draw Klein's line (a straight line along the superior femoral neck) intersecting the lateral edge of the femoral head epiphysis. On the SCFE side, draw the same Klein's line passing ABOVE the femoral head (not intersecting it) because the epiphysis has slipped medially. Label: "Klein's line", "Normal - line intersects epiphysis", "SCFE - line misses epiphysis (Trethowan's sign positive)", "Widening and irregularity of physis". Also label: medial joint space, acetabulum. Style: rough pencil sketch on white paper, handwritten labels, educational orthopaedics exam diagram
Hand-drawn pencil sketch diagram for medical exam showing SCFE grading and in-situ pinning treatment. Left side: draw three proximal femurs showing Grade 1 (less than 33% slip), Grade 2 (34-50% slip), Grade 3 (more than 50% slip) with the epiphysis progressively more displaced posteriorly, labelled accordingly. Right side: draw the in-situ single cannulated screw fixation - a proximal femur with one screw entering anteriorly on the femoral neck and ending centrally in the femoral head, crossing the physis perpendicularly. Label: "Starting point: anterior femoral neck", "Screw tip: central in femoral head", "Perpendicular to physis". Style: rough pencil sketch on white paper, handwritten labels, educational orthopaedics exam diagram
Diagram 1 - SCFE Anatomy (The Slip)

- Epiphysis slips posteriorly, medially, and inferiorly relative to the neck
- Slip occurs through the hypertrophic zone of the physis (zone of Ranvier)
- Neck moves anteriorly and superiorly (NOT the head moving - the neck rides up)
- Mnemonic: "Ice cream slides off the cone"
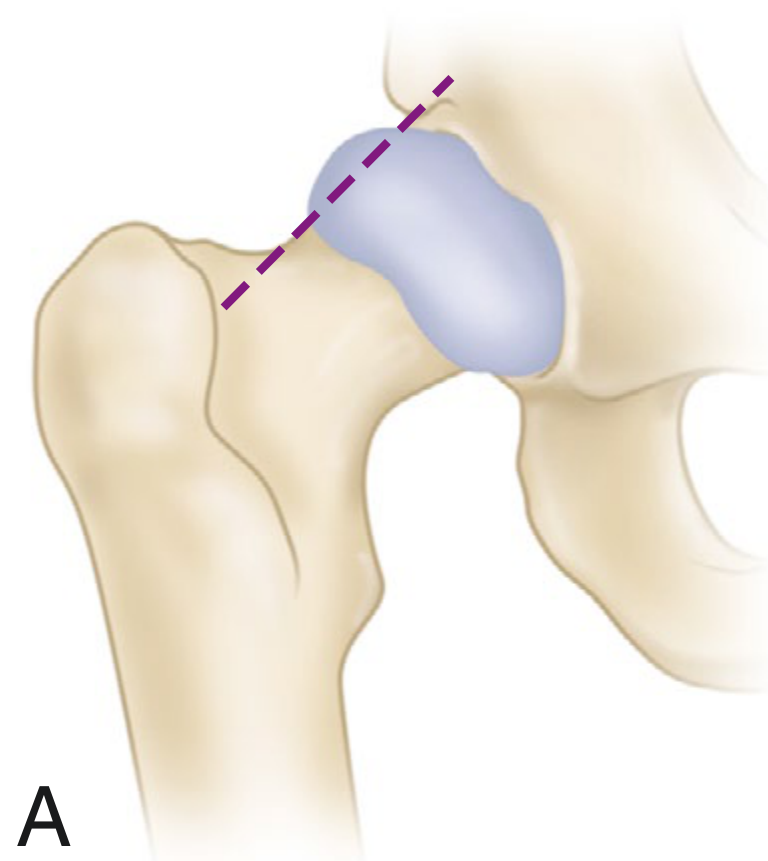
Diagram 2 - Klein's Line / Trethowan's Sign (AP X-ray)
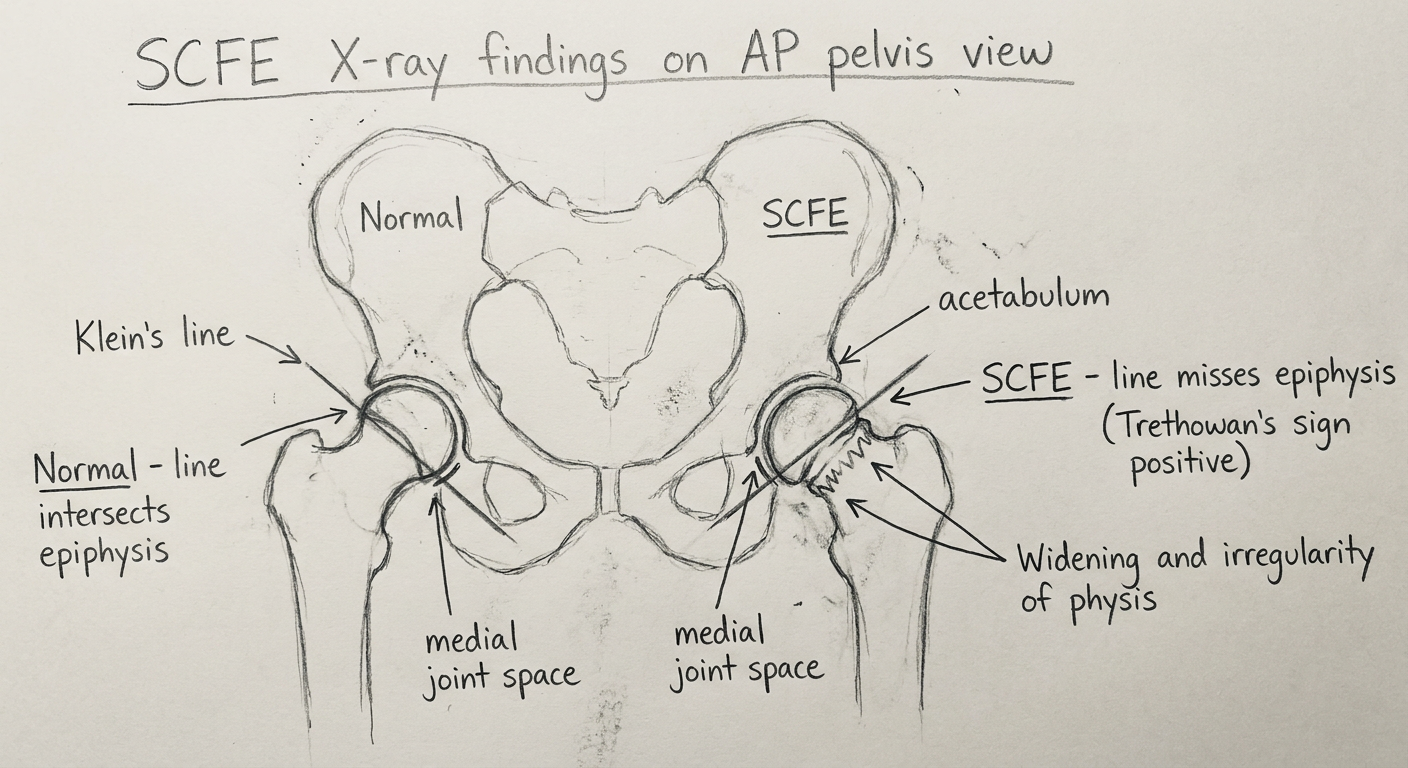
- Klein's line = drawn along the superior border of femoral neck on AP view
- Normal: line intersects at least 1/5th of femoral head
- SCFE: line passes entirely above the head - Trethowan's sign positive
- Additional signs: widened physis, metaphyseal blanch sign (Steel's sign), decreased head-neck offset
Diagram 3 - Grading + In-Situ Pinning Treatment
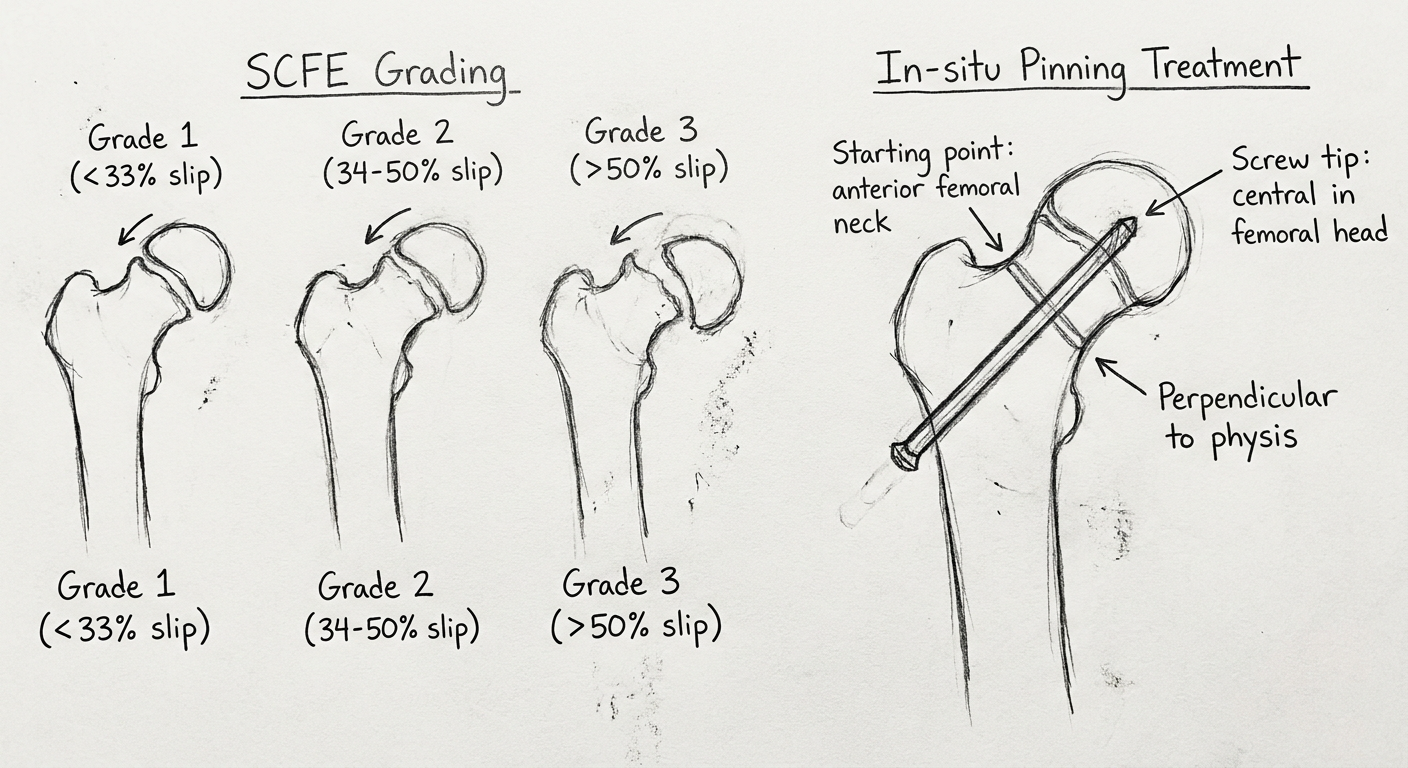
| Grade | Slip |
|---|---|
| I (Mild) | < 33% |
| II (Moderate) | 33-50% |
| III (Severe) | > 50% |
- Stable - can weight bear (with or without crutches) → AVN risk ~0%
- Unstable - cannot weight bear → AVN risk up to 47%
- Single cannulated 7.3 mm screw
- Entry point: anterior on femoral neck (to account for posterior slip)
- Tip: central position in femoral head
- Crosses physis perpendicularly (aim for centre-centre position)
- Do NOT attempt forceful reduction → dramatically increases AVN risk
Quick Answer Framework for 10 Marks
| Heading | Points |
|---|---|
| Definition + Epidemiology | Posterior slip of CFE at proximal femoral physis; peak 10-16 yr; obese boys; bilateral in 20-40% |
| Aetiology | Weakened hypertrophic zone physis due to obesity, hormonal factors (hypothyroidism, GH excess), shear forces |
| Clinical features | Limp, hip/knee pain, external rotation + shortening deformity, limited internal rotation |
| X-ray (Diagram 2) | Klein's line, Trethowan sign, widened physis, AP + frog-leg lateral |
| Classification | Loder (stable/unstable) + Grade I/II/III |
| Treatment (Diagram 3) | In-situ pinning; no forceful reduction; modified Dunn for severe unstable |
| Complications | AVN (most severe), chondrolysis, FAI, OA |
structed answer for scfe knruhs ms ortho theory exams
KNRUHS MS Ortho theory exam SCFE question pattern structured answer
SLIPPED CAPITAL FEMORAL EPIPHYSIS (SCFE)
Structured Answer - KNRUHS MS Ortho Theory Exam
DEFINITION
Technically a Salter-Harris Type I fracture-separation through the hypertrophic zone of the physis.
INCIDENCE / EPIDEMIOLOGY
- Most common hip disorder of adolescence
- Age: 10-16 years (during rapid growth spurt, Risser grade 0)
- Sex: Males > Females (2:1)
- Race: Twice as common in African than European descent
- Bilateral in 25-40% of cases; second slip usually within 12-18 months
- Left side more commonly involved (65%) when unilateral
- Elevated serum leptin levels associated regardless of BMI
AETIOLOGY / RISK FACTORS
Mechanical factors:
- Obesity (increased shear at physis)
- Increased obliquity of physis with growth
- Thinning of perichondrial ring
- Decreased neck-shaft angle (coxa vara)
- Femoral retrotorsion + acetabular retroversion
Hormonal / systemic factors:
| Condition | Mechanism |
|---|---|
| Hypothyroidism (most common) | Weakened physis |
| Growth hormone deficiency | Physeal changes |
| Hypogonadism / panhypopituitarism | Delayed skeletal maturity |
| Renal osteodystrophy | Metabolic bone disease |
| Down syndrome | Hypotonia + hormonal |
Rule: Any child < 10 years with SCFE - mandatory endocrine workup.
PATHOANATOMY
- Slip occurs through the hypertrophic zone of the physis (zone of provisional calcification)
- The perichondrial ring is weakened by hormonal/mechanical factors
- The neck moves anteriorly and rotates externally (NOT the head moving posteriorly)
- Mnemonic: "Ice cream sliding off the cone"
- Reliable orientation of lateral epiphyseal vessels adjacent to the tubercle explains the low rate of AVN in stable, chronic slips
CLINICAL FEATURES
Symptoms:
- Pain in groin, hip, medial thigh, or knee (referred via obturator nerve - missed diagnosis!)
- Limp (antalgic + Trendelenburg gait)
- Chronic: mild shortening, fixed external rotation deformity
Signs:
| Sign | Description |
|---|---|
| Obligate external rotation | Hip externally rotates on flexion - PATHOGNOMONIC |
| Drehmann sign | Same as above - external rotation with flexion |
| Decreased internal rotation | Most consistent finding |
| Thigh atrophy | In chronic cases |
| Trendelenburg positive | Gluteus medius weakness |
Diagnostic trap: SCFE should be suspected in any obese 10-16 year old with knee pain - always examine the hip!
CLASSIFICATION
1. Loder Classification (MOST IMPORTANT - prognostic)
| Type | Definition | AVN Risk |
|---|---|---|
| Stable | Weight bearing possible (with/without crutches) | < 10% |
| Unstable | Cannot weight bear even with crutches | 24-47% |
2. Temporal Classification (descriptive, no prognostic value)
- Acute: symptoms < 3 weeks
- Chronic: symptoms > 3 weeks
- Acute-on-chronic: acute exacerbation of chronic symptoms
3. Southwick Grading (% of slippage on frog-leg lateral)
| Grade | Slip angle |
|---|---|
| Grade I (Mild) | 0-33% / < 30° |
| Grade II (Moderate) | 34-50% / 30-50° |
| Grade III (Severe) | > 50% / > 50° |
INVESTIGATIONS
X-Ray (first-line investigation):
- Frog-leg lateral is MORE sensitive - do not skip it
- Cross-table lateral for unstable slips (avoid positioning)
AP Radiograph Signs:
| Sign | Description |
|---|---|
| Klein's line (Trethowan's sign) | Line along superior femoral neck - normally intersects lateral 1/5 of epiphysis. In SCFE it misses the head entirely |
| Metaphyseal blanch sign (Steel's sign) | Double density at metaphysis due to anterior overlap |
| Widening/irregularity of physis | Early sign |
| Decreased head-neck offset | Loss of spherical contour |
Frog-leg lateral:
- Best view to demonstrate degree of slip (Southwick angle measured here)
- Shows posterior displacement clearly
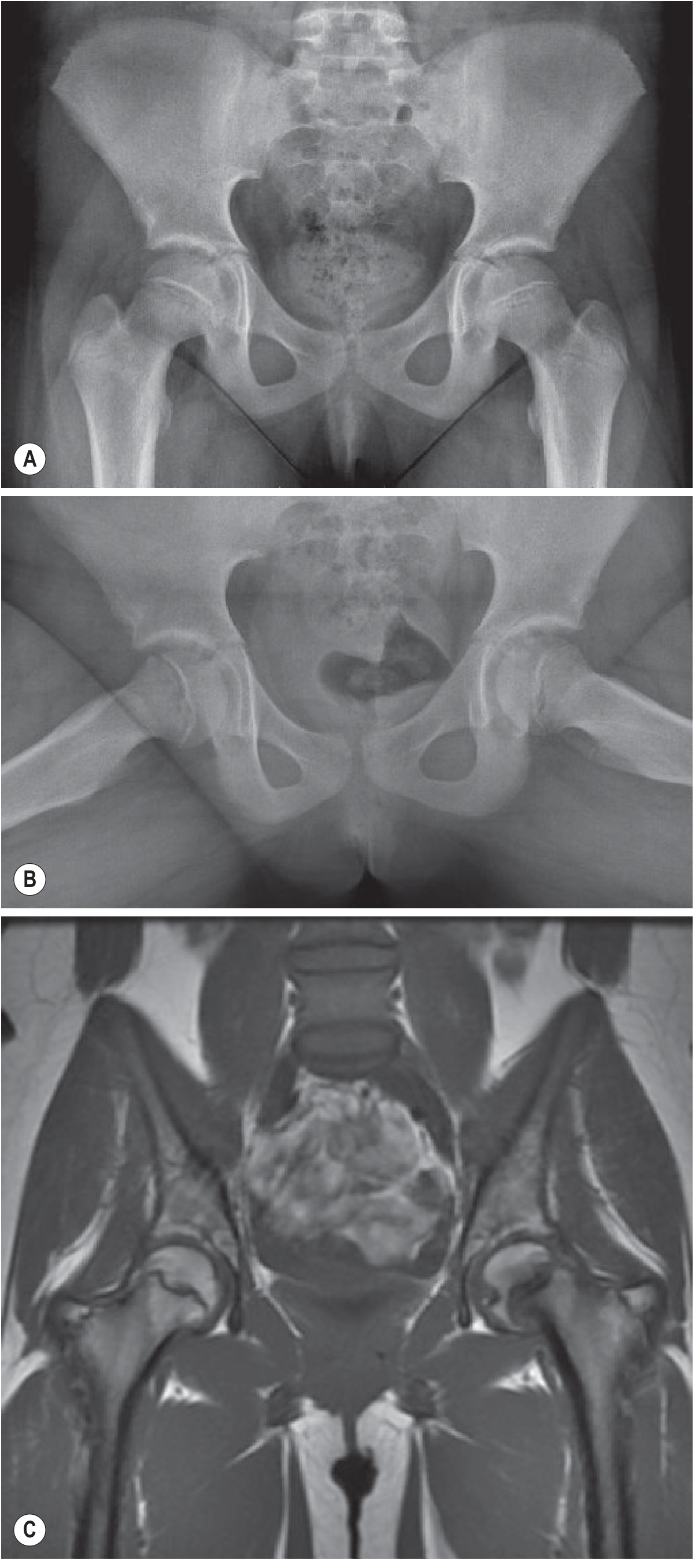
MRI:
- Pre-slip: physeal edema on T2
- Assess femoral head perfusion (unstable slips)
- Rule out additional hip pathology
CT:
- Check if physis is closed
- Pre-operative planning for complex osteotomies
TREATMENT
Principle: Stabilize, do NOT reduce forcefully
Forceful reduction causes AVN - absolutely contraindicated in chronic slips.
A. In-Situ Pinning (Treatment of choice for ALL grades, stable and unstable)
- Patient supine on fracture/radiolucent table
- Image intensifier (C-arm) for AP + true lateral views
- Entry point: anterior on femoral neck (to account for posterior slip)
- Single 7.3 mm cannulated screw, perpendicular to physis
- Tip: central position in femoral head (centre-centre) - no closer than 4 mm from subchondral bone
- Confirm on multiple fluoroscopic views - avoid screw penetration
- Stabilize the epiphysis
- Promote closure of proximal femoral physis
- Prevent further slippage
B. Unstable SCFE - Additional considerations:
- Urgent stabilization within 24 hours
- Capsulotomy to decompress the haemarthrosis (reduces AVN risk)
- Gentle "finger reduction" if possible - avoid forceful manipulation
- Modified Dunn technique (surgical hip dislocation) for severe unstable slips
C. Modified Dunn (Subcapital Realignment):
- Surgical hip dislocation via Ganz approach
- Neck shortening + periosteal retinacular flap preservation
- For moderate-severe chronic slips with deformity
- Preserves blood supply via trochanteric flip osteotomy
D. Osteotomies (for residual deformity/FAI):
| Type | Indication |
|---|---|
| Imhäuser intertrochanteric osteotomy | Moderate-severe chronic SCFE with FAI |
| Subcapital cuneiform osteotomy | Severe deformity at skeletal maturity |
| Arthroscopic/open osteochondroplasty | Residual cam-FAI after in-situ fixation |
E. Prophylactic Pinning of Contralateral Hip:
- Age < 10 years (female) or < 12 years (male)
- Endocrine abnormality present
- Posterior sloping angle > 12 degrees
- Open triradiate cartilage
- Unreliable follow-up
- Hypothyroidism, low Vit D, DM, GH use history
COMPLICATIONS
1. Avascular Necrosis (AVN) - Most feared
- Stable slips: practically 0% risk
- Unstable slips: 24-47% risk
- Due to disruption of the retinacular vessels (lateral epiphyseal vessels)
- Anterior physeal separation on imaging is a sign of high AVN risk (Ballard sign)
- Management: core decompression, vascularized fibular graft, THA in adults
2. Chondrolysis
- Diagnosis: joint space < 3 mm (normal 4-6 mm) + decreased ROM
- Incidence decreased from 7% to 1% with improved surgical technique
- Causes: pin penetration, prolonged immobilization, immune-mediated
- Management: NSAIDs, physiotherapy, joint distraction
3. Femoroacetabular Impingement (FAI)
- Cam-type FAI from residual neck deformity
- Leads to early osteoarthritis
- 22% of hips coming to THA in North America had SCFE-associated OA
4. Other:
- Premature physeal closure + limb length discrepancy
- Coxa vara
- Femoral neck fracture (post-pinning complication)
- Degenerative osteoarthritis (long term)
DIFFERENTIALS (to mention briefly)
| Condition | Differentiating point |
|---|---|
| Perthes disease | Younger age (4-8 yr), AVN of head, no slip |
| Transient synovitis | Afebrile, no radiological changes, self-limiting |
| Septic arthritis | Fever, raised WBC/CRP, hip held in FABER |
| Juvenile idiopathic arthritis | Multiple joints, serology positive |
EXAM-READY SUMMARY BOX
| Parameter | Key Fact |
|---|---|
| Age | 10-16 years |
| Sex | Male > Female (2:1) |
| Site of slip | Hypertrophic zone of physis |
| Direction | Neck anterior + external rotation; head stays in acetabulum |
| Bilateral | 25-40% |
| Best X-ray view | Frog-leg lateral |
| Best sign on AP | Trethowan's sign (Klein's line) |
| Classification | Loder (stable/unstable) - prognostic |
| Treatment | In-situ single cannulated screw fixation |
| No. of screws | Single screw (standard) |
| Entry point | Anterior femoral neck |
| Most feared complication | AVN (47% in unstable) |
| Forceful reduction | ABSOLUTELY CONTRAINDICATED |
| Endocrine workup | Child < 10 years |