Chalizioma
Reading File
Finding Sources
Finding Sources
Searching PubMed
chalazion treatment management
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Chalazion (Meibomian Cyst)
Definition
A chalazion is a sterile, chronic granulomatous inflammatory lesion (lipogranuloma) of the meibomian gland (or occasionally the gland of Zeis) in the eyelid, caused by obstruction of the gland duct with retained lipid-rich sebaceous secretions. The retained material acts as a foreign body, triggering a granulomatous foreign-body inflammatory reaction.
- Goldman-Cecil Medicine, p. 302
- Kanski's Clinical Ophthalmology 10th ed., p. 54
Pathogenesis & Histology
The blocked meibomian gland secretion forms a collection that stimulates:
- Lipogranulomatous inflammation - extracellular fat deposits
- Surrounded by lipid-laden epithelioid cells and multinucleated giant cells
- Background infiltrate of lymphocytes
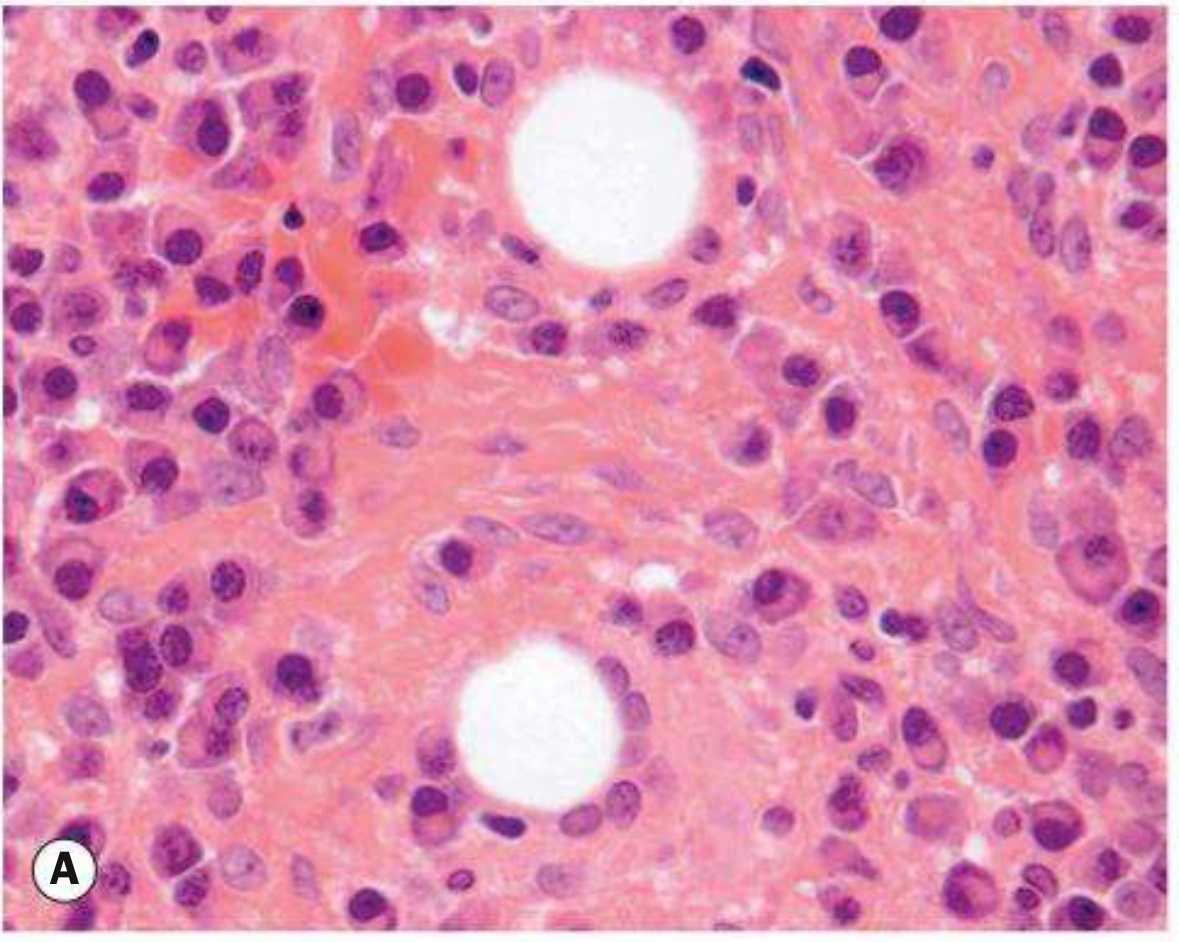
Histopathology (Fig. A below): lipogranuloma with large pale epithelioid cells and well-demarcated empty spaces (fat dissolved out during processing)
Clinical appearance (Fig. B): painless, firm nodule in the upper or lower eyelid

Associated Conditions
| Condition | Relevance |
|---|---|
| Blepharitis | Commonly co-present |
| Acne rosacea | Associated with multiple/recurrent chalazia |
| Bortezomib (proteasome inhibitor for myeloma) | Predisposes to chalazia within 3 months of initiation |
| Sebaceous carcinoma | Must be excluded in recurrent lesions, especially in older patients |
Symptoms & Signs
Symptoms: Acute or chronic eyelid lump, swelling, tenderness (can be painless or painful)
Critical sign: Visible or palpable, well-defined, subcutaneous nodule in the eyelid
Other signs:
- Blocked meibomian gland orifice
- Eyelid swelling and erythema
- Focal tenderness
- Associated blepharitis or acne rosacea
- Lesion may drain mucopurulent material
Chalazion vs. Hordeolum
| Feature | Chalazion | Hordeolum (Stye) |
|---|---|---|
| Nature | Sterile, chronic granulomatous | Acute bacterial abscess |
| Gland involved | Meibomian (± Zeis) | Meibomian (internal) / Zeis or Moll (external) |
| Pain | Painless or mildly tender | Painful |
| Organism | None (sterile) | Usually Staphylococcus spp. |
| Nodule | Well-defined, firm, non-mobile | Tender, may point at lid margin |
Differential Diagnosis
- Preseptal cellulitis - periorbital erythema, edema, warmth
- Sebaceous carcinoma - recurrent chalazia, eyelid thickening, madarosis, chronic unilateral blepharitis in older patients
- Pyogenic granuloma - benign, red, pedunculated conjunctival lesion
- Forniceal foreign body - especially in contact lens wearers
Key clinical tip: If a chalazion recurs at the same lid position in an older patient, biopsy is mandatory to exclude malignancy (sebaceous carcinoma). - Kanski's Clinical Ophthalmology
Workup
- History: Previous ocular surgery/trauma? Previous chalazia?
- External examination: Palpate eyelid for nodule; look for rosacea
- Slit lamp: Evaluate meibomian glands for inspissation, evert eyelid; assess for madarosis, poliosis, ulceration
Treatment
Step 1 - Conservative (all cases)
- Warm compresses for at least 10 minutes 4x daily with gentle massage over the lesion
- Most lesions resolve over days to weeks
Step 2 - Medical (if needed)
- Topical antibiotic/steroid (e.g., neomycin/polymyxin B/dexamethasone ointment b.i.d. for 1-2 weeks)
- Chronic low-dose doxycycline 20-50 mg p.o. daily to b.i.d. for multiple/recurrent chalazia or ocular rosacea (antibacterial + anti-inflammatory)
Step 3 - Procedural (failure after 3-4 weeks)
Option A: Incision and curettage (I&C)
- Chalazion clamp applied with open side inside the eyelid
- Vertical incision through conjunctival surface
- Curettage of contents
Option B: Intralesional steroid injection
- Triamcinolone 40 mg/mL mixed 1:1 with 2% lidocaine with epinephrine (0.2-1.0 mL total, depending on lesion size)
- Alternatives: betamethasone combinations or dexamethasone sodium phosphate 4 mg/mL
Warning on steroid injection: Can cause permanent depigmentation or skin atrophy at the injection site - especially in dark-skinned individuals. Rarely, vigorous injection can cause retrograde intra-arterial infiltration with central retinal artery occlusion. Use with detailed patient counselling.
All removed specimens - send to pathology
Especially recurrent or atypical chalazia.
Follow-Up
-
Medical therapy: reassess only if lesion persists beyond 3-4 weeks
-
After I&C: reexamine as needed
-
The Wills Eye Manual, pp. 381-383
-
Kanski's Clinical Ophthalmology 10th ed., p. 54
-
Goldman-Cecil Medicine, p. 302
This is a shared conversation. Sign in to Orris to start your own chat.