Role of magnesium in Anesthesia and ICU
Reading File
Finding Sources
Finding Sources
Searching PubMed
magnesium sulfate anesthesia perioperative
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching PubMed
magnesium ICU critically ill patients outcomes
Loading Image
Reading File
I have very rich content. Let me now compile the comprehensive, well-organized response.
Magnesium in Anesthesia and Critical Care (ICU)
1. Physiology and Basic Pharmacology
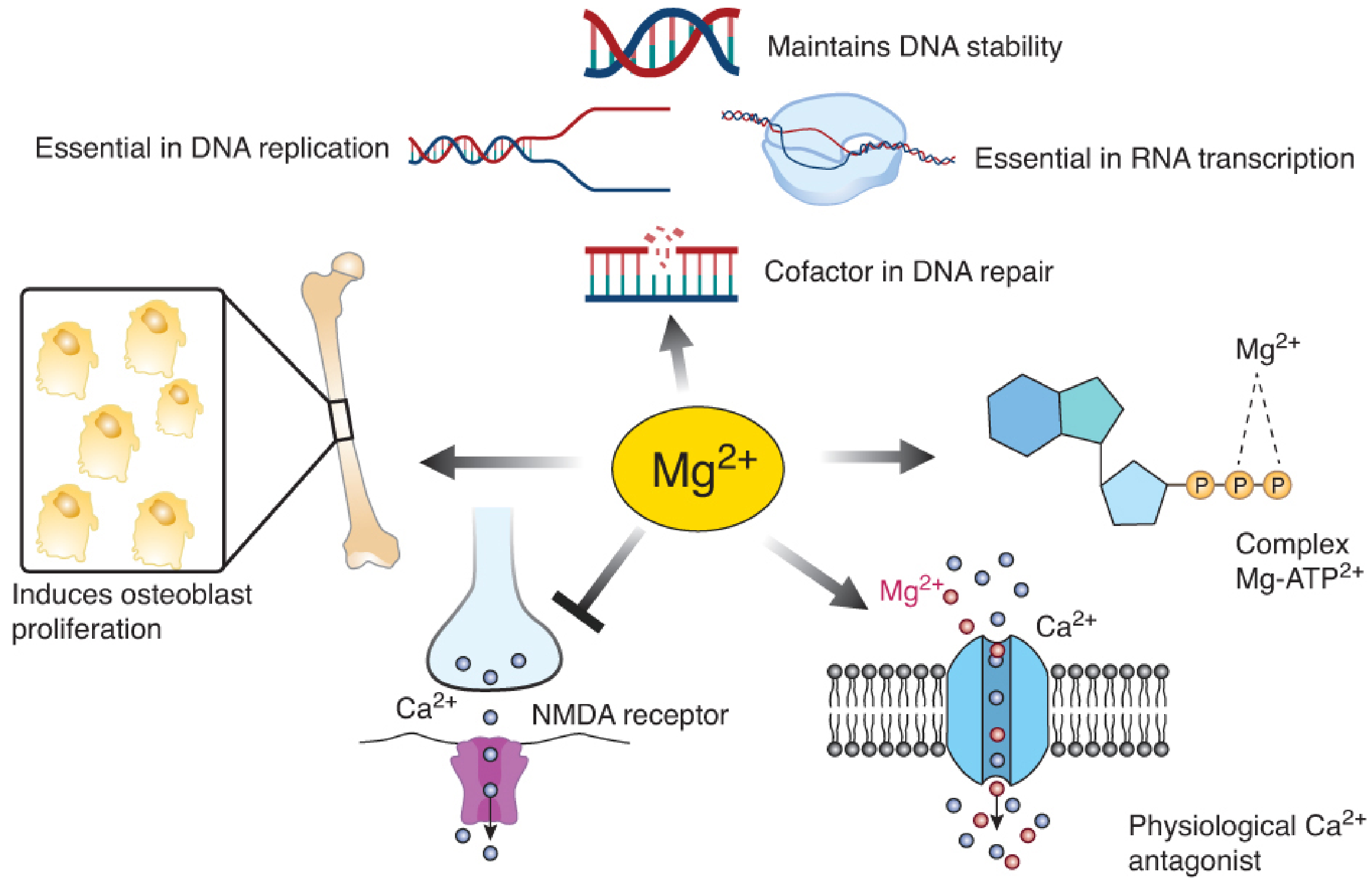
Magnesium (Mg2+) is the second most abundant intracellular cation in the body. Its physiological roles relevant to anesthesia include:
- NMDA receptor antagonism - blocks the voltage-gated Mg2+ channel of the NMDA receptor, explaining its analgesic and neuroprotective properties
- Physiological Ca2+ antagonist - competes with Ca2+ at membrane channels, reduces smooth muscle contractility and vascular tone
- Mg-ATP complex formation - cofactor for >300 enzymatic reactions including Na+/K+-ATPase
- Neuromuscular junction - inhibits presynaptic Ca2+ channels that trigger acetylcholine release; reduces postjunctional membrane excitability
- Cardiac membrane stabilization - slows SA node impulse formation and prolongs AV conduction
Normal serum level: 1.8-2.5 mg/dL (1.5-2.1 mEq/L)
1 gram of MgSO4 = ~4 mmol = 8 mEq = 98 mg elemental magnesium.
2. Clinical Indications in Anesthesia and ICU
A. Obstetric Anesthesia - Preeclampsia and Eclampsia
This is the most established indication. MgSO4 is the cornerstone treatment for seizure prophylaxis and treatment in preeclampsia/eclampsia.
Dosing:
- IV route: 4-6 g loading dose over 15-20 min + 1-2 g/hr continuous infusion
- IM route (Pritchard regimen): 4-5 g IM, repeated every 4 hours
Anesthetic implications:
-
MgSO4 profoundly potentiates nondepolarizing neuromuscular blocking drugs (NMBDs). After a 40 mg/kg MgSO4 dose, the ED50 of vecuronium is reduced by 25%, onset time is nearly halved, and recovery time nearly doubled
-
Neostigmine-induced reversal is attenuated in patients on magnesium
-
The mechanism involves dual action: prejunctional - blocks Ca2+ channels at nerve terminals reducing ACh release; postjunctional - decreases membrane excitability
-
Succinylcholine interaction is controversial - some reports suggest antagonism of succinylcholine block; prolonged weakness can also occur
-
Sugammadex is preferred over neostigmine for reversal in patients receiving MgSO4, given attenuated neostigmine response
-
Objective neuromuscular monitoring is mandatory - dose NMBDs carefully; do not rely on clinical assessment alone
-
The combination of MgSO4 with calcium channel blockers (especially nifedipine) can produce excessive neuromuscular blockade and severe hypotension
-
Miller's Anesthesia 10e, p. 3310-3311; Barash Clinical Anesthesia 9e, block 14, 19
B. Multimodal Analgesia (NMDA Antagonism)
Magnesium is an increasingly used adjunct for perioperative pain management, leveraging its NMDA receptor antagonism to suppress central sensitization.
Evidence (from Barash 9e, block 19):
"Recent meta-analyses indicate that the perioperative administration of IV magnesium may also be an effective adjunct in the treatment of perioperative pain. IV magnesium infusion decreases pain scores, is opioid sparing in the first 24 hours following surgery and is devoid of any serious adverse effects."
- The combination of MgSO4 + low-dose ketamine has shown additive benefit in spinal surgery: magnesium bolus 50 mg/kg + maintenance 8 mg/kg/hr reduced postoperative morphine consumption and improved sleep/satisfaction scores
- Particularly useful in opioid-tolerant patients by suppressing neuropathic pain and central sensitization
- Recent meta-analyses (PMID 38848810, 2024) confirm analgesic efficacy and opioid-sparing effects in general abdominal surgery
Dosing for analgesia:
- Loading dose: 30-50 mg/kg IV
- Maintenance: 6-20 mg/kg/hr
C. Antiarrhythmic Effects - Torsades de Pointes
Magnesium is the drug of choice for torsades de pointes (TdP) and digoxin-induced arrhythmias.
- Necessary for transport of Na+, Ca2+, and K+ across cell membranes
- Slows SA node impulse formation and prolongs conduction through myocardial tissue
- Intravenous formulation required - oral magnesium has no role in acute arrhythmia management
Dosing for TdP:
- Pulseless: 1-2 g IV over 5-20 minutes
- With pulse: 1-2 g IV over 5-60 minutes
For congenital Long QT - TdP during general anesthesia, Miller's Anesthesia recommends: stop volatile anesthesia (switch to TIVA), then administer magnesium sulfate 25-50 mg/kg over 2-3 min as therapeutic treatment.
- Lippincott Pharmacology, block 2; Braunwald's Heart Disease, block 8
D. Bronchospasm / Severe Asthma / COPD Exacerbation
Magnesium acts as a bronchodilator through:
- Inhibiting release of bronchoconstrictors (histamine and acetylcholine)
- Calcium antagonism - relaxes bronchial smooth muscle
- Anti-inflammatory properties
In the ICU setting (Fischer's Mastery of Surgery, 8e), maintaining magnesium >2.5 mEq/L is recommended in patients with acute bronchospasm, as this appears helpful without inducing hypotonia or cardiac dysrhythmia. A recent network meta-analysis (PMID 40637351, 2025) confirms IV magnesium's role among bronchodilators in pediatric critical asthma.
Dosing for asthma/COPD exacerbation: 2 g IV over 30-60 minutes
E. Pheochromocytoma Resection
An important but less commonly discussed indication:
- MgSO4 causes vascular smooth muscle relaxation with arteriolar vasodilation
- Directly inhibits catecholamine release from the adrenal medulla
- Used perioperatively to blunt hypertensive crises and hemodynamic surges during tumor manipulation
Dosing:
-
40-60 mg/kg loading dose prior to intubation + 1-2 g/hr maintenance infusion
-
Barash Clinical Anesthesia 9e, block 5
F. Emergence Agitation
Recent meta-analysis (PMID 38749290, 2024) demonstrates that MgSO4 reduces emergence agitation in surgical adults undergoing general anesthesia. Mechanism likely involves NMDA antagonism reducing excitatory neurotransmission during the emergence phase.
Similarly, MgSO4 reduces laryngospasm in pediatric patients (PMID 39089452, 2024) - likely through relaxation of laryngeal musculature and reduced airway irritability.
G. Uterine Relaxation (Tocolysis)
- Used as a tocolytic for preterm labor
- Loading dose: 6 g IV + maintenance: 2 g/hr
- Also used for uterine relaxation during ex utero intrapartum treatment (EXIT) procedures and open fetal surgery - a magnesium sulfate bolus can be given upfront at uterine closure to reduce tone and improve operative field
H. Neuroprotection in Obstetrics
- Fetal and neonatal neuroprotection in premature births
- Can exacerbate hypotension and potentiate NMB in this context - requires careful monitoring
3. Hypomagnesemia in the ICU
Hypomagnesemia is alarmingly common in the critically ill.
| Serum Mg (mg/dL) | mEq/L | Presentation |
|---|---|---|
| < 1.2 | < 1.0 | Tetanic seizures, arrhythmias |
| 1.2 - 1.8 | 1.0 - 1.5 | Neuromuscular irritability, hypocalcemia, hypokalemia |
| 1.8 - 2.5 | 1.5 - 2.1 | Normal range |
| 2.5 - 5.0 | 2.1 - 4.2 | Asymptomatic (therapeutic) |
| 5 - 7 | 4.2 - 5.8 | Flushing, N/V, lethargy, decreased DTR |
| 7 - 12 | 5.8 - 10 | Loss of DTR, respiratory depression, heart block |
| > 12 | > 10 | Cardiac arrest |
Incidence: ~10% in general hospitalized patients; up to 65% in the critically ill
ICU causes of hypomagnesemia:
- Nasogastric suctioning, diarrhea, vomiting, high-output fistulae
- Diuretic use (loop and thiazide)
- Chronic PPI use (inhibits TRPM6/7 channels reducing Mg2+ GI absorption)
- Chronic alcohol dependence (multifactorial: renal wasting + GI losses + reduced PTH)
- Pancreatitis, short bowel syndrome
Treatment of severe hypomagnesemia (<1.2 mg/dL):
- 1-2 g/hr IV over 3-6 hours, then 0.5-1 g/hr as needed
Refractory hypocalcemia and hypokalemia that fail to correct should trigger a check for hypomagnesemia - magnesium must be repleted first.
4. Hypermagnesemia and Toxicity
The classic toxicity progression is:
| Level | Sign |
|---|---|
| >5 mg/dL (>4.2 mEq/L) | Flushing, nausea, drowsiness |
| Loss of deep tendon reflexes (DTR) | First clinical sign of toxicity - monitor this! |
| 7-12 mg/dL | Respiratory muscle paralysis |
| >12 mg/dL | Cardiac arrest |
Antidote: 10% calcium gluconate (or calcium chloride) 1 g IV - directly antagonizes magnesium at voltage-gated channels.
Monitoring during MgSO4 infusion (especially in preeclampsia):
- Check DTRs regularly (loss = first sign of toxicity)
- Urine output >25-30 mL/hr (magnesium is renally cleared)
- Respiratory rate >12/min
- Serum levels every 4-6 hours if high-dose infusion
5. Neuromuscular Blocking Drug Interactions - Summary
| Drug | Interaction |
|---|---|
| All nondepolarizing NMBDs | Potentiated - reduce dose, titrate carefully with objective monitoring |
| Succinylcholine | Controversial - may be antagonized OR prolonged |
| Neostigmine reversal | Attenuated - sugammadex preferred |
| Aminoglycosides | Additive NMJ blockade - increased risk of prolonged paralysis |
| Calcium channel blockers (nifedipine) | Risk of severe hypotension + NMB potentiation |
6. Regional Anesthesia Adjuvant
Perineural magnesium extends the duration of peripheral nerve blocks:
- Dosing: 150-600 mg MgSO4 added to the primary local anesthetic
- Mechanism: NMDA receptor antagonism at the dorsal horn level
7. Dosing Reference Summary
(From Barash Clinical Anesthesia 9e, Table 16-27)
| Indication | Dose |
|---|---|
| Multimodal analgesia | 30-50 mg/kg load + 6-20 mg/kg/hr |
| Perineural adjuvant | 150-600 mg + local anesthetic |
| Preeclampsia/eclampsia | 4-6 g IV load + 1-2 g/hr (IV); or 4-5 g IM q4h |
| Tocolysis | 6 g IV load + 2 g/hr |
| Torsades de pointes (pulseless) | 1-2 g IV over 5-20 min |
| Torsades de pointes (with pulse) | 1-2 g IV over 5-60 min |
| Pheochromocytoma | 40-60 mg/kg load + 1-2 g/hr |
| Asthma/COPD exacerbation | 2 g IV over 30-60 min |
| Severe hypomagnesemia (<1.2 mg/dL) | 1-2 g/hr over 3-6 hrs |
Recent Evidence (2024-2026)
- PMID 38848810 (2024, Systematic Review): Perioperative IV magnesium in abdominal surgery reduces pain and opioid consumption in the first 24 hours
- PMID 38749290 (2024, Meta-Analysis): IV MgSO4 reduces emergence agitation in adult general anesthesia patients
- PMID 39089452 (2024, Meta-Analysis): MgSO4 reduces laryngospasm incidence in pediatric general anesthesia
- PMID 40606621 (2025, Systematic Review): IV MgSO4 effective in spinal surgery for analgesia and hemodynamic stability
- PMID 40637351 (2025, Network Meta-Analysis): IV magnesium ranks highly among bronchodilators in pediatric critical asthma
Key Teaching Points:
- Magnesium potentiates ALL nondepolarizing NMBDs - always use objective monitoring and reduced doses
- The first clinical sign of toxicity is loss of DTR - monitor before checking levels
- Hypomagnesemia is present in up to 65% of ICU patients - check and correct before troubleshooting refractory hypocalcemia/hypokalemia
- Sugammadex is preferred over neostigmine for reversal in patients on magnesium infusions
- Magnesium is the drug of first choice for torsades de pointes - IV only
Sources: Miller's Anesthesia 10e; Barash Clinical Anesthesia 9e; Lippincott Illustrated Reviews Pharmacology; Fischer's Mastery of Surgery 8e; Creasy & Resnik's Maternal-Fetal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.