Tell me about primary open angle glaucoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"primary open-angle glaucoma"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have thorough information from three authoritative sources. Here is the full response:
Primary Open-Angle Glaucoma (POAG)
Definition
Primary open-angle glaucoma is a chronic, progressive optic neuropathy of adult onset, defined by all of the following:
- Retinal nerve fibre layer (RNFL) thinning
- Glaucomatous optic nerve damage
- Characteristic visual field loss as damage progresses
- An open anterior chamber angle on gonioscopy
- No identifiable secondary cause or non-glaucomatous explanation for the optic neuropathy
IOP is the key modifiable risk factor, but POAG can occur at normal IOP levels (see normal-tension glaucoma).
- Kanski's Clinical Ophthalmology, p. 364
Epidemiology
POAG is the most prevalent type of glaucoma in people of European and African descent. In those older than 70 years:
- ~6% prevalence in White populations
- ~16% in Black populations (also earlier onset, often harder to control)
- ~3% in Asian populations
- Affects both sexes equally
- Kanski's Clinical Ophthalmology, p. 364
Risk Factors
| Risk Factor | Notes |
|---|---|
| Elevated IOP | Higher IOP = greater glaucoma risk; asymmetry ≥4 mmHg also significant |
| Age | More common with advancing age |
| Race | ~4x more common in Black individuals, earlier onset |
| Family history | ~4x risk for siblings; ~2x risk for offspring |
| Myopia | Associated with increased incidence; myopic eyes may be more susceptible |
| Large optic disc | Larger discs are more vulnerable |
| Low ocular perfusion pressure | Difference between arterial BP and IOP; low OPP raises risk |
| Translaminar pressure gradient | IOP minus orbital CSF pressure; implicated in lamina cribrosa deformation |
| Anti-VEGF therapy | Repeated injections (especially bevacizumab) can cause sustained IOP elevation |
| Calcium-channel blockers (monotherapy) | Meta-analyses show higher glaucoma prevalence |
| Vascular disease | Systemic hypertension, cardiovascular disease, vasospasm (migraine) |
- Kanski's Clinical Ophthalmology, p. 364-365
Genetics
POAG has been associated with at least 127 genomic loci (Nature Communications, 2021). Key genes:
- MYOC (myocilin): found in the trabecular meshwork; multiple causative mutations described
- OPTN (optineurin): broadly accepted as causative
A polygenic risk score (PRS) now exists that can predict susceptibility and risk of advanced disease, potentially enabling personalised surveillance strategies.
If a single family member develops glaucoma before age 35, the probability of a MYOC mutation may be as high as 33%.
- Kanski's Clinical Ophthalmology, p. 365
Pathogenesis of Glaucomatous Optic Neuropathy
Retinal ganglion cell (RGC) death in POAG occurs predominantly via apoptosis (not necrosis). The preterminal event involves calcium ion influx and increased intracellular nitric oxide. Glutamine metabolism is intrinsically involved. Downstream effects include astrocyte/glial proliferation and remodelling of the lamina cribrosa extracellular matrix.
Two main injury mechanisms are proposed (they are not mutually exclusive):
- Mechanical - direct damage to RGC axons as they traverse the lamina cribrosa under elevated IOP
- Ischaemic - compression of optic nerve head blood supply; linked to low ocular perfusion pressure
Both pathways converge on:
- Reduced axoplasmic flow
- Nutrient deprivation / metabolic waste accumulation
- Loss of neurotrophic factors
- Oxidative injury
- Immune-mediated damage
- Kanski's Clinical Ophthalmology, p. 365
Clinical Features
Symptoms
POAG is classically asymptomatic until late stages. Peripheral visual fields are lost well before the patient notices functional impairment. When symptoms do occur: difficulty reading, reduced contrast sensitivity, glare, or peripheral visual field defects. Central visual loss is a late finding.
- The Wills Eye Manual, p. 547; Goldman-Cecil Medicine, p. 4131
Signs
1. Intraocular Pressure
Normal range is 10-21 mmHg. However, nearly half of POAG patients have an IOP of ≤21 mmHg at any single screening - IOP alone cannot rule in or rule out the diagnosis.
2. Gonioscopy
Normal-appearing, open anterior chamber angle. No peripheral anterior synechiae (PAS). This finding distinguishes POAG from angle-closure glaucoma.
3. Optic Nerve
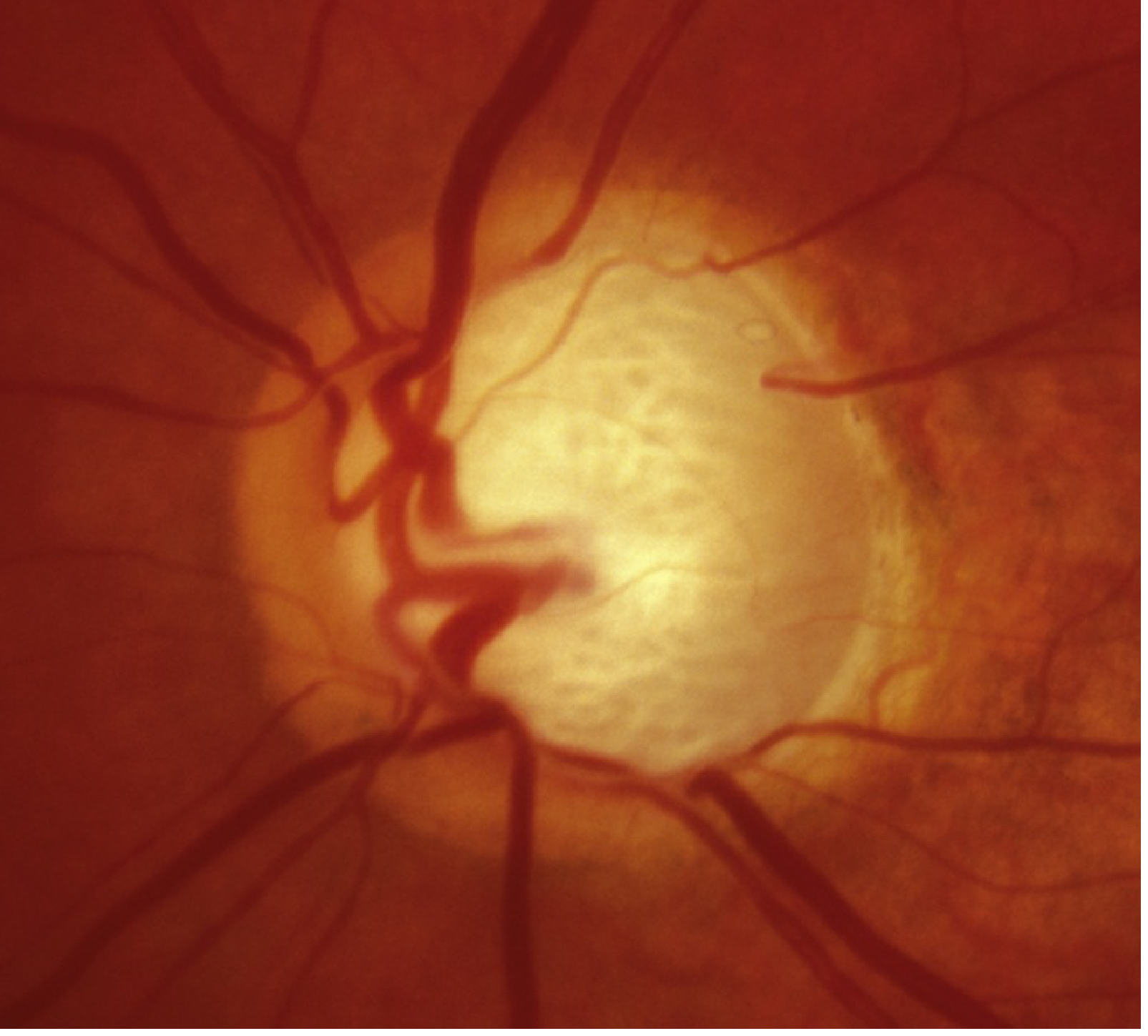
Advanced POAG optic nerve cupping (Wills Eye Manual, Fig. 9.1.1)
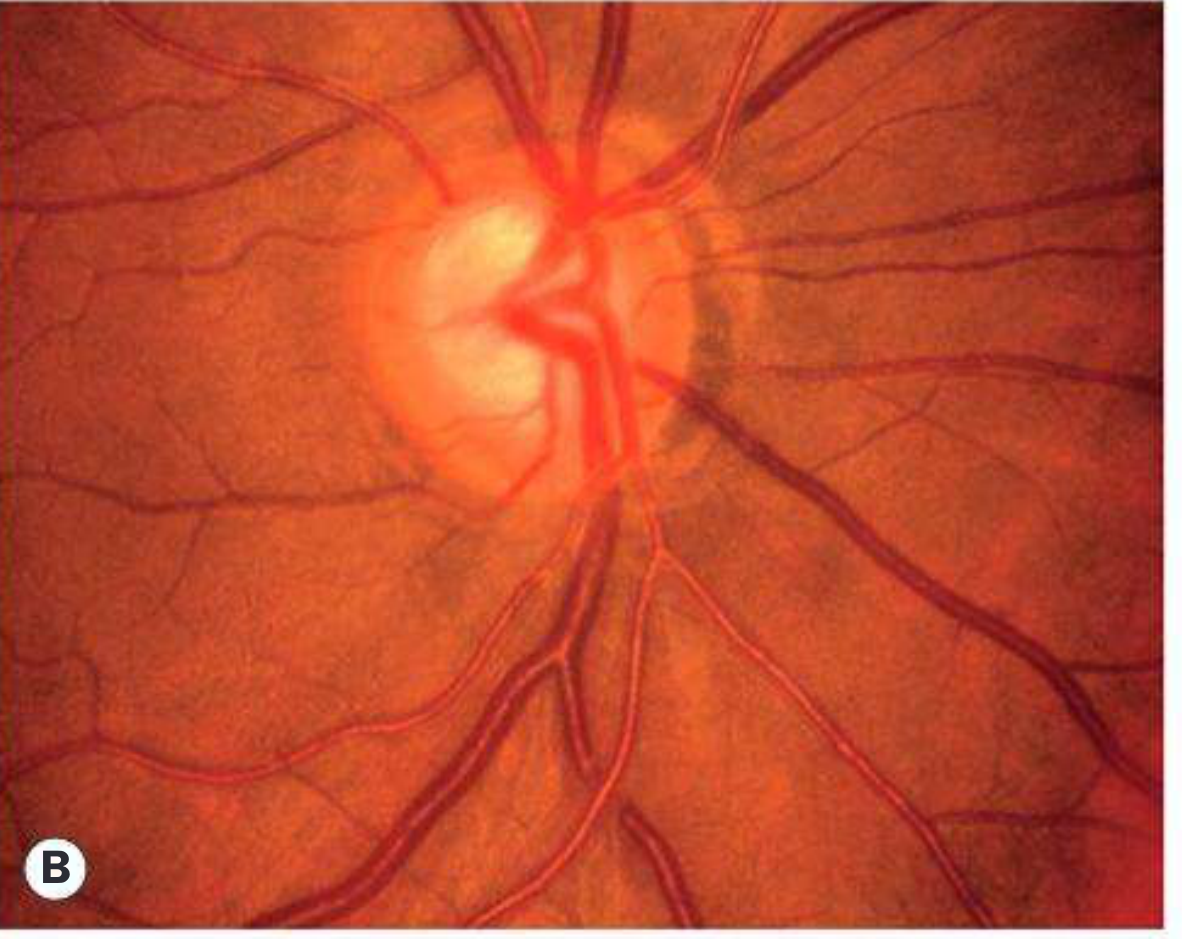
Progressive glaucomatous cupping - same disc 2 years apart (Kanski's, Fig. 11.8B)
Characteristic optic nerve findings include:
- Loss of neuroretinal rim tissue (notching), most commonly inferior > superior
- Progressive cup enlargement (C/D ratio >0.6 is less specific on its own)
- C/D asymmetry >0.2 between eyes (without another explanation)
- Splinter/disc hemorrhage crossing the disc margin (Drance hemorrhage)
- Bayoneting of vessels at the disc margin
- RNFL defects
- Acquired optic disc pit
- Beta-zone peripapillary atrophy
4. Visual Fields
Classic patterns (defects typically respect the horizontal midline):
- Nasal step
- Paracentral scotoma
- Arcuate scotoma (extending from blind spot nasally)
- Altitudinal defect
- Generalised depression
- The Wills Eye Manual, p. 547-549
Diagnosis
Diagnosis requires correlation of IOP, optic nerve appearance, and visual field testing. Automated perimetry (Humphrey visual field) is the standard for detecting and monitoring field loss.
The Early Manifest Glaucoma Trial (EMGT) provides key natural history data: in untreated high-tension glaucoma, the mean rate of visual field progression is -1.31 dB/year; pseudoexfoliation glaucoma progresses fastest at -3.13 dB/year; and normal-tension glaucoma slowest at -0.36 dB/year. On average, untreated glaucoma progresses from normal to blindness over approximately 25 years.
- Kanski's Clinical Ophthalmology, p. 363
Differential Diagnosis
- Ocular hypertension - elevated IOP, normal disc and fields
- Physiologic cupping - large static C/D, no notching or field loss, normal IOP, large disc
- Secondary open-angle glaucoma - identifiable cause (pigmentary, exfoliative, steroid-induced, uveitic, angle recession, etc.)
- Normal-tension glaucoma - same as POAG but IOP always ≤21 mmHg
- Optic atrophy - disproportionate pallor > cupping; visual field respects vertical midline if chiasmal/retrochiasmal
- The Wills Eye Manual, p. 549-550
Treatment
The treatment goal is to lower IOP to a target level that slows or halts progression. IOP reduction of 20-30% from baseline is the typical starting target, adjusted based on disease severity and progression.
1. Topical Pharmacotherapy (First-line)
| Drug Class | Agent | Mechanism | Dosing |
|---|---|---|---|
| Prostaglandin analogues | Latanoprost 0.005%, travoprost 0.004%, bimatoprost | Increase uveoscleral outflow | Once daily (evening) |
| Beta-blockers | Timolol 0.5% | Decrease aqueous production | Twice daily |
| Alpha-2 agonists | Brimonidine 0.1-0.2% | Decrease aqueous production + increase uveoscleral outflow | Three times daily |
| Topical CAIs | Dorzolamide, brinzolamide | Decrease aqueous production | Two to three times daily |
| Rho-kinase inhibitors | Netarsudil 0.02% | Increase trabecular outflow | Once daily |
| Miotics | Pilocarpine 1-4% | Increase trabecular outflow | Two to four times daily (rarely used) |
| Sympathomimetics | Dipivefrin 0.1% | Decrease production + increase outflow | Twice daily (rarely used) |
Tip: Patients should occlude the punctum for 10 seconds (or keep eyelids closed 1-2 minutes) after instillation to reduce systemic absorption.
2. Systemic CAIs (for refractory cases)
- Acetazolamide 125-250 mg orally 2-4 times daily, or 500 mg sequel twice daily
- Methazolamide 25-50 mg twice to three times daily
- IV acetazolamide 250-500 mg for urgent IOP reduction
- Monitor potassium if on other diuretics or digoxin. Rare but severe risks: aplastic anaemia, Stevens-Johnson syndrome.
3. Laser Procedures
- Selective Laser Trabeculoplasty (SLT): Lower energy than argon laser trabeculoplasty (ALT), causes less tissue damage, repeatable. IOP-lowering effect equivalent to ALT. Can be considered first-line therapy - evidence shows it can maintain normal IOP without medications.
- Argon Laser Trabeculoplasty (ALT): Initial success rate 70-80%, dropping to ~50% at 2-5 years. Not repeatable.
4. Surgery (for resistant or advanced cases)
- Trabeculectomy: Creates a fistula between the anterior chamber and episcleral tissue; adjunctive antimetabolites (mitomycin C, 5-fluorouracil) improve efficacy but increase complication risk (bleb leaks, hypotony)
- Tube-shunt implantation: Implants a synthetic filtration device from the anterior chamber into an orbital reservoir - used when trabeculectomy is likely to fail (e.g., prior conjunctival scarring)
- Minimally Invasive Glaucoma Surgery (MIGS): A growing category of trabecular bypass and suprachoroidal procedures
- Goldman-Cecil Medicine, p. 4132; The Wills Eye Manual, p. 555-559
Monitoring and Follow-up
- Re-examine 4-6 weeks after starting a new beta-blocker, prostaglandin, or after SLT/ALT to assess efficacy
- Topical CAIs and alpha-agonists reach steady state more quickly - repeat IOP check can be done at any time
- Roughly 1 in 8 eyes with glaucoma under routine care show a mean deviation (MD) change of >1 dB/year; central 10° field deterioration is equally important to track
- The Wills Eye Manual, p. 559; Kanski's Clinical Ophthalmology, p. 363
Key Takeaways
- POAG is the most common glaucoma type; it is bilateral, chronic, progressive, and largely asymptomatic until late
- IOP is modifiable but not the sole determinant - optic nerve appearance and visual fields are diagnostic anchors
- Prostaglandin analogues are generally first-line topical therapy; SLT can be offered as a first-line alternative
- Treatment is typically lifelong; target IOP is individualised based on disease severity and rate of progression
- Early detection via routine ophthalmological screening remains the most effective strategy to prevent blindness
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed., pp. 363-368
- The Wills Eye Manual, 8th Ed., pp. 547-559
- Goldman-Cecil Medicine, International Edition, pp. 4131-4132
This is a shared conversation. Sign in to Orris to start your own chat.