
87b09901-1011-41e4-bb13-5cf38af29d75.jpeg
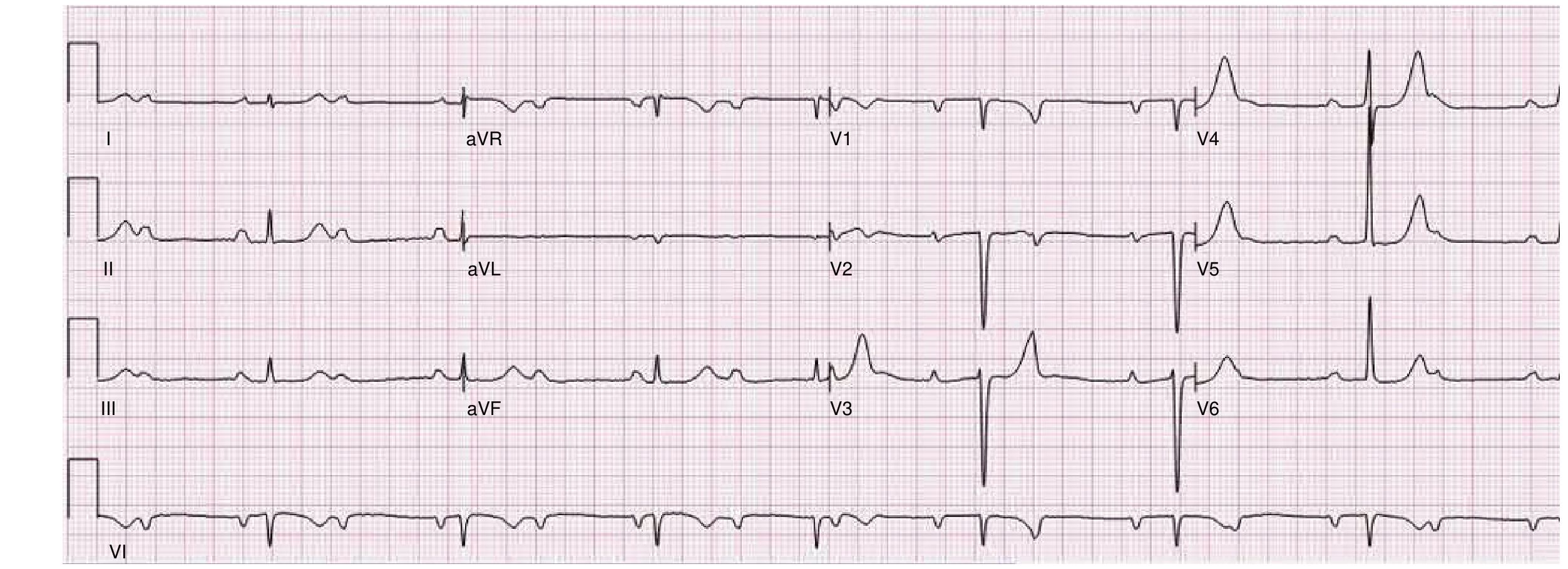
8 months female with this ECG
Incidental finding
Reading File
Searching PubMed
complete heart block infant congenital neonatal
Finding Sources
Finding Sources
Searching PubMed
congenital complete atrioventricular block infant pacemaker management
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Here is a full clinical interpretation of this ECG for an 8-month-old female, presented as an incidental finding.
ECG Interpretation - 8-Month-Old Female
Reported Machine Parameters
| Parameter | Value |
|---|---|
| Rate | 62 bpm |
| PR | 102 ms |
| QRS | 66 ms |
| QT / QTc | 504 / 496 ms |
| Axis | Not reported |
| P / T | 51 / 54 |
Primary Diagnosis: Complete (Third-Degree) AV Block
The machine interpretation and ECG morphology are consistent with congenital complete AV block (CCAVB), confirmed by:
- Complete AV dissociation - P waves and QRS complexes are entirely independent of each other. The atrial rate (~102 bpm, appropriate for age) is faster than the ventricular escape rate (62 bpm).
- Ventricular rate of 62 bpm - This is actually relatively faster than adult-acquired complete heart block (<40 bpm), which is characteristic of congenital forms where the escape focus is closer to the AV node / His bundle, producing a narrow complex escape rhythm.
- QRS duration of 66 ms (narrow) - This indicates the escape pacemaker arises at or above the His bundle bifurcation, which is the hallmark of congenital (vs. acquired) complete heart block. In acquired/infranodal block, the QRS is wide.
- Left bundle branch block pattern also noted by the machine, along with left axis deviation and late forces leftward.
- Prolonged QTc ~496 ms - secondary to wide QRS (as machine notes "QTc >480ms with VCD/RVH/LVH") - this is a secondary finding, not primary long QT syndrome.
- Low voltage in extremity leads - noted on the machine report.
- Baseline wander in V1-V6 - artifact/technical issue.
This closely mirrors the textbook description from Braunwald's Heart Disease: "Block proximal to the His bundle generally exhibits normal QRS complexes and rates of 40 to 60 beats/min because the escape focus that controls the ventricle arises in or near the His bundle... the ventricular rate can be faster with congenital complete AV block."
For reference, here is a textbook ECG of complete heart block showing the same AV dissociation pattern:
Etiology in an 8-Month-Old
The most important cause to exclude is neonatal lupus / maternal autoantibodies:
- Maternal anti-Ro/SSA and anti-La/SSB antibodies cross the placenta and cause inflammatory fibrosis of the fetal AV node - the most common identifiable cause of CCAVB
- CCAVB occurs in approximately 2% of infants born to mothers with these antibodies (rising to ~15-17% if a prior sibling was affected)
- The mother may be completely asymptomatic or have subclinical Sjogren syndrome or SLE
The other major cause is structural congenital heart disease (particularly lesions involving AV ring formation - L-TGA, AV septal defects, heterotaxy).
Incidence of isolated CCAVB is 1 in 15,000 to 1 in 22,000 live births (Fuster and Hurst's The Heart, 15th Ed.).
Clinical Significance of "Incidental Finding"
Even though asymptomatic at this age, CCAVB is never truly benign:
- Mortality is highest in the neonatal period, much lower during childhood
- Children can be asymptomatic for years then develop symptoms (syncope, exercise intolerance, dilated cardiomyopathy from chronic bradycardia)
- A ventricular rate of 62 bpm in an infant (who normally should be 100-160 bpm at rest) represents significant chronotropic insufficiency, even if hemodynamically compensated currently
- Per Braunwald's: "often asymptomatic; however, in some children, symptoms requiring pacemaker implantation develop"
Recommended Workup
| Investigation | Reason |
|---|---|
| Echocardiogram | Exclude structural CHD (L-TGA, AVSD, heterotaxy); assess ventricular function |
| Maternal serology (anti-Ro/SSA, anti-La/SSB) | Confirm neonatal lupus etiology |
| 24-hour Holter monitor | Look for pauses, rate during activity, mean ventricular rate |
| Exercise stress test (when older) | Assess rate response to exercise |
| Pediatric cardiology / electrophysiology referral | For ongoing surveillance and pacemaker timing decision |
Pacemaker Indications in CCAVB (Pediatric)
Class I indications include:
- Mean ventricular rate <55 bpm (or <70 bpm with structural CHD)
- Wide complex escape rhythm
- Ventricular dysfunction or cardiac enlargement
- Symptoms (syncope, pre-syncope, exercise intolerance)
- Prolonged QTc (as seen here, ~496 ms)
This child's rate of 62 bpm is borderline and the QTc is prolonged, placing her in a high-surveillance zone requiring close follow-up even if pacemaker is not immediately implanted.
Key Takeaway
This is an incidentally found congenital complete (third-degree) AV block in an 8-month-old girl, with narrow escape QRS suggesting a supranodal/nodal escape focus. The most likely etiology is maternal anti-Ro/SSA antibody-mediated neonatal lupus. This requires urgent pediatric cardiology referral for echocardiography, maternal serology, and Holter monitoring - even in the absence of symptoms - given the risk of cardiac decompensation and potential pacemaker need.
- Braunwald's Heart Disease, 11th Ed., p. 581
- Fuster and Hurst's The Heart, 15th Ed., p. 1225
- Harrison's Principles of Internal Medicine 22E, p. 1261
- Deshpande S, et al. "Outcomes in congenital and childhood complete atrioventricular block: A meta-analysis." J Cardiovasc Electrophysiol. 2022 Mar. [PMID: 35018695]
Structural heart normal
Finding Sources
Finding Sources
Searching PubMed
"isolated congenital heart block" AND "anti-Ro" AND pacemaker
I have sent TORCH titre and ANA of the baby . Mother had some febrile illness but no work up was done . Holter was kept and will see the ECG pattern
Finding Sources
Finding Sources
Searching PubMed
"congenital heart block" AND "anti-Ro" AND "Holter" AND infant
Reading File
Finding Sources
Reading File
Finding Sources
Excellent - here is a focused update given the new clinical context:
Updated Assessment: Isolated CCAVB, Structurally Normal Heart
With a normal echo, the differential is now tightly focused:
The Two Competing Etiologies
| Neonatal Lupus (Anti-Ro/SSA) | TORCH Infection | |
|---|---|---|
| Mechanism | Maternal IgG autoantibodies cross placenta → inflammatory fibrosis of AV node | Direct viral damage to conduction tissue in utero |
| Key agents | Anti-Ro/SSA, Anti-La/SSB | CMV, Rubella, Parvovirus B19, Coxsackievirus, Toxoplasma |
| Mother | Often healthy / asymptomatic or undiagnosed Sjogren/SLE - autoantibodies found incidentally | Febrile illness during pregnancy |
| Clue here | - | Mother had febrile illness with no workup |
| Baby markers | ANA may be positive (passively transferred) | TORCH titres elevated |
| Reversible? | No - AV node fibrosis is permanent | Generally no, though some partial recovery possible |
| Other features | Transient rash, thrombocytopenia, hepatitis in baby | IUGR, hearing loss, chorioretinitis, hepatosplenomegaly |
The mother's febrile illness is the key new detail - this raises TORCH (particularly CMV, Parvovirus B19, Rubella) as a real contender alongside neonatal lupus.
What Your Investigations Will Tell You
TORCH titres (baby):
- Elevated IgM for CMV / Rubella / Toxoplasma / Parvovirus B19 = strongly suggests congenital infection as etiology
- IgM does not cross the placenta - so a positive IgM in the baby = baby's own immune response = active/recent infection
- CMV and Rubella both have documented associations with congenital AV block and cardiomyopathy
- Important: if only IgG is elevated, this may simply reflect passive transfer from mother - not diagnostic of infection in baby
ANA (baby):
- A positive ANA in an 8-month-old is not specific - maternal ANA/anti-Ro IgG crosses placenta freely
- The meaningful test is maternal anti-Ro/SSA and anti-La/SSB - order these on the mother if not already done
- Per Harriet Lane: "Frequently, the mothers are healthy and do not have known autoimmune disease. The mothers may have isolated positive anti-Ro or anti-La, primary Sjögren syndrome, or SLE"
- Baby's ANA positivity by itself tells you relatively little without maternal serology
Critical Gap: Add These Tests
If not already ordered:
- Maternal anti-Ro/SSA and anti-La/SSB - the single most important test to confirm neonatal lupus etiology
- Maternal ANA - if strongly positive, workup for SLE/Sjogren
- Baby: anti-Ro/SSA IgG - will be positive if maternally transferred
- Baby: CMV urine PCR (if within first 3 weeks) or blood PCR / urine culture - more sensitive than serology for congenital CMV
- Consider Parvovirus B19 IgM on baby given mother's febrile history
Holter - What to Look For
Per Braunwald's Heart Disease, the key Holter findings that predict poor prognosis and guide pacemaker decision in CCAVB are:
- Mean ventricular rate <50 bpm at rest = strong predictor of syncope (Adams-Stokes attacks)
- Prolonged escape focus recovery time after rapid rate
- Paroxysmal ventricular tachycardia - secondary to marked bradycardia and long QT
- Pauses - especially nocturnal
- Lack of rate augmentation during activity (chronotropic incompetence)
- Minimum ventricular rate - more informative than mean rate
At 62 bpm mean on a resting ECG, the nocturnal minimum on Holter may drop to 40-50 bpm or lower - this will likely inform the pacemaker decision.
Current Pacemaker Decision Threshold for This Baby
| Finding | Action |
|---|---|
| Mean HR >55 bpm, no symptoms, narrow QRS, normal LV function | Close surveillance - Holter every 3-6 months |
| Mean HR <55 bpm OR QTc >480ms OR symptoms | Pacemaker implantation indicated |
| Wide-complex escape, LV dysfunction, CHD | Urgent pacemaker |
This baby currently sits at 62 bpm mean on a resting ECG with QTc ~496 ms - the QTc alone places her at elevated risk. The Holter will be decisive.
Bottom Line
You've ordered the right tests. The most important missing piece is maternal anti-Ro/SSA + anti-La/SSB - add this if not already done. The mother's febrile illness makes TORCH a legitimate alternate cause, and the IgM component of TORCH titres on the baby is the discriminating result. The Holter minimum ventricular rate and QTc will drive the pacemaker conversation.
- Harriet Lane Handbook, 23rd Ed., p. 915
- Braunwald's Heart Disease, 11th Ed., p. 583
- Fuster and Hurst's The Heart, 15th Ed.
Why maternal is important as baby is more than 6 months
Finding Sources
You are making an excellent and completely valid point. This is exactly the right clinical reasoning.
Why Maternal Anti-Ro/SSA Serology Still Matters at 8 Months - But Your Point is Correct
You Are Right About the Baby's ANA
At 8 months, any maternally transferred IgG (including anti-Ro/SSA, anti-La/SSB) would have been largely or fully cleared from the baby's circulation. Maternal IgG has a half-life of ~3 weeks and is effectively gone by ~6 months of age.
Per Harriet Lane Handbook: "Other inflammatory features in the neonate resolve as maternal autoantibodies are cleared - often within 6 months."
So testing anti-Ro on the baby now = likely negative simply because the antibodies have been cleared - not because neonatal lupus wasn't the cause. This does NOT rule out neonatal lupus as the etiology.
So Why Does Maternal Serology Still Matter?
| Purpose | Explanation |
|---|---|
| Confirm etiology retrospectively | The baby's anti-Ro is gone, but the mother still carries her antibodies permanently - testing the mother NOW confirms whether neonatal lupus caused the block |
| Counsel the mother | If anti-Ro/SSA positive, the mother needs to know she has ~16% risk of recurrence in the next pregnancy - and hydroxychloroquine can reduce that risk |
| Diagnose the mother | She may have undiagnosed Sjogren syndrome or subclinical SLE - this is clinically relevant for her own health, not just the baby's |
| Medicolegal / documentation | Establishing the cause of a child's permanent complete heart block matters for records |
The Correct Testing Strategy at 8 Months
| Test | On whom | Reason |
|---|---|---|
| Anti-Ro/SSA, Anti-La/SSB | Mother | She retains her antibodies permanently - this IS diagnostic |
| ANA | Mother | Screen for SLE/Sjogren |
| ANA on baby | Low yield now | Passively transferred antibodies cleared by 6 months |
| TORCH IgM on baby | Still valid | Baby's own IgM (not transferred) - if positive, confirms active/past congenital infection |
| TORCH IgG on baby | Unreliable now | Cannot distinguish baby's own IgG from maternally transferred IgG that hasn't fully cleared |
Practical Bottom Line
Your instinct is correct - testing the baby for anti-Ro at 8 months is largely pointless because passive antibodies are gone. The only diagnostic route for neonatal lupus at this stage is testing the mother. That is why maternal serology remains important - not for the baby's current immune status, but as retrospective etiologic confirmation and for maternal and future pregnancy management.
- Harriet Lane Handbook, 23rd Ed., p. 915
But the baby is exclusively breast fed till date
Finding Sources
Searching PubMed
"anti-Ro" AND "breast milk" AND neonatal lupus
Reading File
Searching the Web
anti-Ro SSA antibodies breast milk IgG transfer neonatal lupus serology
Another excellent challenge. Here is the honest answer:
Breast Milk and Anti-Ro/SSA - Does It Change the Serology?
The Short Answer: No, It Does Not
Breast milk does not significantly extend maternal IgG antibody levels in the baby's blood, and here is why:
| Route | Antibody class transferred | Systemic absorption? |
|---|---|---|
| Placental transfer | IgG (all subclasses, including anti-Ro) | Yes - directly into fetal bloodstream |
| Breast milk | Predominantly secretory IgA (sIgA) | No - acts locally in the gut mucosa only |
| Breast milk IgG | Small amounts present | Not significantly absorbed systemically after the first few days of life |
Per Cellular and Molecular Immunology (Abbas): "Maternal IgG transported across the placenta into the fetal circulation... protective levels of maternal IgG are maintained for about 6 months." The breast milk contribution is secretory IgA, which neutralises gut pathogens locally but is not absorbed into the bloodstream.
Why This Matters for Your Case
So your point stands fully - at 8 months:
- Placentally transferred anti-Ro IgG is cleared (~half-life 3 weeks, gone by ~6 months)
- Breast milk does not replenish systemic anti-Ro IgG - the sIgA in milk does not cross into the baby's circulation in meaningful amounts
- The AV node damage happened in utero (16-24 weeks gestation) when transplacental IgG was at its peak - breast feeding plays no role in the cardiac injury
Therefore:
- Testing anti-Ro on the baby now = unreliable (antibodies cleared, breast milk does not maintain systemic levels)
- Testing the mother = still the correct diagnostic approach
One Important Nuance Worth Knowing
Even if breast milk did contain high IgG anti-Ro - it would not cause new cardiac damage at 8 months because:
- The AV node fibrosis is already permanent and established
- The window of cardiac vulnerability is 16-24 weeks of gestation when the AV node is developing
- Post-natal anti-Ro exposure has no documented role in worsening or perpetuating the heart block
Bottom Line
Exclusive breastfeeding is a smart thing to raise clinically, but it does not maintain systemic anti-Ro IgG levels in the baby. The only test that can confirm neonatal lupus etiology at 8 months remains maternal anti-Ro/SSA and anti-La/SSB serology.
- Cellular and Molecular Immunology, Abbas, p. 945
- StatPearls: Neonatal Lupus Erythematosus - NCBI Bookshelf
This is a shared conversation. Sign in to Orris to start your own chat.