Choledocolethiasis 101
Reading File
Finding Sources
Finding Sources
Searching PubMed
choledocholithiasis management guidelines
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Now I have everything needed for a thorough, well-illustrated response.
Choledocholithiasis - A Complete Overview
Choledocholithiasis refers to the presence of stones within the extrahepatic common bile duct (CBD). It affects 5-20% of patients with cholelithiasis and is one of the most common indications for biliary endoscopy and surgery.
1. Classification: Primary vs. Secondary
| Type | Origin | Stone Composition | Common In |
|---|---|---|---|
| Secondary (most common in the West) | Gallbladder stones migrating through cystic duct | Cholesterol or black pigment | United States, Europe |
| Primary | De novo formation within the CBD | Soft brown pigment stones | Asia; post-sphincterotomy patients |
| Retained | Secondary stones found in CBD within 2 years post-cholecystectomy | Mixed | 1-2% of post-cholecystectomy cases |
Primary stone risk factors include IgA deficiency, chronic biliary infection, biliary dyskinesia, and prior sphincterotomy stenosis (allows duodenal reflux to seed stone formation).
- Clinical Gastrointestinal Endoscopy, 3e, p. 804
- Sabiston Textbook of Surgery, p. 1832
2. Presentation
Presentations span a wide spectrum:
Asymptomatic - CBD stones can be clinically silent or pass spontaneously; about 1/3 of incidentally found stones at cholecystectomy resolve on their own.
Biliary colic - Most common symptomatic presentation; intermittent obstruction causes fluctuating bilirubin and LFT abnormalities.
Obstructive jaundice - Painful jaundice (distinguishes it from malignant causes, which tend to be painless). Scleral icterus, dark urine, pale stools.
Ascending cholangitis - Bacterial infection behind an obstructing CBD stone:
- Charcot's triad: Fever/rigors + RUQ pain + Jaundice (42-75% have all three; 95% specific but only 26% sensitive)
- Reynolds' pentad: Charcot's triad + hypotension + altered mental status - indicates severe/suppurative cholangitis
- Bacteremia is found in 74% of patients - antibiotics should be started promptly on clinical suspicion
Gallstone pancreatitis - Second most common complication; CBD stones found in ~50% of patients with gallstone pancreatitis depending on timing of cholangiography.
Chronic/recurrent disease - Can lead to biliary strictures, secondary biliary cirrhosis, and cholangiocarcinoma (via chronic inflammation).
- Mulholland & Greenfield's Surgery, 7e, p. 3071
- Symptom to Diagnosis, 4e, p. 50
3. Diagnosis
Labs
LFTs alone are unreliable but informative:
| Finding | Sensitivity | Specificity | LR+ | LR- |
|---|---|---|---|---|
| Cholangitis | 11% | 99% | 18.3 | 0.93 |
| Jaundice | 36% | 97% | 10.1 | 0.69 |
| Dilated CBD on US | 42% | 96% | 6.9 | 0.77 |
| Elevated ALP | 57% | 86% | 2.6 | 0.65 |
| Elevated amylase | 11% | 95% | 1.5 | 0.99 |
Key points:
- Elevated bilirubin: 69% sensitive, 88% specific
- Normal LFTs have a 97% negative predictive value for CBD stones
- Elevated bilirubin + abnormal US = pretest probability approaches 90%
- Leukocytosis raises concern for cholangitis; lipase >3x ULN is diagnostic for pancreatitis
Imaging
| Modality | Sensitivity | Specificity | Notes |
|---|---|---|---|
| Transabdominal US | 22-60% | ~90% | Poor sensitivity, highly operator-dependent; gold standard for cholelithiasis but poor for CBD stones |
| CT | ~75% | - | Not test of choice; misses small/isodense stones |
| MRCP | 81-100% | 92-100% | Gold standard noninvasive test; 3D duct reconstruction; can miss stones <5 mm |
| EUS | 94-99% | 94-100% | Most sensitive test overall; same-session ERCP possible if positive; reduces ERCP need by 67% |
| ERCP | >90% | 99% | Now reserved as therapeutic, not diagnostic; pancreatitis in 1-5% |
| Intraoperative cholangiogram (IOC) | High | High | Useful during laparoscopic cholecystectomy; ~10-15% positivity rate |
ASGE Risk Stratification (most widely used framework)
| Predictor Strength | Criteria |
|---|---|
| Very strong | CBD stone on US; ascending cholangitis; bilirubin >4 mg/dL |
| Strong | Dilated CBD (>6 mm with GB in situ); bilirubin 1.8-4 mg/dL |
| Moderate | Any other abnormal liver biochemistry; age >55; clinical gallstone pancreatitis |
| Risk Category | Criteria | Pre-test Probability | Next Step |
|---|---|---|---|
| High | Any very strong predictor OR both strong predictors present | >50% | Proceed to ERCP |
| Intermediate | All other patients with some predictors | 10-50% | MRCP or EUS first |
| Low | No predictors | <10% | Cholecystectomy, consider IOC |
Note: A 2025 meta-analysis (PMID: 40569779) found that current diagnostic guidelines have limited performance in acute biliary presentations, reinforcing that clinical judgment must supplement risk stratification.
4. Imaging Examples
EUS identification of a CBD stone - hyperechoic focus with posterior acoustic shadowing:
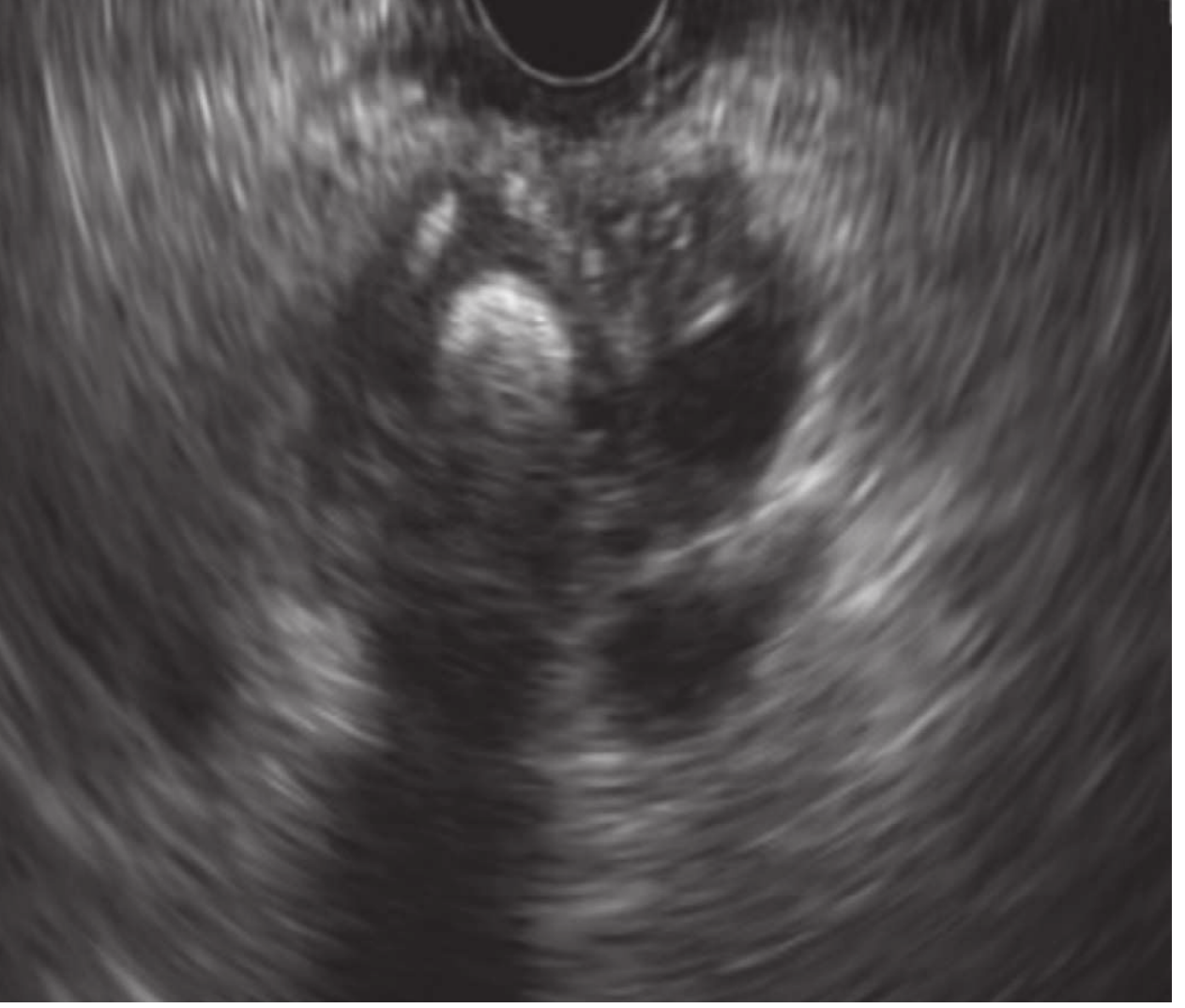
Clinical Gastrointestinal Endoscopy, 3e - Fig. 53.8
Intraoperative cholangiogram showing choledocholithiasis - note the filling defect (arrow) and no dye entering the duodenum:
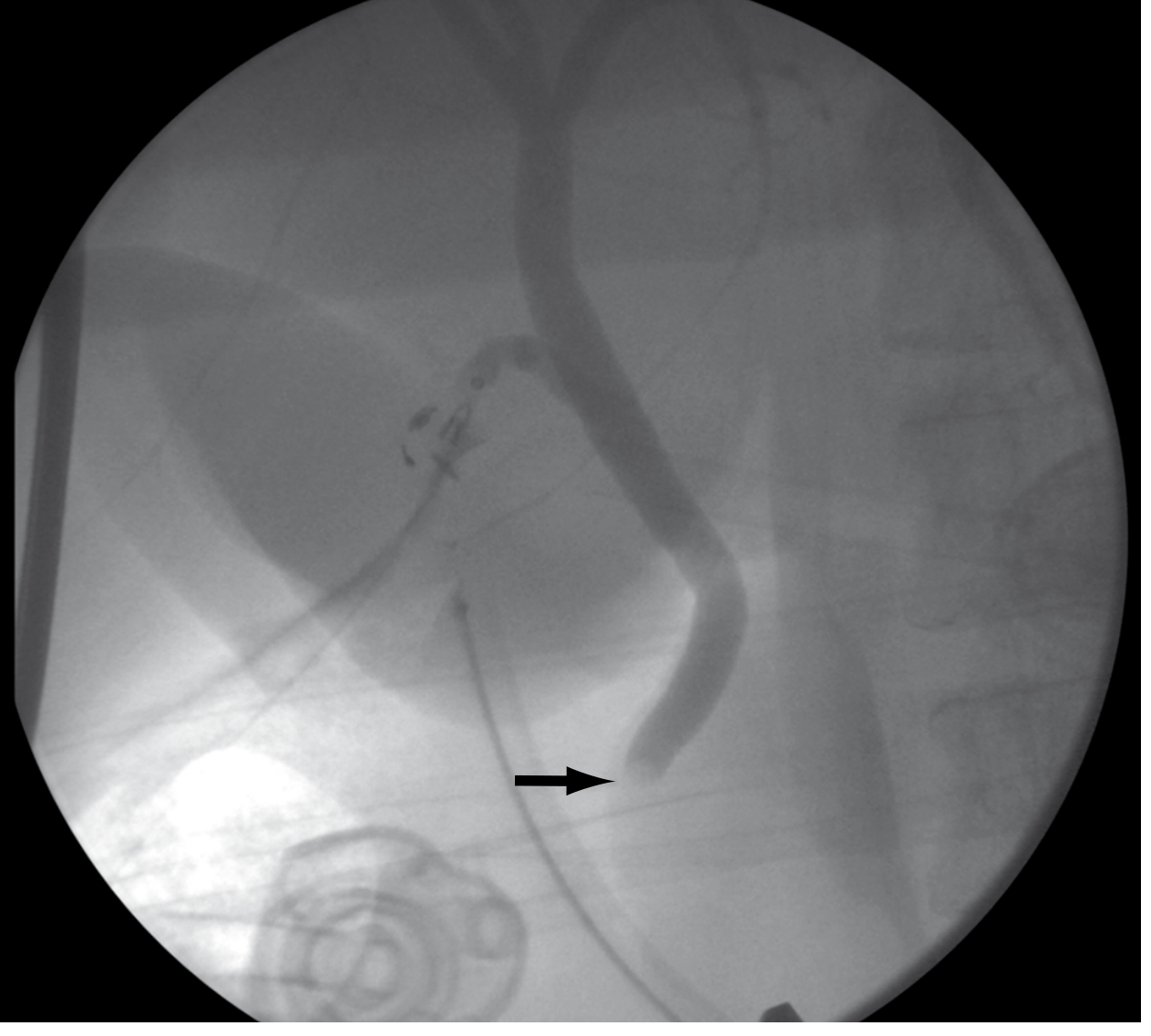
Sabiston Textbook of Surgery - Fig. 88.19
5. Management
Three main approaches exist: endoscopic, surgical, and (less commonly) percutaneous. The ideal approach depends on clinical urgency, gallbladder status, surgical expertise, and stone characteristics.
When to do ERCP first (before cholecystectomy)
- High-risk patients, especially those with ascending cholangitis needing urgent biliary decompression
- Severe gallstone pancreatitis with persistent choledocholithiasis
- Patient unfit for surgery
When to do CBD exploration at surgery
- Large or impacted stones
- Multiple failed endoscopic attempts
- Anatomy precluding endoscopy (e.g., prior Roux-en-Y gastric bypass)
- Intermediate preoperative risk with IOC confirming CBD stones intraoperatively
Endoscopic Approach (ERCP)
- Deep biliary cannulation with cholangiogram to confirm stone(s) and anatomy
- Endoscopic sphincterotomy - first therapeutic step
- Stone extraction using balloon catheters or Dormia baskets
- For large stones: endoscopic balloon dilation, mechanical lithotripsy, laser lithotripsy, or electrohydraulic lithotripsy
- ERCP is successful in ~90% of cases
- Complications: post-ERCP pancreatitis (1-5%), bleeding, perforation, ascending cholangitis
Surgical Approach
- Laparoscopic CBD exploration via transcystic or transcholedochal route - success rate 83-97% in experienced hands
- Open CBD exploration with choledochotomy and T-tube drainage, or primary closure
- Single-stage laparoscopic cholecystectomy + CBD exploration has equivalent duct clearance rates, lower morbidity, and shorter hospital stay compared to two-stage ERCP-then-laparoscopic cholecystectomy - but is highly dependent on surgeon experience
Single-stage vs. Two-stage: What does the evidence say?
A 2025 meta-analysis (PMID: 40101031) of RCTs comparing single-stage laparoscopic management vs. two-stage endoscopic + laparoscopic cholecystectomy found comparable duct clearance and morbidity, supporting single-stage as a valid option when surgical expertise is available.
Timing for Cholecystectomy
- If ERCP was done first for cholangitis or pancreatitis, cholecystectomy should follow during the same admission (or very soon after) to prevent recurrent biliary events
- Delaying cholecystectomy significantly increases the risk of recurrent cholangitis, pancreatitis, and readmission
6. Special Scenarios
Choledocholithiasis identified during cholecystectomy:
Three options: (1) Convert to open with CBD exploration, (2) laparoscopic transcystic CBD exploration, (3) postoperative ERCP. Choice depends on surgeon skill and stone characteristics.
Post-cholecystectomy retained stones (within 2 years): Treat with ERCP and sphincterotomy.
Post-cholecystectomy discovered stones (>2 years): Likely primary CBD stones; treat endoscopically; no further surgical intervention needed if gallbladder already removed.
Intermediate-risk patients: Randomized trial data favor upfront cholecystectomy with IOC over preoperative EUS/ERCP in terms of shorter hospital stay and fewer procedures.
7. Complications Summary
| Complication | Mechanism | Hallmark |
|---|---|---|
| Ascending cholangitis | Bacterial superinfection behind obstruction | Charcot's triad / Reynolds' pentad |
| Obstructive jaundice | Complete biliary obstruction | Painful jaundice, dark urine, pale stools |
| Gallstone pancreatitis | Transient ampullary obstruction | Elevated lipase, epigastric pain |
| Biliary stricture | Chronic inflammation | Recurrent cholestasis, cholangitis |
| Secondary biliary cirrhosis | Prolonged biliary obstruction | Portal hypertension, liver failure |
| Cholangiocarcinoma | Chronic inflammation → neoplasia | Rare long-term complication |
Sources: Clinical Gastrointestinal Endoscopy, 3e | Sleisenger and Fordtran's GI and Liver Disease | Mulholland & Greenfield's Surgery, 7e | Sabiston Textbook of Surgery | Symptom to Diagnosis, 4e | Fischer's Mastery of Surgery, 8e
Recent evidence note: A 2025 systematic review (PMID: 40569779) found that ASGE and other guidelines have limited overall accuracy (~63%) in predicting choledocholithiasis in acute biliary presentations - reinforcing that no guideline should replace individualized clinical assessment.
Differentials
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Excellent - rich differential content from multiple angles. Here is the complete differential diagnosis breakdown:
Differentials for Choledocholithiasis
The differentials depend on the presenting syndrome - obstructive jaundice, RUQ pain, cholangitis, or incidental biliary dilation. Organized by anatomical level and clinical urgency:
Organized by Anatomical Level of Obstruction
Low / Mid Duct (Most Common Level)
| Diagnosis | Malignant? | Key Distinguishing Features |
|---|---|---|
| Choledocholithiasis | No | Painful jaundice; acute onset; fluctuating LFTs; stone on MRCP/EUS |
| Pancreatic head carcinoma | Yes | Painless progressive jaundice; weight loss; palpable GB (Courvoisier's sign); "double-duct sign" on MRCP |
| Ampullary carcinoma | Yes | Intermittent jaundice (tumor sloughs); occult GI bleeding; periampullary mass on EUS/ERCP |
| Chronic pancreatitis stricture | No | History of alcohol/recurrent pancreatitis; calcifications on CT; gradual onset |
| Acute pancreatitis | No | Elevated lipase; pain radiating to back; peripancreatic edema on CT; may coexist with CBD stone |
| Choledochal cyst | No | Can obstruct distally; cystic dilation of duct on imaging; more common in young/Asian patients |
Hilar / Perihilar
| Diagnosis | Malignant? | Key Distinguishing Features |
|---|---|---|
| Cholangiocarcinoma (Klatskin tumor) | Yes | Hilar stricture on MRCP; intrahepatic duct dilation only; insidious painless jaundice; Bismuth classification I-IV |
| Gallbladder carcinoma | Yes | GB wall thickening or mass; direct hilar invasion; often advanced at diagnosis |
| Hepatocellular carcinoma | Yes | Cirrhotic background; elevated AFP; intrahepatic mass with biliary invasion |
| Mirizzi syndrome | No | Large cystic duct/Hartmann's pouch stone extrinsically compressing the CHD; looks malignant on imaging |
| Primary sclerosing cholangitis (PSC) | No | Beaded/multifocal strictures on cholangiography; associated with IBD (usually UC); progressive |
Either Level
| Diagnosis | Malignant? | Key Distinguishing Features |
|---|---|---|
| Postoperative biliary stricture | No | Prior cholecystectomy history; presents weeks to years later; ERCP/PTC shows smooth narrowing |
| Metastatic lymphadenopathy | Yes | Known primary malignancy; porta hepatis nodes on CT |
| Lymphoma | Yes | Systemic symptoms; lymphadenopathy elsewhere |
| Haemobilia | No | History of trauma or procedure; blood in bile; seen at ERCP |
| Parasites (Ascaris, Clonorchis) | No | Travel history; filling defects in duct; eosinophilia |
| IgG4-related sclerosing cholangitis | No | Mimics PSC or cholangiocarcinoma; responds to steroids; elevated serum IgG4 |
Differentials by Presenting Syndrome
1. Obstructive (Cholestatic) Jaundice
The core question is painful vs. painless:
- Painful jaundice with acute onset → favors choledocholithiasis (rapid distension activates pain fibers)
- Painless, progressive jaundice → strongly suggests malignancy (pancreatic head CA, cholangiocarcinoma, ampullary CA)
- Intermittent jaundice → ampullary carcinoma, Mirizzi syndrome, PSC
Courvoisier's rule: A palpable, non-tender gallbladder in a jaundiced patient suggests malignant (not stone) obstruction, since chronic choledocholithiasis leads to a fibrotic, non-distensible gallbladder.
2. RUQ Pain + Fever (Cholangitis picture)
- Choledocholithiasis (most common cause)
- Biliary stricture (post-op or PSC) with superinfection
- Biliary parasitosis (especially Ascaris or Clonorchis)
- Haemobilia (post-procedure or trauma)
- Mirizzi syndrome with secondary infection
3. Elevated LFTs / Incidental Biliary Dilation
- Choledocholithiasis (silent)
- Early PSC
- IgG4-related cholangiopathy
- Ampullary stenosis / papillary dysfunction (Sphincter of Oddi dysfunction)
- Post-cholecystectomy duct dilation (physiologic; reservoir effect - duct up to 10 mm can be normal)
- Drug-induced cholestasis (no ductal dilation)
4. Gallstone Pancreatitis Overlap
- Choledocholithiasis with pancreatitis (stone at ampulla)
- Idiopathic acute pancreatitis
- Other causes of pancreatitis (alcohol, hypertriglyceridemia, autoimmune) with incidental duct dilation
Key Differentiating Workup
| Feature | Choledocholithiasis | Malignant Obstruction | PSC | Biliary Stricture |
|---|---|---|---|---|
| Pain | Often present | Usually absent | Variable | Variable |
| Onset | Acute/fluctuating | Progressive | Insidious | Gradual (post-op) |
| LFTs | Transaminases first, then cholestatic | Predominantly cholestatic | Mixed | Cholestatic |
| Bilirubin | Fluctuates | Steadily rises | Fluctuates | Steady |
| CA 19-9 | Normal (mildly elevated if cholangitis) | Often markedly elevated | May be elevated | Normal-mildly elevated |
| US | Stone/dilation | Mass, dilation | Beading | Stricture, dilation |
| MRCP | Stone, filling defect | Stricture + mass | Multifocal beading | Smooth tapering |
| Double-duct sign | Absent | Present (pancreatic CA) | Absent | Absent |
| Response to stone removal | Resolution | No change | Partial | Variable |
Radiological Pearl: Level of Obstruction
-
Intrahepatic duct dilation only → hilar obstruction (Klatskin tumor, hilar metastases)
-
Both intra- and extrahepatic duct dilation → low/mid duct obstruction (stone, pancreatic CA, ampullary CA)
-
No duct dilation + jaundice → consider PSC, cholangitis, hepatocellular jaundice (hepatitis, cirrhosis), or drug-induced causes
-
Grainger & Allison's Diagnostic Radiology - Table 24.1
-
Sleisenger & Fordtran's GI and Liver Disease, p. 1268
-
Current Surgical Therapy, 14e, p. 577
This is a shared conversation. Sign in to Orris to start your own chat.