Tell me all about hip displacements dislocations and everything related Orthopedics - refer indian standard textbook Do point wise
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive data from multiple authoritative orthopedic textbooks. Let me compile the complete, detailed answer:
Hip Dislocations - Comprehensive Review
Sources: Miller's Review of Orthopaedics (9th Ed), Rockwood & Green's Fractures in Adults (10th Ed, 2025), Campbell's Operative Orthopaedics (15th Ed, 2026)
1. ANATOMY AND STABILITY OF THE HIP JOINT
- The hip is a ball-and-socket joint with inherent bony stability due to the deep acetabulum
- Stability is augmented by the fibrocartilaginous labrum, strong capsule (iliofemoral, pubofemoral, ischiofemoral ligaments), and ligamentum teres
- Blood supply to the femoral head comes primarily from the medial and lateral circumflex femoral arteries (branches of the profunda femoris), which form a ring giving rise to cervical retinacular vessels. A minor contribution comes from the obturator artery via the ligamentum teres
- This vascular supply is the reason dislocation leads to AVN - the capsule and retinacular vessels are at risk with any dislocation
2. INCIDENCE AND MECHANISM
- Hip dislocation is uncommon due to the joint's inherent stability - it requires high-energy trauma
- Most common mechanism: axial load with the hip in a specific position; direction of dislocation depends on hip position at time of impact
- Classic mechanism (posterior): Dashboard injury - patient seated in a car, hip flexed and adducted, femur driven posteriorly (knee hits dashboard)
- 93% rate of MRI abnormalities of the ipsilateral knee - always examine the knee
- High rate of associated systemic and musculoskeletal injuries; posterior dislocation associated with 30% rate of ipsilateral meniscal tear
- Associated injuries: posterior wall acetabular fracture, femoral head fracture, sciatic nerve injury
3. CLASSIFICATION
A. Direction-Based (Primary Classification)
| Type | Frequency | Limb Position |
|---|---|---|
| Posterior | Most common (85-90%) | Flexed, adducted, internally rotated |
| Anterior | Uncommon (~10-15%) | Extended, abducted, externally rotated |
| Central | 2-4% | Acetabular floor fracture; head driven centrally |
B. Thompson and Epstein Classification (Posterior Dislocations)
| Type | Description |
|---|---|
| I | Dislocation with or without minor fracture |
| II | Dislocation with single large fracture of the posterior rim of the acetabulum |
| III | Dislocation with comminuted fracture of the rim, with or without a large major fragment |
| IV | Dislocation with fracture of the acetabular floor |
| V | Dislocation with fracture of the femoral head |
(Source: Rockwood & Green's Fractures in Adults, 10th Ed)
C. Stewart and Milford Classification (Posterior, focuses on postreduction stability)
| Type | Description |
|---|---|
| I | Simple dislocation without fracture |
| II | Dislocation with one or more rim fragments but with sufficient socket to ensure stability after reduction |
| III | Dislocation with fracture of the rim producing gross instability |
| IV | Dislocation with fracture of the head or neck of the femur |
D. Pipkin Classification (for Thompson & Epstein Type V - with femoral head fracture)
| Type | Description |
|---|---|
| I | Posterior dislocation with femoral head fracture caudad (below) the fovea |
| II | Posterior dislocation with femoral head fracture cephalad (above) the fovea (weight-bearing surface; worse prognosis) |
| III | Femoral head fracture with associated femoral neck fracture (worst prognosis) |
| IV | Type I, II, or III with associated acetabular fracture |
(Source: Rockwood & Green's Fractures in Adults, 10th Ed)
E. Anterior Dislocation Subtypes
- Obturator (inferior): Femoral head displaces medially toward the obturator foramen - most common anterior type
- Pubic: Femoral head displaces toward the pubis
- Iliac (superior/subspinous): Femoral head displaces superolaterally toward the iliac crest
F. OTA/AO Classification (2018)
- Hip dislocation categorized as 30(5_) in the AO comprehensive fracture and dislocation system
4. CLINICAL FEATURES
Posterior Dislocation
- Leg: shortened, flexed, adducted, and internally rotated
- Patient in severe pain, unable to move the hip
- Palpable fullness in the gluteal region (femoral head posteriorly)
Anterior Dislocation
- Leg: extended, abducted, and externally rotated
- Limb may appear lengthened
- Femoral head palpable anteriorly (near groin/inguinal region)
- Risk of femoral vessel injury with superior (pubic) dislocations
General Examination Points
- Involved leg is foreshortened with excessive rotation
- Ecchymosis around abdomen, proximal thigh, or knee
- Anterior knee bruising/laceration - a sign that suggests hip dislocation ("dashboard mechanism")
- Mandatory sciatic nerve assessment before any reduction attempt in posterior dislocations
- Peroneal division most commonly affected - test foot dorsiflexion and eversion
- Distal pulses must be assessed (posterior dislocation can be associated with posterior knee dislocation; anterior dislocation may injure femoral vessels)
- Examine the spine and pelvis
5. RADIOLOGICAL EVALUATION
Pre-reduction
- AP pelvis and lateral views of the hip
- Compare femoral head sizes on AP pelvis - asymmetry helps identify direction
- In posterior dislocation: the femoral head appears smaller (farther from plate) and internally rotated
- In anterior dislocation: femoral head appears larger (closer to plate) and in abduction/external rotation
- Rule out femoral neck fracture before any reduction attempt (non-displaced neck fracture requires fixation BEFORE reduction to avoid displacement)
Post-reduction
- AP pelvis, Judet views - evaluate for acetabular fracture
- Fine-cut CT scan - mandatory after reduction to:
- Confirm concentric reduction
- Identify loose bodies in joint
- Assess femoral head fracture
- Assess acetabular wall fracture
6. TREATMENT
A. Emergency Closed Reduction - URGENT (within 6 hours)
- AVN rate is 2-10% if reduction occurs within 6 hours
- AVN rate exceeds 50% if reduction is delayed more than 12 hours
- A delay >12 hours increases AVN risk 5.6 times
- Most cases of AVN appear within 2 years of injury
- Reduction can be done in the ER if the patient is intubated or no OR is available; otherwise, general/spinal anesthesia in OR preferred
- Principle: Traction in line with the femur and gentle rotation - never use sudden forceful movements (risk of femoral neck fracture and articular damage)
B. Allis Maneuver (for Posterior Dislocation) - Most Common
- Patient supine on a stable radiolucent table
- Assistant stabilizes the pelvis - pushes down on the ASIS and laterally on the inner proximal thigh
- Surgeon flexes the knee and hip to 90° (relaxes hamstrings)
- Apply steady longitudinal traction with the extremity in internal rotation and adduction
- Gently rotate the leg while applying traction to achieve reduction
- Modifications: "East Baltimore lift" (multiple assistants), lateral position reduction (reduces back strain on surgeon)
- After reduction: extend and externally rotate the hip, place a knee immobilizer
C. Stimson (Gravity) Technique (Posterior Dislocation)
- Patient placed prone with the leg hanging over the edge of the bed
- Hip and knee both flexed to 90 degrees
- Downward (gravity-assisted) traction applied; gentle rotation aids reduction
- Advantage: less muscular effort required; useful when an assistant is unavailable
D. Captain Morgan Technique
- Physician's knee used as a fulcrum
- Surgeon places their knee under the patient's popliteal fossa, lifts upward while applying downward pressure on the ankle
E. Walker Modification of Allis (Anterior Dislocation)
- For inferior (obturator) dislocations: Continuous traction in line with the femur + gentle flexion + lateral push on the inner thigh + internal rotation and adduction
- For superior (pubic/iliac) dislocations: Distal traction until head is at acetabular level, then gentle internal rotation; extension may be needed
- Always continuous traction - never short jerky movements
F. Reverse Bigelow Technique (Anterior Dislocation)
- Hip placed in partial flexion and abduction
- Traction applied along the long axis of the femur
- Gently adduct and internally rotate the leg to achieve reduction
7. CONTRAINDICATIONS TO CLOSED REDUCTION
- Pipkin Type III and IV (associated femoral neck fracture or complex fracture pattern)
- Incongruent reduction
- Loose bodies interfering with articulation
- Displaced femoral neck fractures
- Associated pelvic ring fractures (countertraction impossible - open reduction needed)
- Irreducibility after 2-3 attempts under adequate anesthesia - proceed to open reduction
8. OPERATIVE TREATMENT - INDICATIONS
- Irreducible dislocation (muscle, capsule, labrum, loose body interposed)
- Incongruent reduction due to loose body or fracture fragment
- Sciatic nerve injury following reduction attempt
- Pipkin Types II, III, IV - ORIF of femoral head fracture indicated
- Posterior wall fracture causing instability (requires ORIF)
- Pipkin Type I - trial of closed reduction acceptable if fragment is caudal to fovea and not impinging; operative if displaced
Types of operative management:
- Open reduction with/without debridement
- Open reduction and internal fixation (ORIF)
- Total hip arthroplasty (in elderly, or failed ORIF cases, or post-AVN collapse)
9. POST-REDUCTION MANAGEMENT
- Fluoroscopic evaluation after closed reduction for Pipkin Type I cases and suspected instability from posterior wall fracture
- Weight bearing as tolerated (if hip is stable and no associated fractures requiring fixation)
- Traction and/or hip abduction pillow for unstable injuries pending definitive management of associated injuries
- Small bony fragments in fovea centralis: do not require removal as long as they are not impinging on the articular surface and are not between joint surfaces
- Physiotherapy program: gradual mobilization, protected weight bearing as per stability
10. COMPLICATIONS
Early
| Complication | Details |
|---|---|
| Sciatic nerve injury | Up to 20%; peroneal division most commonly affected; must assess PRE-reduction and post-reduction |
| Vascular injury | Rare; femoral vessels at risk in anterior (superior) dislocations |
| Ipsilateral knee injury | 93% MRI abnormality rate; 30% meniscal tear; ligamentous injuries |
| Femoral head/neck fracture | Associated in Pipkin types; neck fracture must be ruled out before reduction |
| Missed injuries | Acetabular fractures, posterior wall fractures frequently missed |
Late
| Complication | Details |
|---|---|
| Avascular Necrosis (AVN) | Up to 15% overall; most cases appear within 2 years of injury; risk dramatically increased with delayed reduction |
| Post-traumatic Osteoarthritis | Common; less frequent when associated with posterior wall acetabular fracture |
| Recurrent dislocation | Rare |
| Heterotopic Ossification | Can follow operative treatment |
| Stiffness/restricted ROM | Secondary to capsular scarring |
AVN incidence from historical series:
- Thompson & Epstein (1951): 10% AVN, 7% OA
- Dreinhofer et al. (1994): 19% AVN in posterior, 0% in anterior
- Reduction >12 hours: 5.6x increased risk of AVN
11. SPECIAL CONSIDERATIONS
Ipsilateral Femoral Neck Fracture (Critical Point)
- Most difficult associated injury to diagnose (can be non-displaced and subtle)
- Always rule out with high-quality radiographs +/- fine-cut CT before any reduction attempt
- If present: fix the femoral neck FIRST, then reduce the hip
- Attempting reduction with an unrecognized femoral neck fracture can displace it - catastrophic complication
Hip Prosthesis Dislocation
- More common than native hip dislocation
- Most common after posterior approach THA
- Treated with closed reduction; recurrent dislocation may require revision surgery or constraint liner
Pediatric Hip Dislocation (Developmental Dysplasia of Hip - DDH)
- Different entity from traumatic dislocation
- Managed with Pavlik harness (0-6 months), closed reduction and spica cast (6-18 months), open reduction with or without osteotomy (>18 months or failed closed reduction)
- Femoral shortening osteotomy + Dega/Salter/triple pelvic osteotomy used in complex cases
12. PROGNOSIS
- Results strongly correlate with time to reduction - early reduction is the single most important factor
- Good and excellent outcomes in 48-87% depending on series and associated injuries
- Posterior dislocations carry higher AVN risk than anterior dislocations
- Associated femoral head/acetabular fractures worsen prognosis
- Pipkin Type III has the worst prognosis due to combined femoral neck + femoral head + dislocation injury
References:
- [Miller's Review of Orthopaedics, 9th Ed](Miller's Review of Orthopaedics 9th Edition) - Sections on Young Adult Proximal Femur Injuries, Hip Dislocations
- [Rockwood and Green's Fractures in Adults, 10th Ed, 2025](Rockwood and Green's fractures in adults 10th ed 2025) - Chapter 52: Hip Dislocations, Classification, Reduction Techniques
- [Campbell's Operative Orthopaedics, 15th Ed, 2026](Campbell's Operative Orthopaedics 15th Ed 2026) - Hip Dislocation and Fracture-Dislocation sections
Anything about hip displacement And not hip dislocation
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Here is the complete guide on Hip Displacement (excluding traumatic dislocation):
HIP DISPLACEMENT - Complete Guide
Sources: Miller's Review of Orthopaedics (9th Ed), Campbell's Operative Orthopaedics (15th Ed, 2026), Rockwood & Green's Fractures in Adults (10th Ed, 2025)
PART 1 - DEVELOPMENTAL DYSPLASIA OF THE HIP (DDH)
1. DEFINITION AND OVERVIEW
- DDH represents abnormal development or dislocation of the hip secondary to capsular laxity and mechanical factors (e.g., intrauterine positioning)
- Formerly called "Congenital Dislocation of Hip (CDH)" - now replaced by DDH as the term reflects a spectrum, not just dislocation
- Occurs during late pregnancy or early infancy
2. SPECTRUM OF DISEASE (5 Types)
| Form | Description |
|---|---|
| Dysplasia | Shallow acetabulum only - femoral head in socket but acetabular roof inadequate |
| Subluxation | Femoral head partially displaced from acetabulum |
| Dislocation | Complete loss of contact between femoral head and acetabulum |
| Teratologic | Dislocated in utero, irreducible at birth; associated with neuromuscular conditions (arthrogryposis, Larsen syndrome) |
| Late Dysplasia | Presents in adolescence or adulthood |
3. RISK FACTORS
- Breech positioning (strongest risk factor - 30-50% incidence)
- Female sex (85% of cases)
- Positive family history (ligamentous laxity) - >20% incidence
- Firstborn child (less intrauterine space)
- Left hip more often involved (67% of cases)
- Postnatal swaddling with hips extended
- Increased maternal estrogens
- Associated conditions: torticollis (20%), metatarsus adductus (10%); no association with clubfoot
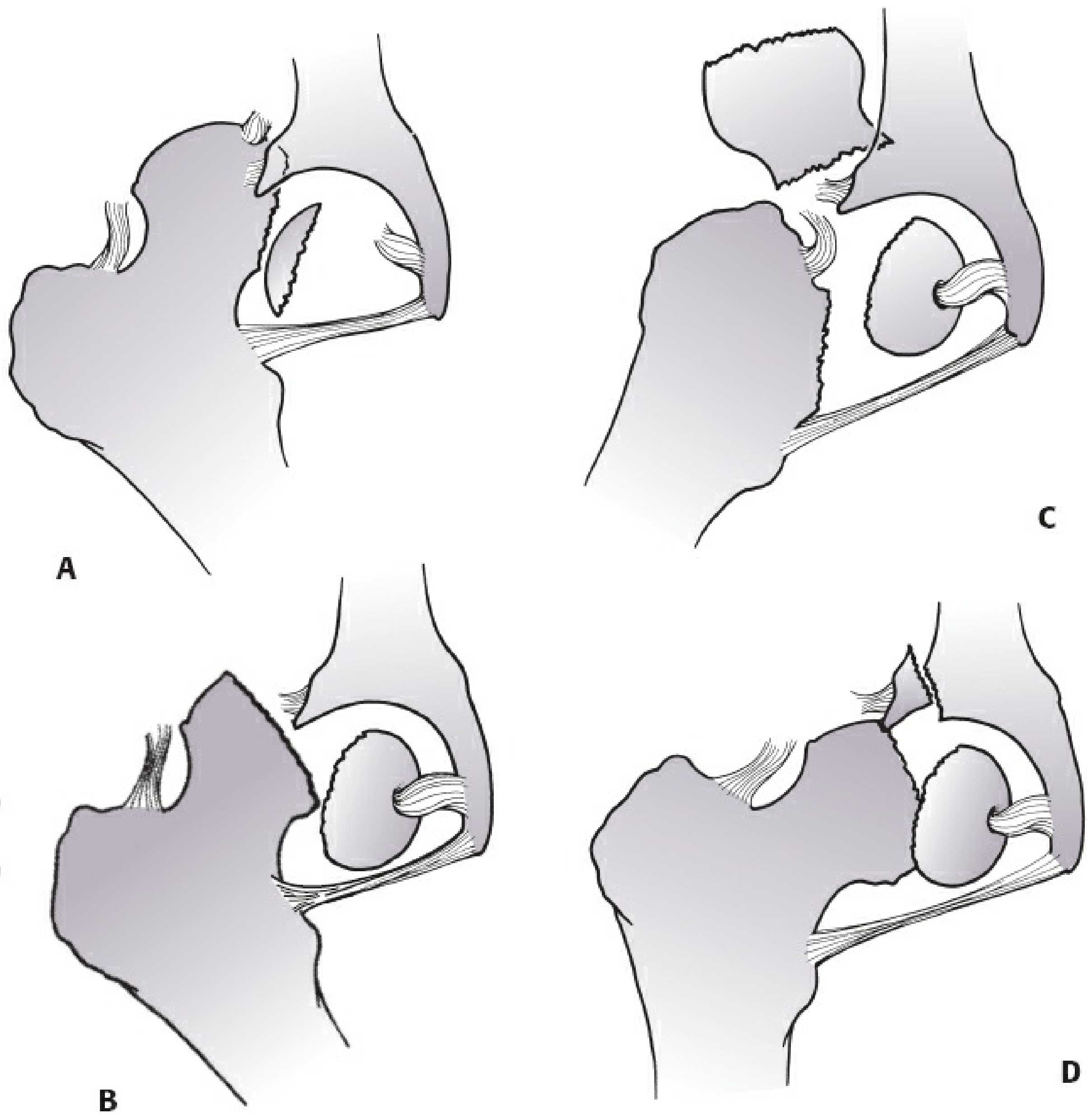
4. PATHOLOGY - BLOCKS TO REDUCTION
If left untreated, the following structures prevent concentric reduction:
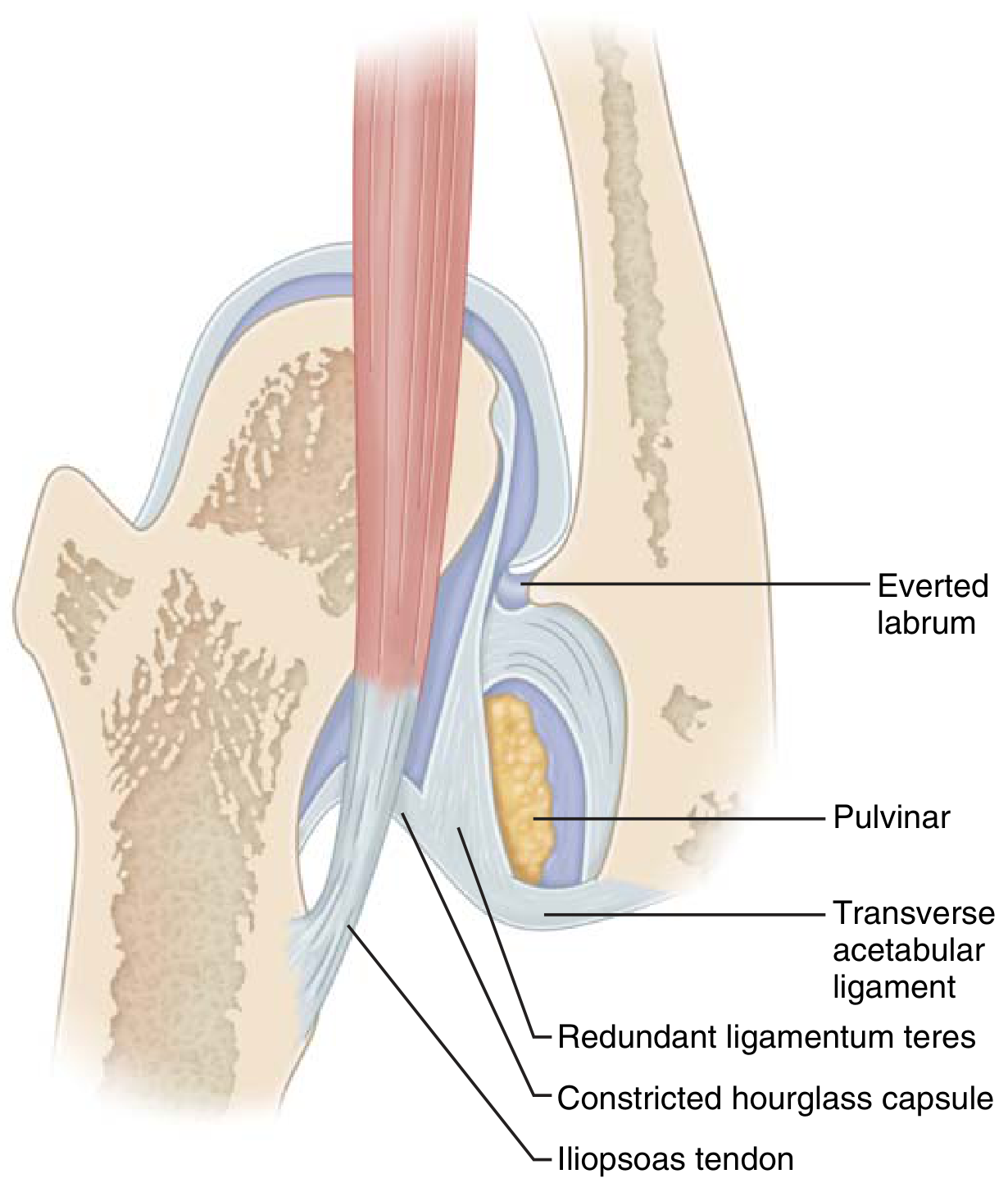
- Iliopsoas tendon - constricts capsule at acetabular entry
- Pulvinar - fibrofatty tissue filling the acetabulum
- Hypertrophied ligamentum teres
- Contracted inferomedial hip capsule (hourglass deformity)
- Transverse acetabular ligament - blocks inferior entry
- Inverted (everted) labrum
5. CLINICAL FEATURES
Physical Examination - Screening Tests
- Ortolani Test (reduction test): Elevation + abduction of flexed hip - a "clunk" of relocation indicates a dislocated but reducible hip (positive in early DDH)
- Positive = Dislocated hip
- Barlow Test (provocation test): Adduction + posterior pressure on flexed hip - a "clunk" of subluxation indicates a reducible but dislocatable hip
- Positive = Dislocatable hip
Three Phases of DDH on Examination
| Phase | Test | Clinical state |
|---|---|---|
| Dislocated | Ortolani positive (early); Ortolani negative (late - irreducible) | Hip is out |
| Dislocatable | Barlow positive | Hip is in but can be pushed out |
| Subluxable | Barlow suggestive | Partial displacement possible |
Other Clinical Signs (Older Children)
- Galeazzi sign - foreshortening of femur on affected side (knees at different heights with hips and knees flexed, feet together)
- Limited hip abduction on affected side (most reliable sign after 3 months)
- Asymmetric gluteal skin folds (less reliable)
- Trendelenburg sign and gait in walking children
- Increased lumbar lordosis
- Pelvic obliquity
- In bilateral DDH: abduction may be decreased symmetrically - easy to miss
6. RADIOLOGICAL INVESTIGATIONS
Ultrasonography (Gold Standard - Birth to 4 months)
- Femoral head is cartilaginous at birth and not visible on X-ray
- Dynamic ultrasound (Graf method) used for screening and follow-up
- Alpha angle (α): Normal > 60 degrees (between bony roof and ilium); <50° = dysplastic
- Femoral head should be bisected by the line drawn down the ilium on coronal view
- Also useful for: monitoring Pavlik harness reduction, assessing acetabular dysplasia
- Screening ultrasound recommended for children with significant risk factors
Plain Radiograph (from 4-6 months onwards - when ossific nucleus appears)
Key measurements:
| Measurement | Normal | Significance |
|---|---|---|
| Acetabular Index (AI) | <25° | Increased = dysplastic |
| Perkin's line | Ossific nucleus medial to this vertical line | Lateral = displaced |
| Shenton's line | Smooth continuous arc from femoral neck to superior obturator foramen | Disrupted = subluxation/dislocation |
| Hilgenreiner's line | Horizontal through triradiate cartilage | Used with Perkin's line to form quadrants |
| Ossification | Begins 4-6 months | Delayed on affected side |
- Arthrography - useful to assess concentric reduction and identify blocks
- CT/MRI - after closed reduction to confirm concentric position
7. TREATMENT (Age-Based Algorithm)
Goal: Achieve and maintain early concentric reduction to prevent degenerative joint disease
Birth to 6 months - Pavlik Harness
- Ortolani-positive (dislocated) hips: Pavlik harness immediately
- Barlow-positive (dislocatable) hips: close observation or Pavlik harness
- Maintains hip in ~100° flexion and mild abduction ("human position" / Salter position)
- Hip maintained within "safe zone of Ramsey" - between maximum adduction (redislocation risk) and excessive abduction (AVN risk)
- Confirm reduction by radiograph/ultrasound after harness placement
- Continue until examination and ultrasound are normal
- If not reduced in harness: transition to rigid abduction orthosis OR closed reduction + spica cast
- Contraindications: Teratologic hip dislocation, narrow safe zone <40° (consider adductor tenotomy)
- Excessive flexion in Pavlik harness can cause femoral nerve palsy
6 to 18 months - Closed Reduction and Spica Casting
- Hip arthrography + percutaneous adductor tenotomy + closed reduction under anesthesia
- Spica cast application (human/frog-leg position)
- Post-reduction CT or MRI to confirm concentric reduction
- If closed reduction fails: open reduction
18 months to 3 years - Open Reduction
- Open reduction required (soft tissue contractures, ossification progressing)
- Often with femoral shortening osteotomy + possible acetabular osteotomy
- Approach: anterolateral (Smith-Petersen/bikini incision)
3 to 8 years - Acetabular Osteotomy (with or without femoral osteotomy)
| Osteotomy | Type | Indication |
|---|---|---|
| Salter | Open-wedge osteotomy through ilium | Concentric reduction; age <6 years |
| Pemberton | Incomplete iliac osteotomy (hinges on triradiate cartilage) | Acetabular remodeling |
| Dega | Hinges on medial wall of pelvis | Posterior/lateral deficiency; cerebral palsy |
| Staheli (shelf) | Bone graft augmentation | Lateral coverage |
Older than 8 years (Growth Plate Open) - Triple/Double Pelvic Osteotomies
- Triple pelvic osteotomy (Steele/Tonnis) - three cuts around acetabulum; allows rotation in all directions
- Double pelvic osteotomy (Sutherland)
- Chiari osteotomy - medial displacement osteotomy (salvage procedure; creates fibrocartilaginous coverage)
Growth Plate Closed (Adolescent/Adult) - Periacetabular Osteotomy (PAO)
- Ganz PAO (Bernese osteotomy) - gold standard for adolescent/adult dysplasia
- Preserves posterior column blood supply; allows large correction
- Total Hip Arthroplasty (THA) when patient is adult with end-stage osteoarthritis
8. COMPLICATIONS OF DDH AND ITS TREATMENT
| Complication | Details |
|---|---|
| Avascular Necrosis (AVN) | Caused by excessive abduction (compression of posterior retinacular artery); most serious treatment complication |
| Redislocation | After closed or open reduction |
| Residual dysplasia | Inadequate acetabular coverage; leads to early OA |
| Femoral nerve palsy | Excessive hip flexion in Pavlik harness |
| Late osteoarthritis | Untreated or inadequately treated DDH |
PART 2 - SLIPPED CAPITAL FEMORAL EPIPHYSIS (SCFE)
1. DEFINITION
- Displacement of the proximal femoral epiphysis (femoral head) from the femoral neck through the physeal plate
- The epiphysis (head) remains in the acetabulum; the metaphysis (neck) displaces anteriorly and superiorly relative to the head
- Net effect: the femoral neck rotates into external rotation and valgus relative to the head = the head appears to "slip" posteriorly and inferiorly
- SCFE is a Salter-Harris Type I fracture through the proximal femoral physis
2. EPIDEMIOLOGY
- Age: 10-16 years (puberty/rapid growth phase); 78% during rapid growth phase
- Males more common (2:1 ratio)
- Obesity is the single most consistent risk factor
- African descent (twice as common as European)
- Bilateral involvement in 25-40%; second slip occurs within 12-18 months
- Left hip slightly more common than right
3. ETIOLOGY AND PATHOPHYSIOLOGY
Physeal Factors (Mechanical)
- Growth spurt causes pathophysiologic changes in physis
- Decrease in neck-shaft angle with growth in adolescents
- Increase in obliquity of physis with growth - more shear force
- Thinning of perichondrial ring
- Decrease in size of epiphyseal tubercle and physeal widening
Risk/Etiologic Factors (Box 38.8, Campbell's)
- Obesity (increased shear stress across physis)
- Open triradiate cartilage
- Inflammatory conditions
- Endocrine disorders: hypothyroidism, hypopituitarism, chronic renal disease, hypogonadism
- Down syndrome
- Local trauma with shear or torsional forces
- Genetics
Atypical SCFE
- Children <10 or >16 years, or below 50th percentile in weight: 4.2-8.4x more likely to have atypical/endocrine cause
- Must screen for underlying endocrinopathy
4. CLASSIFICATION
A. Loder Classification (Stability - Most Important Clinically)
| Type | Definition | AVN Rate | Outcome |
|---|---|---|---|
| Stable | Patient can walk, with or without crutches | 0% | 96% satisfactory |
| Unstable | Cannot walk even with crutches due to severe pain | 47% | 47% satisfactory |
B. Severity / Grade Classification (Southwick Head-Shaft Angle)
| Grade | Displacement | Head-shaft angle deviation |
|---|---|---|
| Preslip | Physeal widening/irregularity; edema on MRI; no displacement | - |
| Mild (Grade I) | <1/3 diameter of femoral head | ≤30° |
| Moderate (Grade II) | 1/3 to 1/2 diameter | 30-60° |
| Severe (Grade III) | >1/2 diameter | >60° |
(60-90% of SCFE are chronic; >50% are mild slips)
C. Chronological Classification (Less Commonly Used Now)
| Type | Duration | Features |
|---|---|---|
| Acute | <3 weeks symptoms | Acute onset, may be unstable |
| Chronic | >3 weeks symptoms | Most common; mild symptoms |
| Acute-on-chronic | Acute episode on background of chronic | Prior prodrome + sudden worsening |
5. CLINICAL FEATURES
- Pain in the groin, hip, medial thigh, or knee (referred knee pain in 20% - frequently causes delayed diagnosis)
- Limitation of internal rotation - hallmark sign
- When hip is flexed, leg externally rotates into frog-leg position (obligate external rotation on flexion - pathognomonic)
- Chronic SCFE: mild/moderate shortening of affected extremity
- Fixed external rotation with outward foot progression angle
- Trendelenburg gait
- SCFE should be suspected in any obese adolescent with knee or hip pain and limited internal rotation
6. RADIOLOGICAL EVALUATION
Plain Radiograph (AP + Frog-Leg Lateral Pelvis - Most Important)
- AP view: The femoral head appears "smaller" and displaced; metaphyseal blanch sign (double density at metaphysis because neck has moved anteriorly)
- Klein's Line (most important sign on AP):
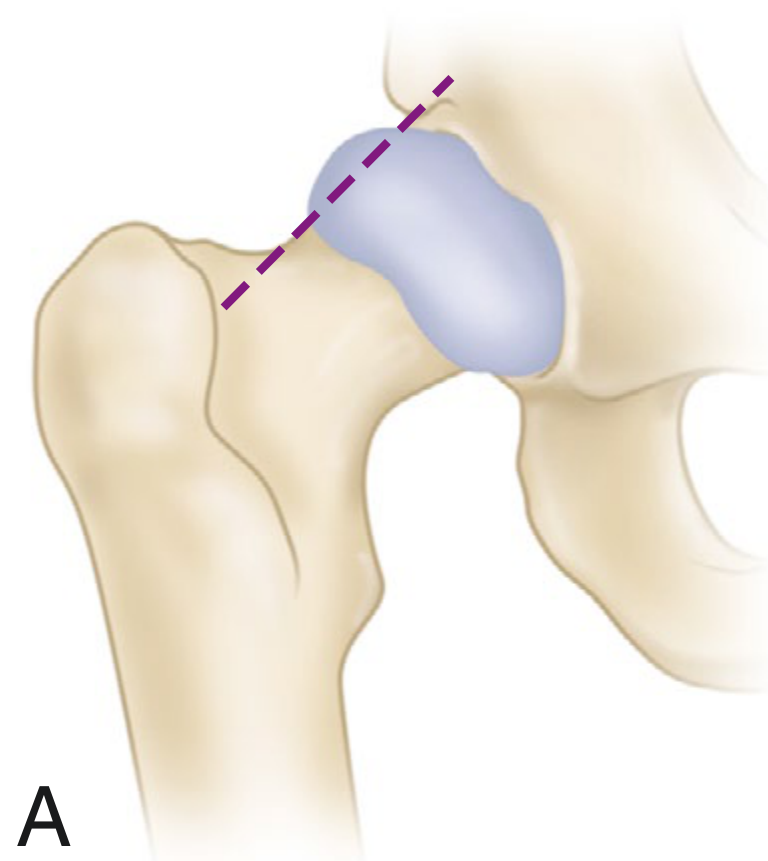
-
Line drawn along the superior (lateral) femoral neck should intersect the epiphysis normally
-
In SCFE: epiphysis is flush with or below this line (does not intersect)
-
Modified: slip present if maximal width of epiphysis lateral to Klein's line differs ≥2 mm vs. contralateral side (improves sensitivity from 40% to ~80%)
-
Frog-leg lateral view: More sensitive for early/mild slips
Advanced Imaging
- MRI: Diagnosis of "preslip" - edema around physis on T2; rules out additional pathology; assesses femoral head perfusion
- CT: Determines if physis is closed; preoperative planning for complex osteotomies; Southwick angle measurement
7. TREATMENT
Key principle: DO NOT attempt forceful reduction - high risk of AVN
Stable SCFE - In Situ Fixation (Standard of Care)
- Percutaneous in situ single cannulated screw fixation - most commonly used for both stable and unstable SCFE
- Single large-diameter screw in center-center position of the epiphysis
- Screw placed no closer than 4 mm from subchondral bone to avoid penetration
- Occasionally a second screw used for high-grade slips
- Multiple radiographic views mandatory to ensure no screw penetration
Unstable SCFE - Gentle/Incidental Reduction + Fixation
- Simple positioning on the operating table may achieve gentle reduction
- Leadbetter Maneuver (gentle, not forceful):
- Flex hip to 90° and slightly adduct
- Apply longitudinal traction
- Rotate leg 45°
- Slightly abduct and extend
- Forceful manipulation is absolutely contraindicated - directly causes osteonecrosis
- After gentle reduction: percutaneous cannulated screw fixation
Moderate/Severe SCFE
- Open reduction + ORIF (Dunn procedure / modified Dunn procedure using surgical dislocation approach) - for moderate/severe slips to restore epiphyseal alignment
- Extracapsular base-of-neck osteotomy - for moderate/severe slips at skeletal maturity
- In situ fixation remains acceptable even for severe slips in some cases (accepts deformity to avoid AVN)
Contralateral Hip
- Prophylactic pinning debated; recommended in children at higher risk (endocrinopathy, age <10, bilateral involvement likely)
Atypical SCFE
- Treat underlying endocrinopathy first
- Close follow-up with radiographs
- Smooth-proximal/threaded-distal pins used to allow continued physeal growth while preventing further slip
8. COMPLICATIONS OF SCFE
| Complication | Details |
|---|---|
| Osteonecrosis (AVN) | Unstable SCFE: 47%; Stable SCFE: 0%; Caused by forceful reduction, delayed fixation, or vascular disruption |
| Chondrolysis | Cartilage dissolution; associated with screw penetration, immobilization in cast, or Black race; presents with hip stiffness and pain |
| Cam-type FAI | Posterior slip deformity creates anterior cam lesion; leads to femoroacetabular impingement in adult life |
| Leg length discrepancy | Secondary to physeal damage |
| Premature physeal closure | Secondary to pinning |
| Screw penetration | Joint sepsis, acetabular erosion, synovitis, chondrolysis, late OA |
| Degenerative osteoarthritis | Long-term consequence |
PART 3 - HIP SUBLUXATION
1. DEFINITION
- Partial loss of contact between the femoral head and acetabulum - unlike dislocation (complete loss of contact)
- Represents the intermediate point on the spectrum: normal → subluxation → dislocation
2. CAUSES
| Cause | Category |
|---|---|
| DDH (early/mild form) | Developmental - most common in infants |
| Cerebral Palsy | Neuromuscular - spasticity of hip flexors and adductors; hip abductor weakness |
| Spina Bifida (myelomeningocele) | Paralytic - unopposed hip flexors/adductors |
| Muscular Dystrophy | Neuromuscular - muscle imbalance |
| Post-traumatic | After fractures around the hip |
| Post-radiation | Growth plate damage |
3. HIP SUBLUXATION IN CEREBRAL PALSY
- Caused by spastic imbalance: hip flexors and adductors overpower abductors and extensors
- Characterized by four progressive stages:
- Hip at risk: Abduction <45°, partial uncovering on X-ray; exception to avoiding surgery <3 years in CP
- Hip subluxation: Best treated with adductor tenotomy if abduction <20°; sometimes + psoas release
- Spastic dislocation: May need open reduction, femoral shortening, VDRO + pelvic osteotomy (Dega)
- Windswept hips: One hip abducted, contralateral adducted; bilateral femoral osteotomies to varus angle
- Radiographic measure: migration percentage (Reimer's index) - % of femoral head uncovered by acetabulum
- Treatment of one hip can prevent dislocation of the contralateral hip
Surgical Options for CP Hip Subluxation/Dislocation
| Procedure | Indication |
|---|---|
| Adductor tenotomy ± psoas release | Mild subluxation (abduction <20°) |
| Open reduction + femoral VDRO | Reducible dislocation, femoral coxa valga |
| Dega osteotomy | Posterior/lateral acetabular deficiency |
| Girdlestone resection arthroplasty | Late painful dislocation - salvage |
| Schanz abduction osteotomy | Late painless dislocation - improve seating |
4. HIP SUBLUXATION IN SPINA BIFIDA (Myelomeningocele)
- Most common at L3-L4 level (unopposed iliopsoas with paralysed abductors/extensors)
- Containment is controversial - principles follow any paralytic hip dislocation
- Thoracic-level myelomeningocele: functional outcome independent of hip position/dislocation status
- Late dislocation at low lumbar level may be caused by tethered spinal cord - must be released before hip reduction
- Management priority: limiting soft tissue contractures; functional goals over anatomic
SUMMARY TABLE
| Feature | DDH | SCFE | Subluxation (CP) |
|---|---|---|---|
| Age | Birth-infancy (late dysplasia in adolescence) | 10-16 years | Any age; CP usually childhood |
| Sex | Female predominance (85%) | Male predominance (2:1) | Equal |
| Mechanism | Capsular laxity + intrauterine/postnatal factors | Physeal failure during growth spurt | Muscle imbalance/spasticity |
| Key sign | Ortolani/Barlow, Galeazzi | Obligate external rotation on flexion; limited IR; knee pain | Limited abduction; Trendelenburg |
| Key X-ray sign | Disrupted Shenton's line, increased acetabular index | Klein line positive, metaphyseal blanch sign | Migration percentage |
| Key imaging | Ultrasound (0-4 months), then X-ray | AP + frog-leg X-ray | AP X-ray; migration percentage |
| Treatment | Age-based: Pavlik → closed reduction → open reduction → osteotomy | In situ cannulated screw fixation | Adductor release → VDRO → Dega osteotomy |
| Worst complication | AVN from excessive abduction; late OA | AVN (47% in unstable SCFE); chondrolysis | Established painful dislocation |
Sources:
- Miller's Review of Orthopaedics, 9th Ed - DDH (pp. 264-270), Cerebral Palsy Hip (pp. 304-305), SCFE
- [Campbell's Operative Orthopaedics, 15th Ed 2026](Campbell's Operative Orthopaedics 15th Ed 2026) - Chapters on DDH, SCFE (pp. 1832-1848)
- [Rockwood & Green's Fractures in Adults, 10th Ed, 2025](Rockwood and Green's fractures in adults 10th ed 2025) - Hip Dislocation classification tables
This is a shared conversation. Sign in to Orris to start your own chat.