Ecg
Reading File
Asking for Preferences
Finding Sources
Searching the Web
ECG interpretation basics normal waveforms intervals
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have rich textbook content and images to put together a comprehensive ECG overview. Here it is:
Electrocardiogram (ECG) - Complete Overview
What is an ECG?
An ECG (electrocardiogram) is a non-invasive recording of the electrical activity of the heart at the body surface. It provides direct measurement of the rate, rhythm, and time-dependent electrical vector of the heart, and gives fundamental information about the origin and conduction of the cardiac action potential. - Medical Physiology
The Cardiac Conduction System
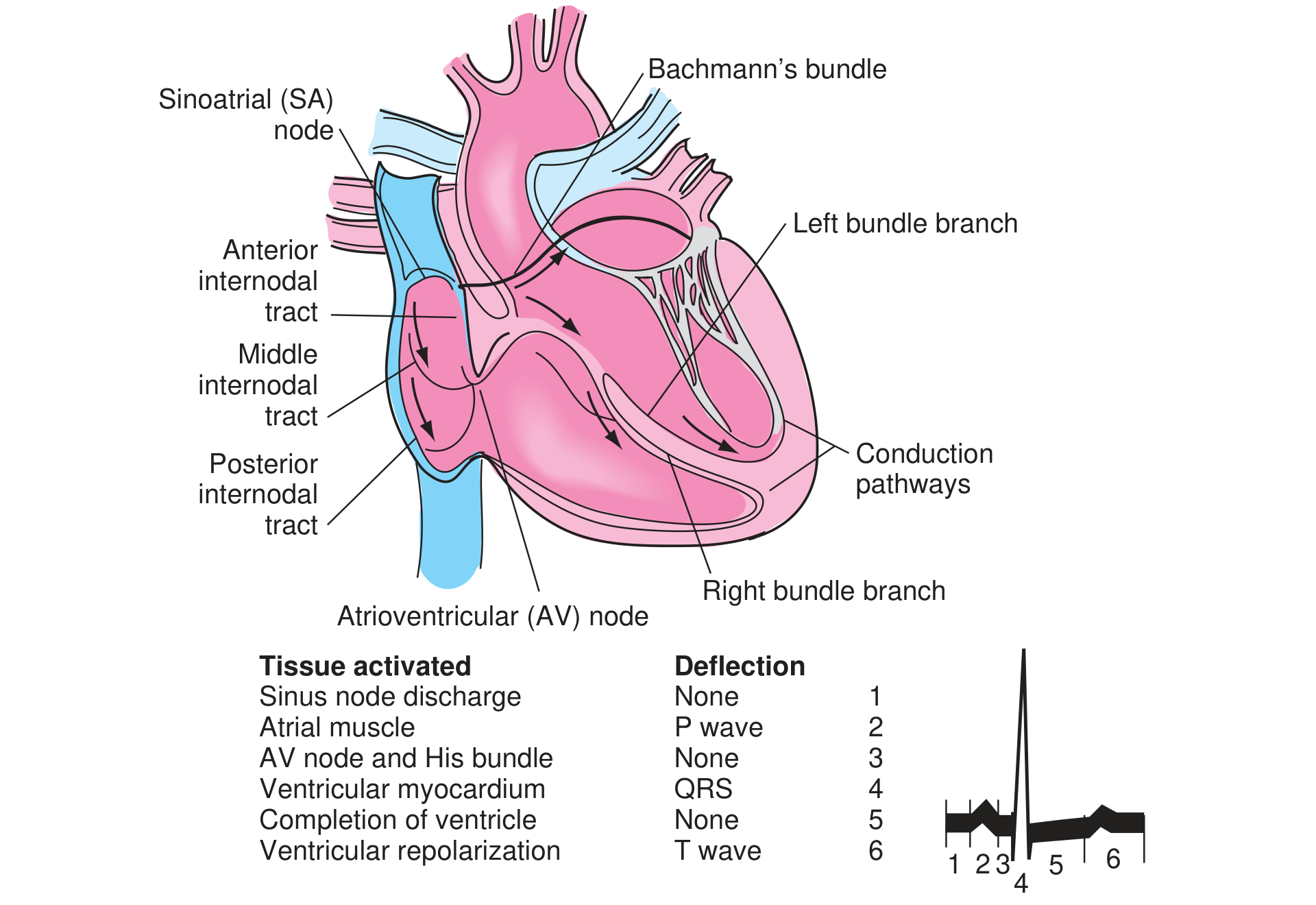
The electrical impulse travels through the heart in this sequence:
| Tissue Activated | ECG Deflection |
|---|---|
| SA node discharge | None (silent) |
| Atrial muscle | P wave |
| AV node + His bundle | None (isoelectric PR segment) |
| Ventricular myocardium | QRS complex |
| Completion of ventricle | None (ST segment) |
| Ventricular repolarization | T wave |
- The SA node fires spontaneously, spreading depolarization through both atria via Bachmann's bundle and the internodal tracts
- At the AV node, conduction slows deliberately - creating the PR delay between atrial and ventricular contraction
- From the His bundle, the impulse travels through the left and right bundle branches into the Purkinje fibers, rapidly depolarizing the ventricles
ECG Paper & Calibration
- Vertical axis: 0.1 mV per 1 mm square
- Horizontal axis: 0.04 sec per small box (1 mm) | 0.2 sec per large box (5 mm)
- Five large boxes = 1.0 second
The Normal Waveforms, Segments & Intervals

P Wave
- Represents atrial depolarization
- Normally upright in inferior leads (II, III, aVF)
- Duration: 0.06-0.12 sec (1.5-3 small boxes)
- Amplitude: 2-3 mm
PR Interval
- From start of P wave to start of QRS
- Represents time for conduction through the AV node
- Normal: 0.12-0.20 sec (3-5 small boxes)
- Prolonged in AV block; shortened in pre-excitation (WPW)
QRS Complex
- Represents ventricular depolarization
- Normally starts with a small Q (septal), then tall R (ventricular mass), then S wave
- Normal duration: up to 0.10 sec (2.5 small boxes)
- Wide QRS (>0.12 sec) = bundle branch block or ventricular origin
ST Segment
- From end of QRS (J point) to start of T wave
- Represents the plateau phase of the ventricular action potential
- Normally isoelectric (flat at baseline)
- Elevation = ischemia/injury/infarction or pericarditis
- Depression = subendocardial ischemia or reciprocal change
T Wave
- Represents ventricular repolarization
- Normally upright in most leads; inverted in aVR
- Peaked/tall T waves = hyperkalemia or hyperacute MI
- Inverted T waves = ischemia, ventricular hypertrophy
QT Interval
- From start of QRS to end of T wave
- Represents the entire ventricular action potential duration
- Normal: up to 0.43 sec (rate-corrected QTc)
- Shortens with faster heart rates (inverse relationship)
- Prolonged QT = risk of torsades de pointes
Key Intervals - Normal Values
(Ganong's Review of Medical Physiology)
| Interval | Average | Normal Range | What it Measures |
|---|---|---|---|
| PR interval | 0.18 sec | 0.12-0.20 sec | AV conduction time |
| QRS duration | 0.08 sec | up to 0.10 sec | Ventricular depolarization |
| QT interval | 0.40 sec | up to 0.43 sec | Ventricular action potential |
| ST interval (QT - QRS) | 0.32 sec | - | Plateau phase |
Heart Rate Calculation
Method 1 (regular rhythm): Rate = 60 / R-R interval in seconds
Quick method: Count large boxes in the R-R interval and use the sequence:
300 - 150 - 100 - 75 - 60 - 50
Each number corresponds to 1, 2, 3, 4, 5, or 6 large boxes between R waves. For example, 4 large boxes between R waves = 75 bpm.
The 12 Leads
Bipolar limb leads (measure potential difference between two limbs):
- Lead I: Left arm (+) vs Right arm (-)
- Lead II: Left leg (+) vs Right arm (-)
- Lead III: Left leg (+) vs Left arm (-)
Augmented unipolar limb leads:
- aVR (right arm), aVL (left arm), aVF (left foot)
Precordial (chest) leads: V1-V6, placed across the chest wall
Each lead "looks" at the heart from a different angle. This allows localization of pathology to specific regions of the heart.
Systematic ECG Interpretation (Step-by-Step)
- Rate - Regular or irregular? Calculate bpm
- Rhythm - Sinus (P before every QRS)? Regular?
- P wave - Present, upright, normal morphology?
- PR interval - Normal (0.12-0.20 sec)?
- QRS complex - Narrow or wide? Normal morphology?
- Axis - Normal (-30° to +90°)?
- ST segment - Elevation or depression?
- T wave - Upright and normal?
- QT interval - Prolonged?
Key ECG Abnormalities
| Finding | Likely Cause |
|---|---|
| ST elevation | STEMI, pericarditis, Brugada, LBBB |
| ST depression | NSTEMI, subendocardial ischemia, digoxin |
| Wide QRS (>0.12 sec) | Bundle branch block, ventricular tachycardia, hyperkalemia |
| Prolonged PR (>0.20 sec) | First-degree AV block |
| Absent P waves + irregular rhythm | Atrial fibrillation |
| Regular wide-complex tachycardia | Ventricular tachycardia |
| Delta wave + short PR | Wolff-Parkinson-White (pre-excitation) |
| Peaked T waves | Hyperkalemia |
| Q waves (pathological) | Old myocardial infarction |
ECG in Myocardial Infarction
The ECG changes in acute MI arise from three mechanisms (Ganong's Review of Medical Physiology):
| Defect in Infarcted Cells | Current Flow | ECG Change |
|---|---|---|
| Rapid repolarization | Out of infarct | ST elevation |
| Decreased resting membrane potential | Into infarct | ST elevation (via TQ depression) |
| Delayed depolarization | Out of infarct | ST elevation |
Over time, the ECG evolves: ST elevation (minutes-hours) → T wave inversion → pathological Q waves (permanent scar)
Sources: Ganong's Review of Medical Physiology (26th ed.) | Medical Physiology | Miller's Anesthesia (10th ed.) | Textbook of Family Medicine (9th ed.)
Want me to go deeper on any specific aspect - arrhythmia recognition, axis determination, bundle branch blocks, or a particular condition?
This is a shared conversation. Sign in to Orris to start your own chat.