Anemia
Asking for Preferences
Asking for Preferences
Reading File
Finding Sources
Searching PubMed
"iron deficiency anemia"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching Images
iron deficiency anemia peripheral blood smear microcytic hypochromic
Reading File
Reading File
Loading Image
I now have comprehensive information to provide a thorough, well-cited overview. Let me compile the response.
Iron Deficiency Anemia (IDA)
Iron deficiency is the most common nutritional disorder in the world and the leading cause of anemia globally. It affects ~10% of people in high-resource countries and 25–50% in low-resource settings.
Epidemiology & High-Risk Groups
- Toddlers and infants (low iron in breast milk: ~0.3 mg/L)
- Adolescent girls and premenopausal women (menstrual loss)
- Pregnant women (increased demand)
- Vegans (lack of heme iron)
- The elderly and impoverished
- Adult men and postmenopausal women with unexplained IDA → must be assumed to have GI blood loss until proven otherwise
Iron Metabolism (Key Concepts)
| Parameter | Males | Females |
|---|---|---|
| Total body iron | ~3.5 g | ~2.5 g |
| Hemoglobin compartment | 2100 mg | 1750 mg |
| Storage (ferritin + hemosiderin) | 1000 mg | 400 mg |
- Daily losses: 1–2 mg/day (shed epithelial cells); no regulated excretion pathway
- Daily requirement: ~7–10 mg (men), 7–20 mg (women)
- Dietary heme iron (from meat): ~20% absorbed; non-heme iron: only 1–2% absorbed
- Hepcidin (liver peptide) is the master regulator — it degrades ferroportin, suppressing iron absorption when stores are adequate; upregulated by IL-6 in inflammation (mechanism of anemia of chronic disease)
- Absorption enhancers: ascorbic acid, citric acid, amino acids
- Absorption inhibitors: tannins (tea), carbonates, oxalates, phosphates
— Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 612; Robbins & Kumar Basic Pathology, p. 393
Causes
| Category | Examples |
|---|---|
| Dietary lack | Low-resource countries; vegans; infants; elderly |
| Impaired absorption | Celiac disease, sprue, gastrectomy, H. pylori infection, IBD (proximal small bowel) |
| Increased requirement | Pregnancy, infancy, adolescence |
| Chronic blood loss (most common in developed countries) | GI bleeding (cancer, ulcer, hookworm), menorrhagia, urinary tract loss |
In adult men and postmenopausal women in high-income countries, IDA must be attributed to GI blood loss until proven otherwise — an occult GI cancer may be the source.
— Robbins, Cotran & Kumar, p. 613
Pathophysiology (Stages of Depletion)
- Stage 1 – Pre-latent: Iron stores (ferritin) depleted; serum iron and Hb still normal; ↑ bone marrow erythroid activity
- Stage 2 – Latent iron deficiency: ↓ Serum iron and transferrin saturation; no anemia yet; ↑ TIBC
- Stage 3 – Iron deficiency anemia: Stores exhausted → ↓ Hb → microcytic, hypochromic anemia
Laboratory Findings
| Test | Iron Deficiency | Inflammation (ACD) | Thalassemia |
|---|---|---|---|
| Serum iron (µg/dL) | < 30 | < 50 | Normal–high |
| TIBC (µg/dL) | > 360 | < 300 | Normal |
| Transferrin saturation | < 10% | 10–20% | 30–80% |
| Ferritin (µg/L) | < 15 | 30–200 | 50–300 |
| Smear | Micro/hypo | Normal or mild micro/hypo | Micro/hypo + targeting |
— Harrison's Principles of Internal Medicine, 21st ed., p. 2889
Peripheral Blood Smear
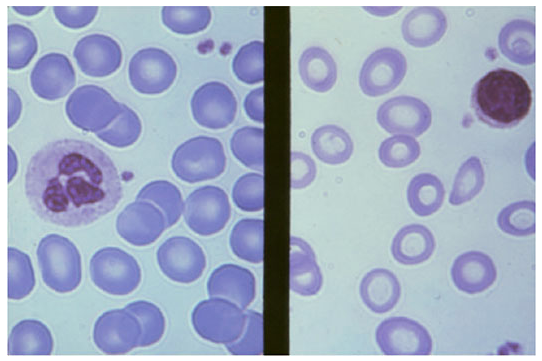
Normal red cells (left) vs. iron deficiency anemia (right): cells are smaller (microcytic) with greatly increased central pallor (hypochromic). Poikilocytes (pencil cells, elliptocytes) may also be present.
Clinical Features
Symptoms of anemia:
- Fatigue, weakness, exertional dyspnea, pallor, palpitations
Signs specific to iron deficiency (severe/chronic):
- Koilonychia (spoon nails)
- Pica — craving for non-food items (ice = pagophagia, dirt = geophagia)
- Glossitis and angular stomatitis
- Plummer-Vinson syndrome — IDA + esophageal webs + dysphagia (rare)
- Restless leg syndrome association
Diagnosis
- CBC: ↓ Hb, ↓ MCV (microcytic), ↓ MCH (hypochromic), ↑ RDW
- Serum ferritin < 15 µg/L (most specific single test for depletion)
- ↓ Serum iron, ↑ TIBC, transferrin saturation < 10%
- Bone marrow: absent Prussian blue–stainable iron (gold standard, rarely needed)
- Reticulocyte response to iron therapy confirms diagnosis
GI evaluation (for adult men of any age and postmenopausal women):
- Colonoscopy first → upper endoscopy + push enteroscopy if negative → duodenal biopsy for celiac disease → test for H. pylori → capsule endoscopy if all negative
— Goldman-Cecil Medicine, p. 1424
Treatment
1. Oral Iron (First-line)
| Preparation | Tablet Size | Elemental Iron/Tablet | Usual Adult Dose (tablets/day) |
|---|---|---|---|
| Ferrous sulfate (hydrated) | 325 mg | 65 mg | 2–4 |
| Ferrous gluconate | 325 mg | 36 mg | 3–4 |
| Ferrous fumarate | 325 mg | 106 mg | 2–3 |
Key points:
- Ferrous (Fe²⁺) salts are absorbed ~3× better than ferric (Fe³⁺) salts
- Optimal dose: 150–200 mg elemental iron/day; once-daily dosing on an empty stomach may maximize absorption by avoiding hepcidin-mediated suppression from multiple daily doses
- Continue for 3–6 months after Hb normalizes to replenish stores
- Ascorbic acid (≥200 mg) co-administration increases absorption by ~30%
- Take separately from antacids, dairy, tea, and calcium supplements
- Hb should rise ~1–2 g/dL per week with adequate therapy; reticulocytosis peaks at 7–10 days
Side effects (dose-related): nausea, epigastric discomfort, constipation/diarrhea, black stools (no clinical significance)
— Katzung's Basic & Clinical Pharmacology, 16th ed., p. 932; Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 929
2. Parenteral Iron (Reserved for specific indications)
Indications: intolerance/malabsorption of oral iron, hemodialysis patients on erythropoietin, inflammatory bowel disease involving proximal small bowel, post-gastrectomy, rapid repletion needed.
Available agents:
- Iron dextran — IV or IM; test dose required (anaphylaxis risk)
- Sodium ferric gluconate complex — lower anaphylaxis risk
- Iron sucrose — well tolerated, widely used in renal patients
- Ferric carboxymaltose / ferumoxytol — newer agents, high-dose single infusions possible
3. Blood Transfusion
Reserved for severe symptomatic anemia (Hb < 7–8 g/dL with hemodynamic compromise) or urgent pre-operative correction.
Summary: IDA at a Glance
| Feature | Detail |
|---|---|
| Most common cause (developed world) | Chronic GI blood loss |
| Most common cause (globally) | Dietary insufficiency |
| Most specific lab test | Serum ferritin < 15 µg/L |
| Smear morphology | Microcytic, hypochromic; pencil cells, poikilocytes |
| First-line treatment | Oral ferrous sulfate 325 mg once daily |
| Treatment duration | 3–6 months after Hb correction |
| Must exclude in adult men/postmenopausal women | GI malignancy |
This is a shared conversation. Sign in to Orris to start your own chat.