Cardiorenal syndrome pearl in a photo
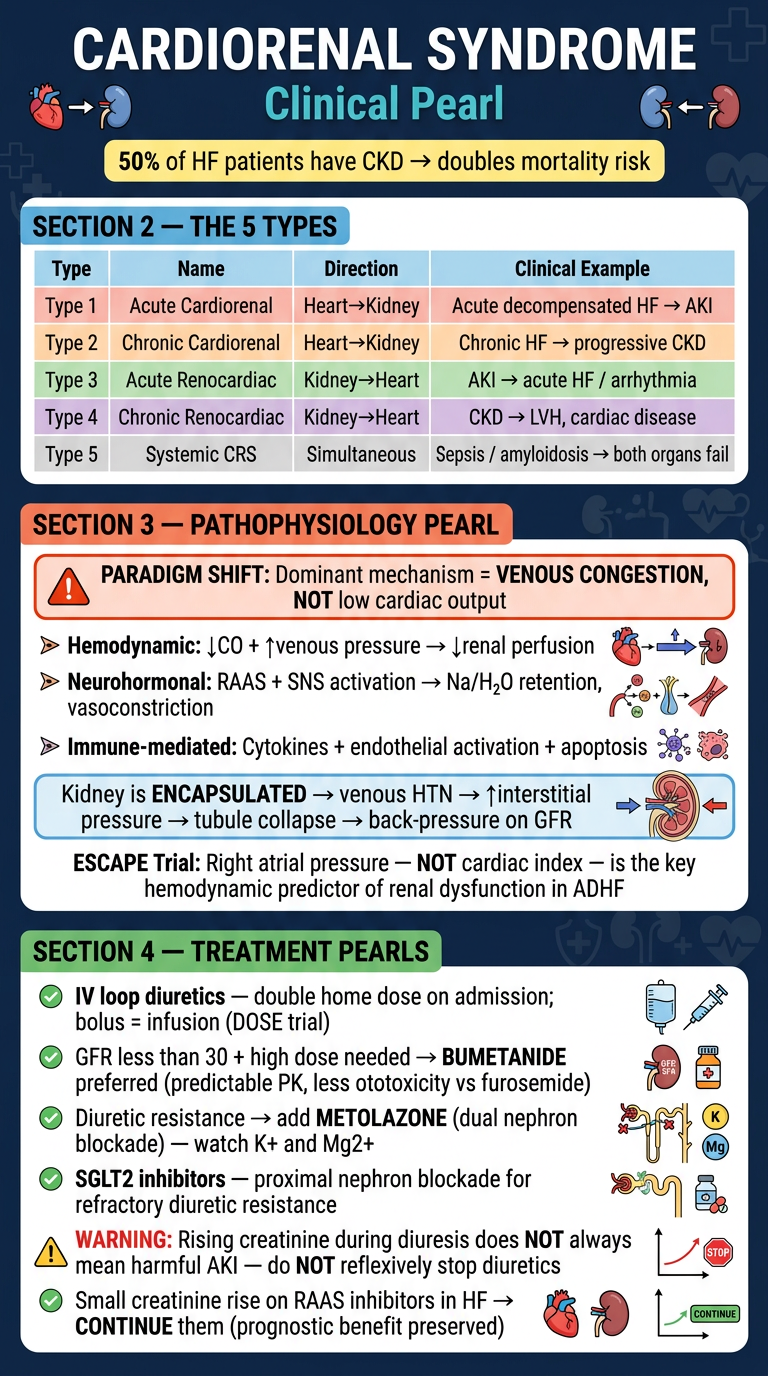
Cardiorenal Syndrome - Clinical Pearl
What is CRS?
The 5 Types (Ronco Classification)
| Type | Name | Direction | Example |
|---|---|---|---|
| 1 | Acute cardiorenal | Heart → Kidney | Acute decompensated HF → AKI |
| 2 | Chronic cardiorenal | Heart → Kidney | Chronic HF → progressive CKD |
| 3 | Acute renocardiac | Kidney → Heart | AKI → acute HF, arrhythmia |
| 4 | Chronic renocardiac | Kidney → Heart | CKD → LVH, cardiac disease |
| 5 | Systemic CRS | Simultaneous | Sepsis, amyloidosis → both organs fail |
Key Pathophysiology Pearl
- The ESCAPE trial showed right atrial pressure (not cardiac index) was the only hemodynamic parameter independently associated with renal dysfunction
- Increased central venous pressure → renal venous hypertension → increased Bowman's capsule pressure → back-pressure on GFR
- The kidney is an encapsulated organ: venous congestion raises interstitial pressure, compresses tubules, and collapses them - reducing GFR through back-pressure
- ADHERE Registry confirmed: worsened kidney function was equally prevalent in HFpEF and HFrEF, meaning systolic dysfunction alone does not explain CRS
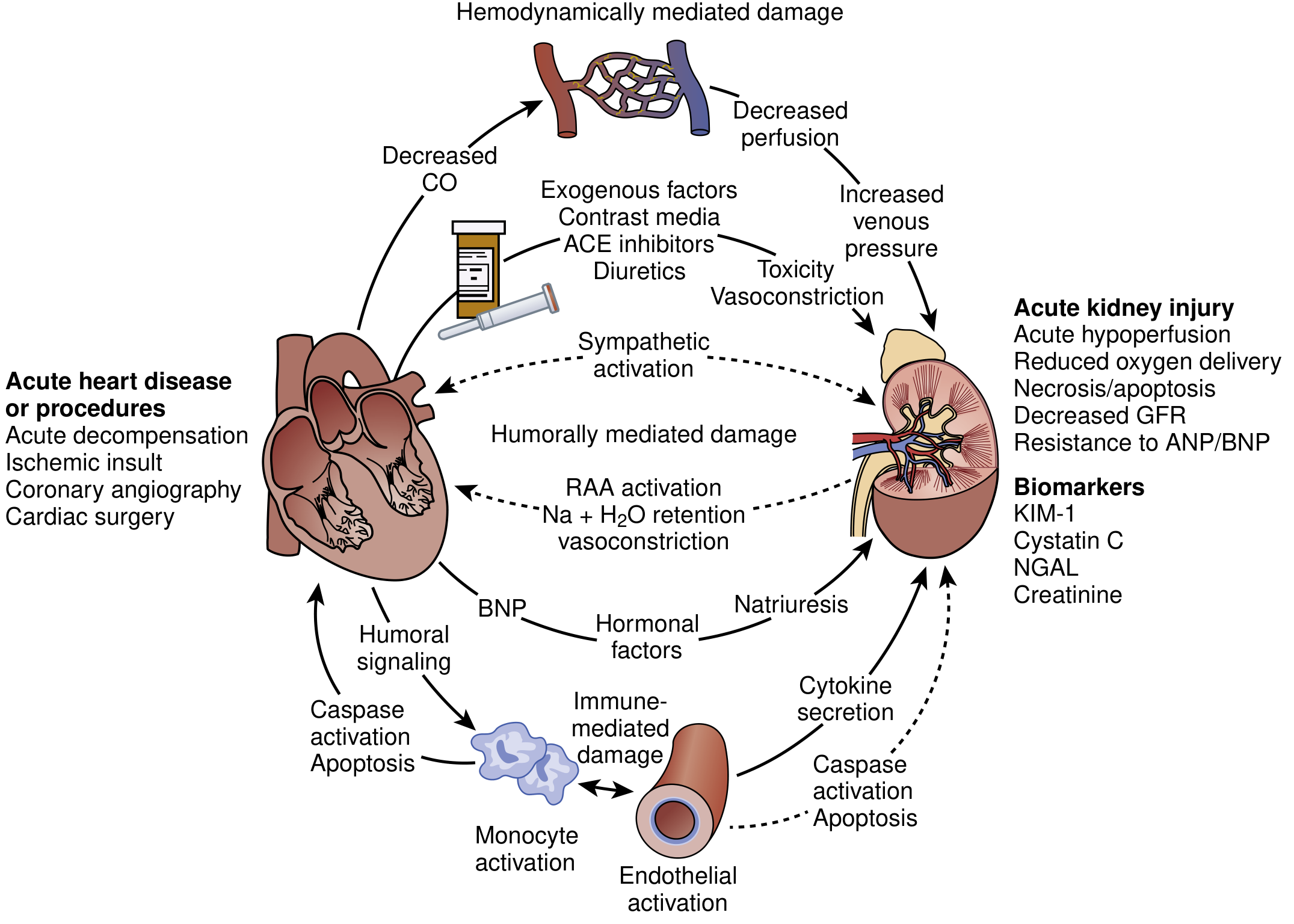
- Hemodynamic - decreased CO + increased venous pressure → decreased perfusion
- Neurohormonal - RAAS + sympathetic activation → Na/H₂O retention, vasoconstriction
- Immune-mediated - cytokine secretion, endothelial activation, apoptosis
Treatment Pearl
- IV loop diuretics (double home dose on admission; bolus = infusion per DOSE trial)
- For GFR < 30 + high diuretic need: bumetanide > furosemide (predictable pharmacokinetics, less ototoxicity)
- Diuretic resistance → add metolazone (dual nephron blockade) - watch K⁺ and Mg²⁺
- SGLT2 inhibitors emerging as add-on proximal nephron blockade in resistant cases
All of this info in one photo
A detailed medical education infographic/poster titled "Cardiorenal Syndrome (CRS) Clinical Pearl" with a dark navy blue background and clean white/colored text. The poster is divided into clear sections: TOP SECTION - Title: "CARDIORENAL SYNDROME" in large bold white text, subtitle "Clinical Pearl" in teal/cyan. Below it a one-liner: "Bidirectional dysfunction — heart and kidney each worsen the other. 50% of HF patients have CKD → doubles mortality." SECOND SECTION - "THE 5 TYPES" with a clean table layout showing: - Type 1 | Acute Cardiorenal | Heart→Kidney | Acute decompensated HF → AKI - Type 2 | Chronic Cardiorenal | Heart→Kidney | Chronic HF → progressive CKD - Type 3 | Acute Renocardiac | Kidney→Heart | AKI → acute HF/arrhythmia - Type 4 | Chronic Renocardiac | Kidney→Heart | CKD → LVH, cardiac disease - Type 5 | Systemic CRS | Both simultaneously | Sepsis/amyloidosis → both organs fail Each type in a different color row. MIDDLE SECTION - "KEY PATHOPHYSIOLOGY PEARL" with a bold red/orange highlight box: "⚠ PARADIGM SHIFT: Dominant mechanism = VENOUS CONGESTION, not low cardiac output" Three injury pathways shown as icons/bullets: 1. Hemodynamic: ↓CO + ↑venous pressure → ↓renal perfusion 2. Neurohormonal: RAAS + SNS activation → Na/H₂O retention, vasoconstriction 3. Immune-mediated: Cytokines + endothelial activation + apoptosis A small callout box: "Kidney is ENCAPSULATED → venous HTN → ↑interstitial pressure → tubule collapse → back-pressure on GFR" "ESCAPE Trial: Right atrial pressure (NOT cardiac index) = only hemodynamic predictor of renal dysfunction" BOTTOM SECTION - "TREATMENT PEARLS" with a green header: • IV loop diuretics — double home dose on admission (bolus = infusion, per DOSE trial) • GFR <30 + high dose needed → use BUMETANIDE (predictable PK, less ototoxic vs furosemide) • Diuretic resistance → add METOLAZONE (dual nephron blockade) — monitor K⁺ and Mg²⁺ • SGLT2 inhibitors — proximal nephron blockade for refractory cases • ⚠ TRAP: Rising Cr during diuresis ≠ always harmful AKI — do NOT reflexively stop diuretics • Small Cr rise on RAAS inhibitors in HF → continue them (prognostic benefit preserved) Clean medical infographic style, well-organized, easy to read, professional cardiology/nephrology reference card aesthetic. Include small heart and kidney icons near the title.
All this info in one photo
A detailed medical education infographic poster titled "CARDIORENAL SYNDROME — Clinical Pearl" on a dark navy blue background. Professional cardiology/nephrology reference card style with clean layout, white and colored text, small heart and kidney icons near the title. SECTION 1 — TITLE AREA: Large bold white title: "CARDIORENAL SYNDROME" Teal subtitle: "Clinical Pearl" Yellow callout box: "50% of HF patients have CKD → doubles mortality risk" SECTION 2 — "THE 5 TYPES" (colored table): Type 1 | Acute Cardiorenal | Heart→Kidney | Acute decompensated HF → AKI Type 2 | Chronic Cardiorenal | Heart→Kidney | Chronic HF → progressive CKD Type 3 | Acute Renocardiac | Kidney→Heart | AKI → acute HF / arrhythmia Type 4 | Chronic Renocardiac | Kidney→Heart | CKD → LVH, cardiac disease Type 5 | Systemic CRS | Simultaneous | Sepsis / amyloidosis → both organs fail SECTION 3 — "PATHOPHYSIOLOGY PEARL" with orange/red alert box: "PARADIGM SHIFT: Dominant mechanism = VENOUS CONGESTION, NOT low cardiac output" Three bullet pathways: • Hemodynamic: ↓CO + ↑venous pressure → ↓renal perfusion • Neurohormonal: RAAS + SNS activation → Na/H₂O retention, vasoconstriction • Immune-mediated: Cytokines + endothelial activation + apoptosis Key fact box: "Kidney is ENCAPSULATED → venous HTN → ↑interstitial pressure → tubule collapse → back-pressure on GFR" "ESCAPE Trial: Right atrial pressure — NOT cardiac index — is the key hemodynamic predictor of renal dysfunction in ADHF" SECTION 4 — "TREATMENT PEARLS" with green header: • IV loop diuretics — double home dose on admission; bolus = infusion (DOSE trial) • GFR less than 30 + high dose needed → BUMETANIDE preferred (predictable PK, less ototoxicity vs furosemide) • Diuretic resistance → add METOLAZONE (dual nephron blockade) — watch K+ and Mg2+ • SGLT2 inhibitors — proximal nephron blockade for refractory diuretic resistance • WARNING: Rising creatinine during diuresis does NOT always mean harmful AKI — do NOT reflexively stop diuretics • Small creatinine rise on RAAS inhibitors in HF → CONTINUE them (prognostic benefit preserved)