Biliary ascleresis usg reporting and impressive
Reading File
Finding Sources
Searching the Web
biliary atresia ultrasound USG reporting findings triangular cord sign 2024
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information. Let me compile the full answer.
Biliary Atresia - USG Reporting & Findings
Note: The query appears to be "biliary atresia" (not "biliary ascleresis" - there is no recognized condition by that name). If you meant a different condition, please clarify.
Background
Biliary atresia (BA) is a neonatal fibro-obliterative disease of the extrahepatic and/or intrahepatic bile ducts, occurring in ~1:8,000-18,000 live births. It is the most common cause of childhood liver transplant. Jaundice persisting beyond 2 weeks of life should raise suspicion.
Fasting ultrasound is the gold-standard first-line investigation when biliary atresia is suspected.
Sonographic Signs of Biliary Atresia
1. Triangular Cord Sign (Most Specific)
The most important and specific USG finding.
- Defined as a triangular or tubular echogenic density (fibrous ductal remnant) located cranial to the portal vein bifurcation, at the anterior aspect of the right portal vein at its bifurcation
- Represents the fibrotic obliterated remnant of the extrahepatic bile ducts
- Positive criterion: thickness of echogenic anterior wall of right portal vein (EARPV) >3-4 mm on longitudinal scan
Diagnostic performance (meta-analysis of 20 studies):
- Sensitivity: 74% (95% CI: 0.61-0.84)
- Specificity: 97% (95% CI: 0.95-0.99) - highly specific
- Accuracy: ~93-94%
- PPV: ~94%, NPV: ~94%
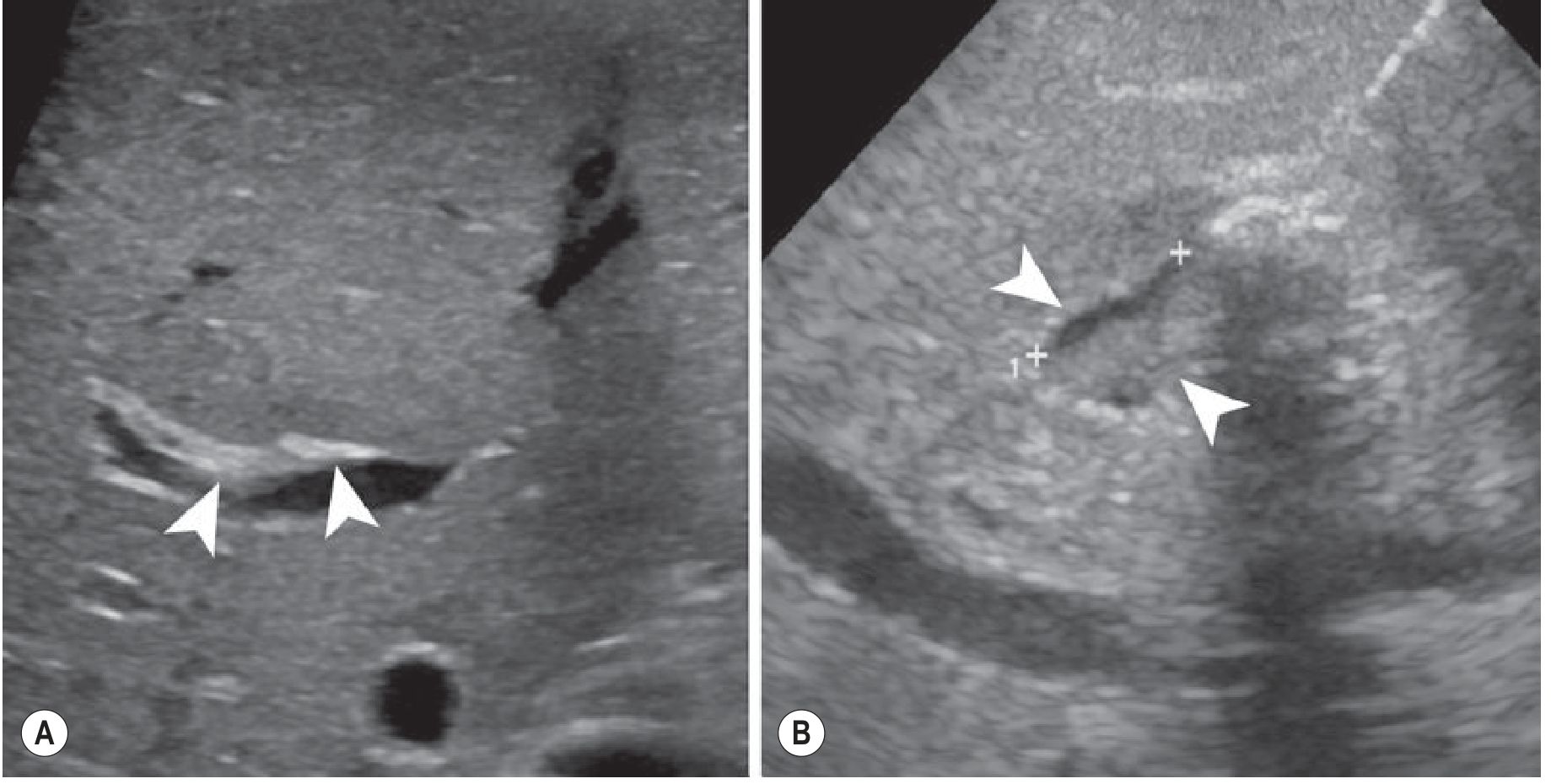
Fig: (A) Fibrous atretic plate (arrowheads) at porta hepatis - Triangular cord sign. No biliary dilatation is present. (B) Small (~10 mm) gallbladder with abnormal wall (arrowheads). - Grainger & Allison's Diagnostic Radiology
2. Gallbladder Abnormalities
Diagnostic performance (meta-analysis of 19 studies):
- Sensitivity: 85% (95% CI: 0.76-0.91)
- Specificity: 92% (95% CI: 0.81-0.97)
Abnormalities include:
| Finding | Detail |
|---|---|
| Absent gallbladder | Specificity ~99%; highly diagnostic |
| Small gallbladder | Length <1.5 cm (fasting), or <1.9 cm |
| Gallbladder "Ghost" Triad | (a) Length <1.9 cm, (b) lack of smooth/complete echogenic mucosal lining with indistinct wall, (c) irregular or lobular contour |
| Abnormal wall | Irregular, non-smooth, poorly defined wall |
| Dysmotility | No contraction after feeding |
Note: In ~10% of BA patients, the distal biliary tract is patent and a gallbladder may be seen - so presence of gallbladder does NOT exclude BA.
3. Absence of Common Bile Duct
- Non-visualization of the CBD is a supporting finding
- Less valuable than triangular cord sign and gallbladder findings
4. No Biliary Dilatation
- Critical negative finding - intrahepatic bile ducts are NEVER dilated in BA
- This differentiates BA from choledochal malformation and other obstructive causes
- Absence of biliary dilatation or sludge in a jaundiced infant should prompt suspicion for BA
5. Hepatic Artery Enlargement
- Hepatic artery diameter >2 mm at the porta hepatis is a supporting sign
- Less specific but useful adjunct
6. Liver Parenchyma Changes
- Often inhomogeneous with markedly increased periportal echoes due to fibrosis
- Progressive liver enlargement
- Signs of portal hypertension in advanced/late cases: splenomegaly, ascites, reversal of portal venous flow
Combined Diagnostic Performance
The combination of triangular cord sign + gallbladder abnormalities is superior to either alone:
- Sensitivity: 95% (95% CI: 0.70-0.99)
- Specificity: 89% (95% CI: 0.79-0.94)
A negative triangular cord sign combined with normal gallbladder morphology has a high negative predictive value (>90%) for extrahepatic BA in infants up to 3 months with conjugated hyperbilirubinemia - Grainger & Allison's Diagnostic Radiology.
Standard USG Reporting Checklist for Suspected Biliary Atresia
When reporting a fasting USG in a neonate with conjugated jaundice, document all of the following:
- Liver - size, echogenicity, parenchymal texture, periportal echogenicity
- Porta hepatis / Triangular cord sign - presence/absence, thickness of EARPV (measure in mm)
- Gallbladder - present/absent; if present: length, wall characteristics (smooth vs. irregular), mucosal lining, response to feeding (motility)
- Common bile duct - visualized/not visualized; if seen, measure diameter
- Intrahepatic bile ducts - dilated or not (dilatation argues against BA)
- Hepatic artery - diameter at porta hepatis (>2 mm supports BA)
- Portal vein - direction of flow, any thrombosis
- Spleen - size (splenomegaly suggests portal hypertension or polysplenia syndrome)
- Associated anomalies - polysplenia, preduodenal portal vein, situs, IVC
Differential Diagnosis on USG
| Condition | Gallbladder | Bile ducts | Triangular cord |
|---|---|---|---|
| Biliary atresia | Absent/small/abnormal | NOT dilated | Present |
| Choledochal cyst | Normal | Dilated (cystic) | Absent |
| Neonatal hepatitis | Normal | Not dilated | Absent |
| Inspissated bile | May contain sludge/echogenic bile | May be mildly dilated | Absent |
Additional Investigations After USG
- Hepatobiliary scintigraphy (99mTc-HIDA/DISIDA): High sensitivity but false-positive rate >20%; non-excretion of radionuclide into bowel supports BA but not specific
- MRCP: 82% accurate, 90% sensitive, 77% specific; useful for anatomy
- Liver biopsy: Inflammatory cells + fibrotic parenchyma + bile neoductal structures = definitive diagnosis
- Intraoperative cholangiography: Definitive diagnosis; required to define surgical anatomy for Kasai portoenterostomy
Key clinical point: Kasai portoenterostomy performed before 8 weeks of age gives the best outcomes - approximately half of patients reach adolescence without needing transplant. Early USG diagnosis is therefore time-critical.
Sources: Grainger & Allison's Diagnostic Radiology | Sleisenger & Fordtran's Gastrointestinal and Liver Disease | Schwartz's Principles of Surgery, 11th ed. | Bailey & Love's Short Practice of Surgery, 28th ed. | AJR meta-analysis on triangular cord sign | Medscape Biliary Atresia Imaging
This is a shared conversation. Sign in to Orris to start your own chat.