BPH
Reading File
Finding Sources
Searching PubMed
"benign prostatic hyperplasia"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of Benign Prostatic Hyperplasia (BPH) drawn from authoritative medical textbooks.
Benign Prostatic Hyperplasia (BPH)
Definition
BPH is the non-malignant proliferation of both stromal and glandular elements of the prostate gland. A prostate volume exceeding 30 mL is the threshold definition, though the degree of enlargement correlates poorly with symptom severity. The gland can enlarge 3- to 5-fold, reaching 60-100 g or more.
- Goldman-Cecil Medicine, p. 1316
- Robbins & Kumar Basic Pathology, p. 659
Epidemiology
-
Affects ~50% of men over age 50 (histologically)
-
Rises to ~90% by the 8th decade
-
Of those with histologic BPH, approximately 50% develop clinically significant lower urinary tract symptoms (LUTS)
-
Prevalence increases linearly between ages 40-80
-
Goldman-Cecil Medicine, p. 1316
Pathogenesis
BPH originates in the periurethral transition zone (distinguishing it from prostate cancer, which arises in the peripheral zone).
Androgen-driven mechanism:
- Dihydrotestosterone (DHT) is the primary mediator - it is 10x more potent than testosterone
- DHT is synthesized from testosterone in the prostate by 5α-reductase type 2
- DHT binds nuclear androgen receptors and upregulates genes supporting stromal and glandular growth/survival
- DHT-induced growth factors increase stromal cell proliferation and decrease epithelial cell apoptosis
Role of estrogens:
- With aging, testosterone declines but estrogen levels remain stable or increase (via peripheral conversion)
- Estrogens act synergistically with DHT to drive growth of both epithelial and stromal cells (both express estrogen receptors)
Note: BPH does not occur in males castrated before puberty or in those with genetic disorders blocking androgen activity - confirming the androgen-dependence.
- Robbins & Kumar Basic Pathology, p. 659
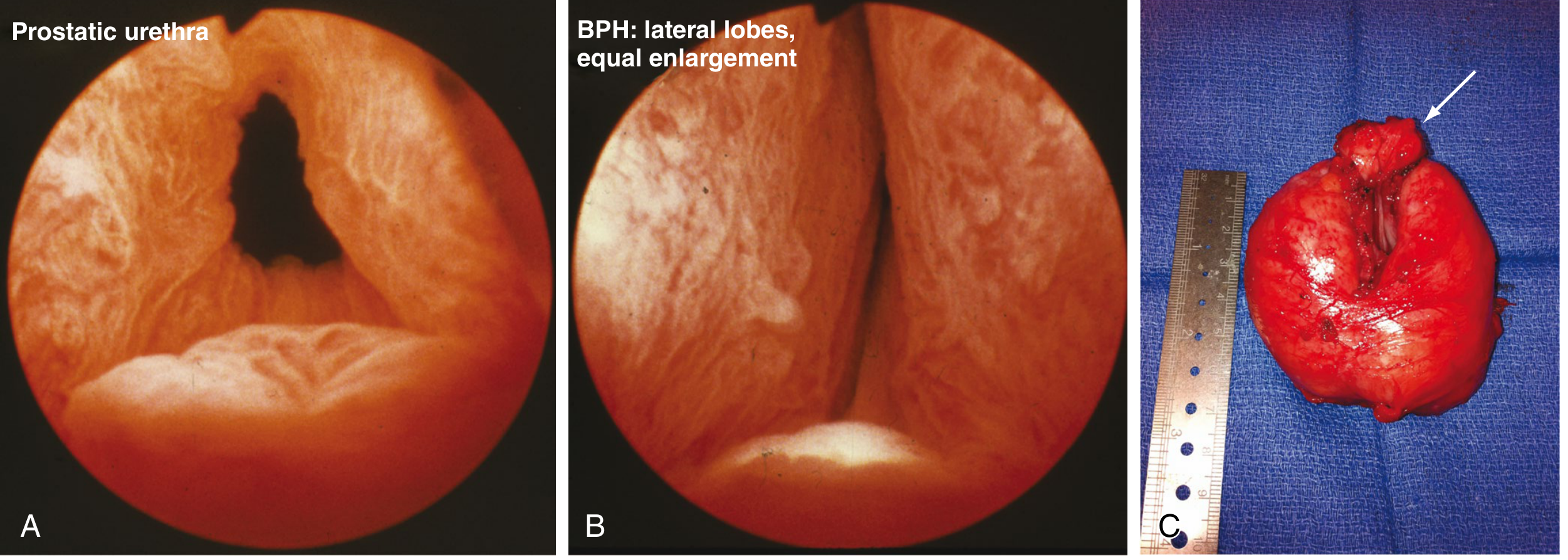
Morphology
Gross:
- Affects the transition zone, compressing the urethra to a slit-like orifice
- Hyperplastic nodules vary in color/consistency depending on cellular content
- May appear solid or contain cystic spaces (dilated glands)
Microscopic:
- Nodules composed of variable proportions of proliferating glandular elements and fibromuscular stroma
- Hyperplastic glands lined by two cell layers: tall columnar inner epithelial cells + peripheral flattened basal cells (key distinction from malignant glands, which lose the basal layer)
- Glandular lumina often contain corpora amylacea (laminated proteinaceous secretory material)
- Sabiston Textbook of Surgery, p. 2824
- Robbins & Kumar Basic Pathology, p. 659
Clinical Features
BPH causes bladder outlet obstruction (BOO) through two mechanisms:
- Mechanical - physical compression of the urethra by enlarged gland
- Dynamic - smooth muscle contraction in the prostatic stroma (alpha-1 adrenergic receptor-mediated)
LUTS are classified into three categories:
| Category | Symptoms |
|---|---|
| Storage (irritative) | Urgency, frequency, nocturia, urge incontinence |
| Voiding (obstructive) | Hesitancy, weak/intermittent stream, straining, prolonged voiding |
| Post-void | Incomplete emptying, terminal dribbling |
Complications:
-
Urinary retention (acute or chronic) - from complete obstruction
-
Recurrent UTI - residual urine acts as a culture medium
-
Bladder hypertrophy and distension
-
Hydronephrosis if untreated
-
Bladder calculi
-
Azotemia (elevated creatinine from back-pressure)
-
Sabiston Textbook of Surgery, p. 2824
Evaluation
- History and International Prostate Symptom Score (IPSS)
- Digital rectal exam (DRE) - assess prostate size and texture
- Urinalysis - rule out infection, hematuria
- PSA - in men with life expectancy >10 years (controversial; mainly to screen for concurrent prostate cancer)
- Post-void residual (PVR) - if >300 cc, indicates significant retention regardless of symptoms
- Uroflowmetry - assesses peak and average flow rates
- Cystoscopy and urodynamics - for refractory or complex cases
Management
AUA 2023 Guideline Algorithm
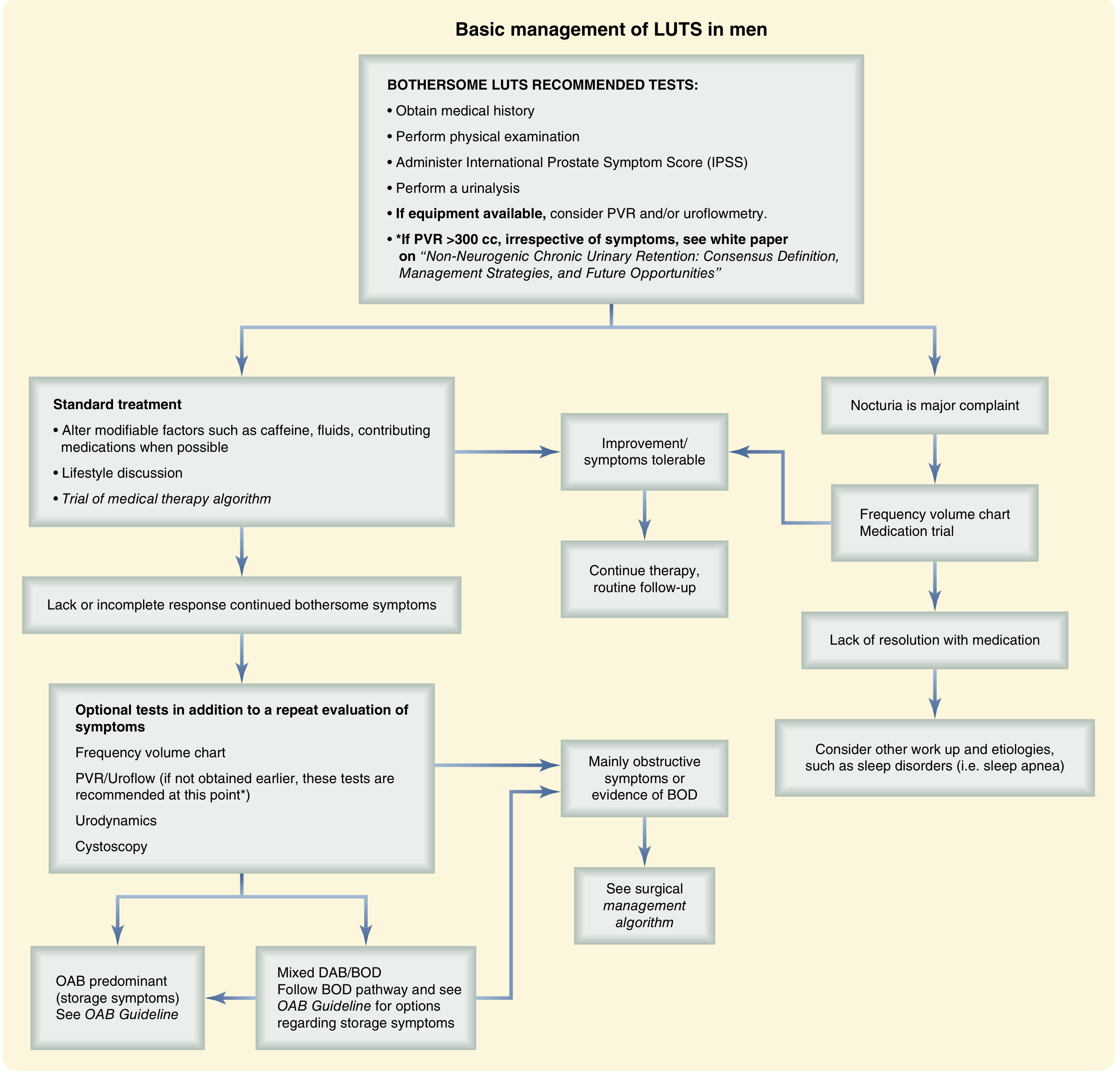
Step 1: Lifestyle/Behavioral Modifications (all patients)
- Fluid management (reduce caffeine, alcohol, evening fluids)
- Bladder training
- Manage contributing medications (e.g. diuretics)
Step 2: Medical Therapy
| Drug Class | Mechanism | Examples | Key Side Effects |
|---|---|---|---|
| α1-blockers | Relax smooth muscle in bladder neck and prostate (α1a selective) | Tamsulosin, Alfuzosin, Silodosin, Doxazosin | Orthostatic hypotension, retrograde ejaculation, rhinitis |
| 5α-reductase inhibitors (5-ARI) | Block testosterone → DHT conversion; reduce prostate volume over months | Finasteride (5-ARI type 2), Dutasteride (5-ARI type 1+2) | Reduces PSA ~50% (must adjust interpretation), sexual dysfunction |
| PDE5 inhibitors | Reduce smooth muscle tone via cGMP pathway | Tadalafil | Useful if concurrent ED |
| Combination therapy | α-blocker + 5-ARI | Superior to monotherapy for larger prostates |
Note: 5-ARIs reduce serum PSA by approximately 50% - this must be accounted for when using PSA for prostate cancer screening. Multiply measured PSA x2 when patient is on a 5-ARI.
Step 3: Surgical Indications
Surgery is indicated when medical therapy fails or when objective complications arise:
- Acute urinary retention
- Bladder calculi
- Azotemia / renal impairment
- Recurrent UTIs
- Recurrent hematuria
Surgical Options:
| Procedure | Notes |
|---|---|
| TURP (Transurethral Resection of the Prostate) | Gold standard; monopolar, bipolar, or laser variants |
| HoLEP (Holmium Laser Enucleation) | Excellent for large glands |
| ThuLEP (Thulium Laser Enucleation) | Similar to HoLEP |
| PVP (Photoselective Vaporization) | Laser vaporization |
| Open simple prostatectomy | For very large adenomas (>100g) |
| Minimally invasive (microwave, radiofrequency, HIFU) | Office-based; inferior long-term outcomes vs TURP |
TURP Complications:
-
Bleeding
-
TURP syndrome - dilutional hyponatremia from glycine absorption (monopolar only; eliminated with bipolar/laser using saline irrigation)
-
UTI
-
Urinary incontinence
-
Urethral stricture
-
Retrograde ejaculation
-
Sabiston Textbook of Surgery, p. 2824-2825
-
Goldman-Cecil Medicine, p. 1318
Key Distinctions: BPH vs Prostate Cancer
| Feature | BPH | Prostate Cancer |
|---|---|---|
| Zone affected | Transition zone | Peripheral zone |
| Histology | Two cell layers (columnar + basal) | Loss of basal cell layer |
| DRE | Smooth, symmetric enlargement | Hard, irregular nodule |
| Malignant potential | None (not premalignant) | N/A |
| PSA elevation | Mild, proportional to size | Often disproportionately high |
- Robbins & Kumar Basic Pathology, p. 659
This is a shared conversation. Sign in to Orris to start your own chat.