Hypoplastic left heart syndrome at 16 weeks
Reading File
Finding Sources
Searching PubMed
"hypoplastic left heart syndrome"[MeSH Terms] AND "prenatal diagnosis"[MeSH Terms]
Searching the Web
hypoplastic left heart syndrome 16 weeks prenatal diagnosis ultrasound findings management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a thorough response. Here is the full answer:
Hypoplastic Left Heart Syndrome (HLHS) at 16 Weeks
What Is HLHS?
HLHS is a heterogeneous spectrum of cardiac malformations characterized by varying degrees of underdevelopment of all left-sided structures - the left ventricle (LV), mitral valve, aortic valve, and ascending aorta. The defining feature is a left heart that is incapable of sustaining systemic cardiac output. Prevalence is approximately 0.2 per 1000 live births, and it occurs roughly twice as often in males. Left untreated, it is uniformly fatal and accounts for ~25% of all early neonatal cardiac deaths.
- Schwartz's Principles of Surgery, 11th Ed.
Anatomic Subtypes (Valvular Classification)
| Subtype | Features |
|---|---|
| Aortic stenosis + mitral stenosis | Some residual LV; may have forward flow |
| Aortic atresia + mitral atresia | Most severe; near-absent LV; ascending aorta < 2 mm |
| Aortic atresia + mitral stenosis | Intermediate severity |
| Aortic stenosis + mitral atresia | VSD often present (allows some LV filling) |
Associated features in virtually all cases:
- Hypoplastic ascending aorta (more severe with aortic atresia)
- Coarctation shelf in ~80% of patients
- Large ductus arteriosus and main pulmonary artery
- Restricted interatrial foramen ovale (in ~22% of HLHS cases - a critical prognostic finding)
- Small segmental pulmonary arteries (from reduced intrauterine pulmonary blood flow)
Diagnosis at 16 Weeks
HLHS can be detected as early as 11-14 weeks on fetal echocardiography, though it is more commonly diagnosed at the standard 18-22 week anomaly scan. Diagnosis at 16 weeks is entirely feasible - the University of Michigan Fetal Heart Program specifically notes echocardiographic diagnosis of HLHS as early as 16 weeks gestation.
Some cases begin as severe aortic stenosis in the first trimester, which then evolves into full HLHS by mid-gestation or term. This means that a fetus diagnosed with critical aortic stenosis at 16 weeks may not yet show the full HLHS picture - serial surveillance is required.
Key Ultrasound / Echocardiographic Findings
Four-chamber view (4CV) - the primary screening view:
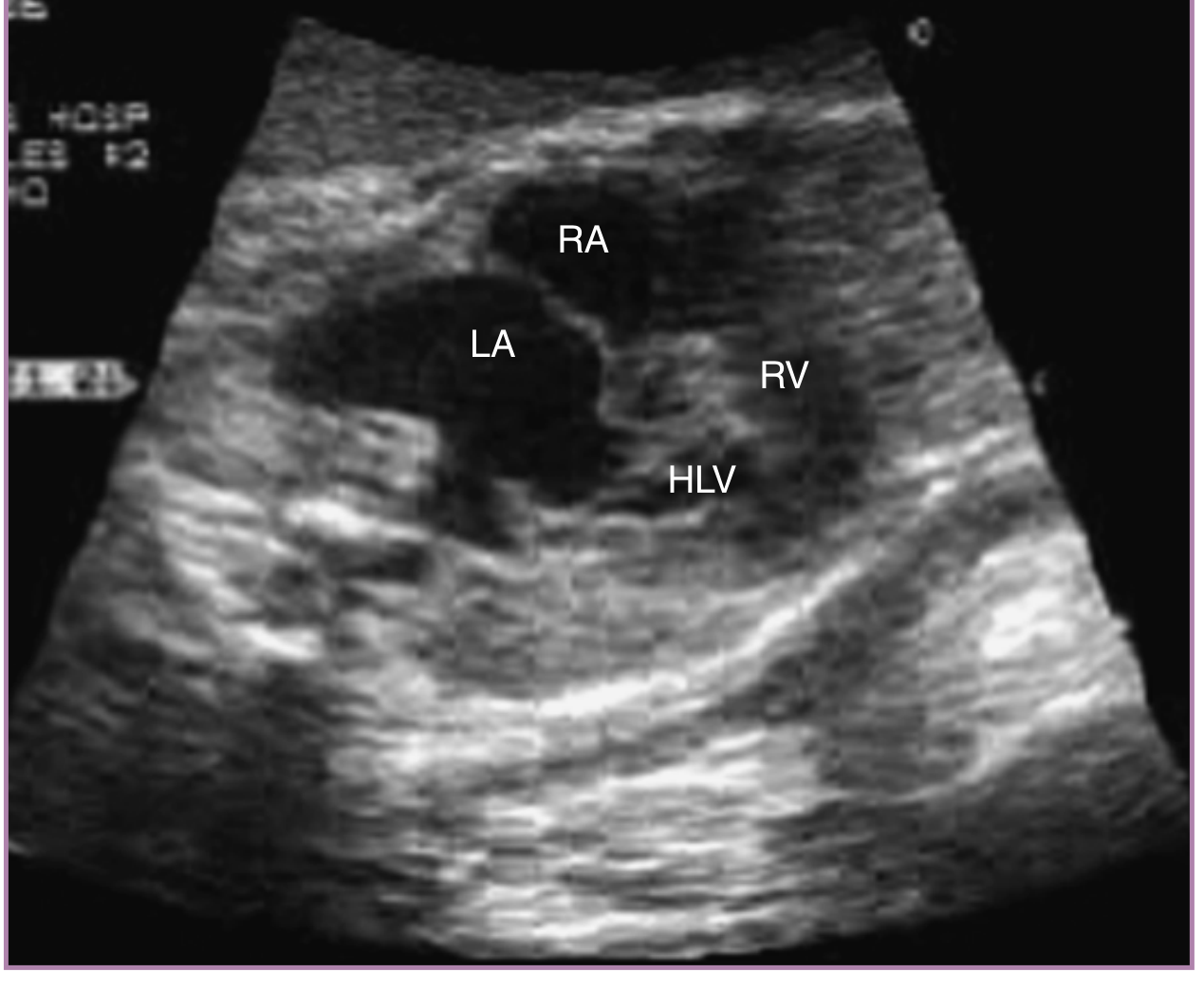
Fetal echo (four-chamber view): HLHS with restrictive foramen ovale. Note the markedly small HLV (hypoplastic left ventricle) compared to the dominant RV. The dilated LA and pulmonary veins indicate left atrial hypertension from impaired egress. - Creasy & Resnik's Maternal-Fetal Medicine
| Finding | Significance |
|---|---|
| Severely hypoplastic or absent LV | Hallmark of HLHS |
| No or restricted inflow across mitral valve | Mitral atresia/stenosis |
| Intact or near-intact ventricular septum | Typical; VSD presence alters subtype |
| Restrictive / bowing foramen ovale | Negative prognostic sign - leads to pulmonary venous congestion and irreversible pulmonary vascular disease |
| Dilated LA and pulmonary veins | Consequence of restricted foramen ovale |
| Retrograde flow in aortic arch | Aortic arch filled from ductus in retrograde manner - confirmatory with color Doppler |
| Dominant RV with right ventricular hypertrophy | Compensatory right-sided dominance |
| Tricuspid regurgitation | Indicates RV dysfunction; prognostically important |
- Creasy & Resnik's Maternal-Fetal Medicine
Associated Abnormalities
- Increased risk of chromosomal aneuploidy - karyotype / chromosomal microarray recommended at diagnosis
- Increased risk of congenital or acquired CNS abnormalities (neurodevelopmental delay is common in survivors)
- Shone syndrome (multiple left-sided obstructive lesions) can mimic HLHS but may be amenable to biventricular repair - distinction is clinically important but sometimes very subtle
Fetal Counseling at 16 Weeks
Parents must receive detailed information about the diagnosis, prognosis, and all available pathways. Key points:
- Termination of pregnancy - Up to ~48% of pregnancies are terminated following a prenatal diagnosis of HLHS. Parents need strong emotional and multidisciplinary support.
- Palliative surgical pathway - Three-stage staged palliation (Norwood → Glenn → Fontan), all at a tertiary center. This is not a cure.
- Cardiac transplantation - An alternative to staged palliation; limited by donor availability.
- Comfort/palliative care only - Some families choose this pathway; it results in neonatal death.
Early prenatal diagnosis (including at 16 weeks) has been associated with reduced neonatal mortality and less postnatal brain injury, likely due to optimized perinatal planning (prostaglandin E1 started immediately after birth to maintain ductal patency, delivery at a specialized center).
Fetal Interventions (Select Cases)
In fetuses with critical aortic stenosis evolving toward HLHS, in-utero fetal aortic valvuloplasty (FAV) may be considered to preserve biventricular circulation. Published series from Boston Children's Hospital:
- Technical success in ~77-83% of attempted procedures
- ~38% achieved biventricular circulation (vs. univentricular palliation)
- Survival at 1 year: 80% ± 4%; at 5 years: 75% ± 5%
- Intraprocedural complications occur in ~48% (fetal bradycardia, pericardial/pleural effusion, balloon rupture)
- Fetal death within 2 days of procedure: ~16.7%
- Multiple cardiac punctures (needed in 25%) increase complication risk
For HLHS with restrictive or intact atrial septum, fetal atrial septostomy may be considered to relieve left atrial hypertension and prevent pulmonary vascular disease.
- Creasy & Resnik's Maternal-Fetal Medicine
Postnatal Surgical Palliation (Three-Stage Norwood Pathway)
Stage I - Modified Norwood Procedure (within first week of life)
- Creates a neoaorta arising from the RV by connecting pulmonary root + native ascending aorta + homograft patch
- Pulmonary blood flow provided via either:
- Modified Blalock-Taussig shunt (mBTS) from innominate artery to right pulmonary artery
- Sano shunt (RV-PA conduit, 5-6 mm Gore-Tex graft) - SVR trial showed 74% vs 64% transplantation-free survival at 12 months favoring Sano, though more unintended interventions
- Interatrial septum is widely excised (prevents pulmonary venous hypertension)
- Postoperative management requires careful balancing of pulmonary vs. systemic perfusion
Stage II - Glenn Procedure (~6 months of age)
- Bidirectional cavopulmonary anastomosis (superior vena cava to right pulmonary artery)
- Reduces volume overload on the single (right) ventricle
Stage III - Fontan Procedure (~2-3 years of age)
- Total cavopulmonary connection - inferior vena cava flow directed to pulmonary arteries
- Separates pulmonary and systemic circulations
Prognosis
| Timepoint | Outcome |
|---|---|
| 5-year survival (best/largest centers) | ≥80% |
| Long-term | Incomplete data; outcomes still evolving |
| Neurodevelopment | Many survivors have some degree of delay |
| Adults | Progressive right heart failure; may require cardiac transplantation |
| Risk of liver dysfunction from abnormal venous physiology |
Key Management Summary for 16-Week Diagnosis
- Refer to tertiary/quaternary fetal cardiac unit immediately for detailed fetal echocardiography
- Assess foramen ovale with 2D + color Doppler (restriction = poor prognosis, may need planned cesarean + immediate intervention)
- Chromosomal microarray / karyotype (aneuploidy risk elevated)
- Multidisciplinary counseling - maternal-fetal medicine, pediatric cardiology, neonatology, cardiac surgery, genetics, social work
- Serial surveillance - some aortic stenosis cases evolve to full HLHS; others may stabilize
- Discuss all options - surgical palliation, transplantation, comfort care, and (where applicable) fetal intervention
- Plan delivery at a center with immediate neonatal cardiac surgery capabilities
- Prostaglandin E1 initiated immediately after birth to maintain ductal patency before Stage I Norwood
Sources:
- Creasy & Resnik's Maternal-Fetal Medicine - primary prenatal reference
- Schwartz's Principles of Surgery, 11th Ed. - surgical treatment
- Medscape: HLHS Clinical Presentation - prenatal diagnosis statistics
- EACTS/AEPC Guidelines for HLHS management (2020) - Alphonso N et al., Eur J Cardiothorac Surg
This is a shared conversation. Sign in to Orris to start your own chat.