Difference between Immunofixation and electrophoresis
Reading File
Searching the Web
immunofixation vs protein electrophoresis difference clinical use
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a thorough comparison, backed by Harrison's and Goldman-Cecil Medicine:
Protein Electrophoresis vs. Immunofixation Electrophoresis (IFE)
The Diagnostic Figure
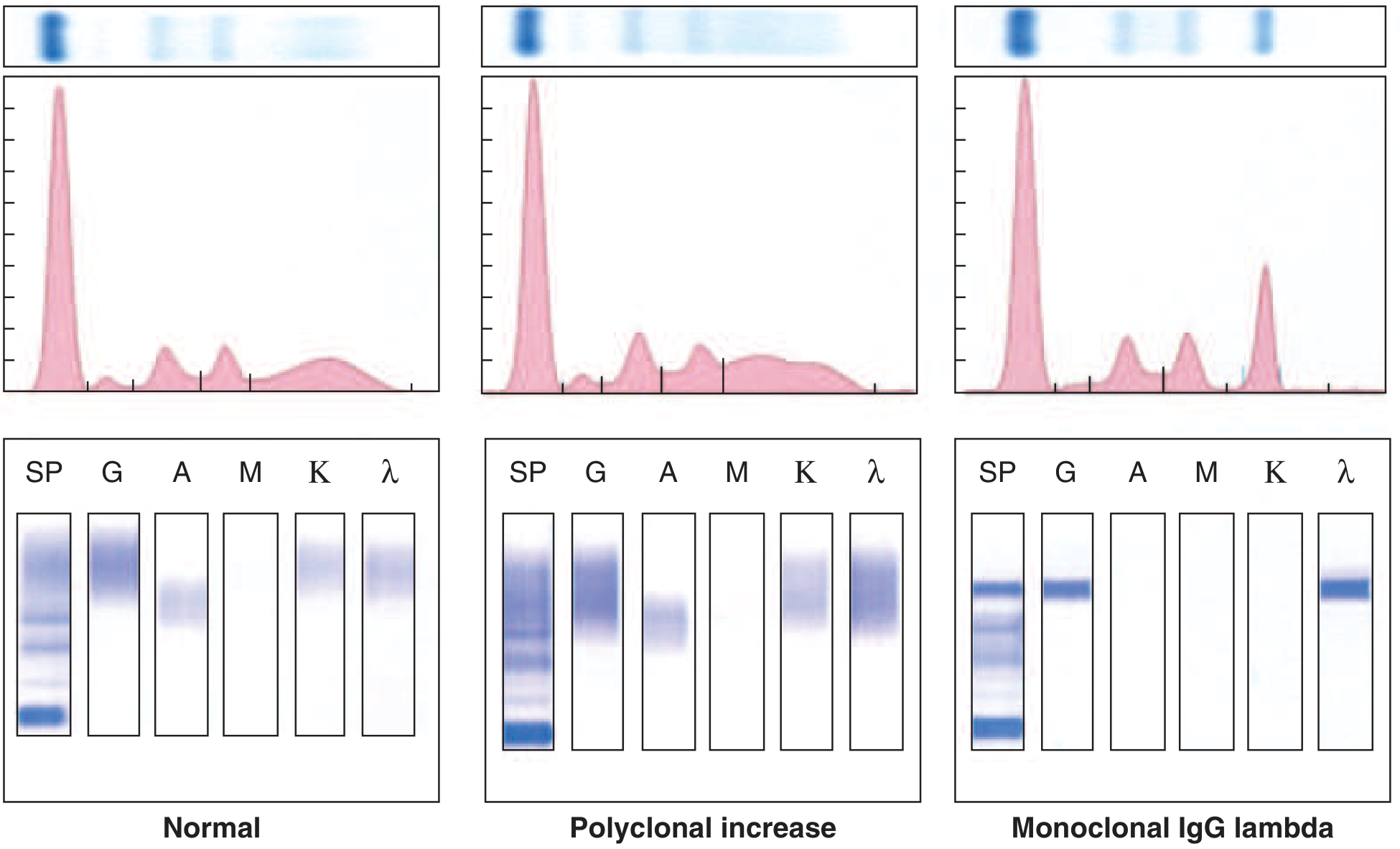
Top row: agarose gel. Middle row: densitometric tracing. Bottom row: immunofixation panels (SP, G, A, M, K, λ lanes).
Side-by-Side Comparison
| Feature | Protein Electrophoresis (SPEP/UPEP) | Immunofixation Electrophoresis (IFE) |
|---|---|---|
| Purpose | Screen/detect and quantify protein fractions | Confirm and identify the specific M protein type |
| Principle | Separates proteins by charge and size in an electric field into bands (albumin, α1, α2, β, γ) | After electrophoresis, specific antisera to IgG, IgA, IgM, kappa, lambda are applied to precipitate and identify the protein |
| What it shows | A narrow "church spire" peak or dense discrete band in the γ region suggests an M protein | Identifies the exact heavy chain class (IgG, IgA, IgM, IgD, IgE) AND light chain type (κ or λ) |
| Sensitivity | Lower - can miss small M proteins | Higher - detects small, unmeasurable M proteins missed on electrophoresis |
| Specificity | Lower - cannot characterize the protein type | Higher - definitive characterization of M protein isotype |
| Quantitation | Yes - can measure the size of the M spike (g/dL) | No - not used for quantitation |
| Role | Screening + monitoring (size of M protein over time) | Diagnosis/confirmation |
| When to use IFE | Always alongside electrophoresis when myeloma is first suspected | After any abnormal peak/band on SPEP; also when electrophoresis is negative but suspicion remains high |
Key Points from Textbooks
Electrophoresis (SPEP):
- Detects M protein as a narrow "church spire" peak on the densitometer or a dense discrete band on agarose gel
- Allows quantitation of the M protein spike - important for monitoring response to treatment
- Monoclonal free light chains (Bence Jones proteins) are rarely seen on serum electrophoresis but are easily detected on urine electrophoresis (UPEP)
- UPEP requires a 24-hour urine collection
Immunofixation (IFE):
- After separating proteins, monospecific antisera are applied against IgG (G), IgA (A), IgM (M), kappa (K), and lambda (λ) - each in its own lane
- A monoclonal protein produces a discrete, sharp band in the corresponding lane (e.g., both the G lane and λ lane light up = IgG lambda myeloma)
- Normal/polyclonal increases produce no discrete bands (just diffuse smearing)
- Particularly important in:
- Oligosecretory myeloma
- Primary (AL) amyloidosis
- Solitary plasmacytoma
- After treatment of myeloma/macroglobulinemia - to confirm complete response
Why both are ordered together:
"Immunofixation should always be performed in conjunction with electrophoresis when multiple myeloma or related disorders are first suspected so as to detect small, unmeasurable M proteins that may be missed on electrophoresis."
- Goldman-Cecil Medicine
Clinical Workflow
Suspicion of plasma cell disorder
↓
SPEP + UPEP (screen)
↙ ↘
Abnormal peak Normal but high suspicion
↓ ↓
IFE ←————————————————→ IFE still indicated
↓
Identifies: IgG κ? IgA λ? Free light chain only?
↓
Confirms diagnosis (myeloma, MGUS, amyloidosis, etc.)
↓
Follow-up: SPEP for quantitative monitoring of M-spike
Summary in One Line
Electrophoresis = screening + quantitation. Immunofixation = characterization + confirmation. They are complementary tests, not alternatives. IFE is more sensitive, while SPEP is better for tracking M protein size over time.
- Harrison's Principles of Internal Medicine 22E, Fig. 116-2
- Goldman-Cecil Medicine, Chapter 173: Plasma Cell Disorders
Multiple myeloma tretament
Finding Sources
Searching PubMed
"multiple myeloma" AND treatment
Finding Sources
Reading Article
PMID: 40340857
Finding Sources
Searching the Web
multiple myeloma treatment 2025 NCCN guidelines daratumumab VRd
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of multiple myeloma treatment based on Harrison's 22E (2025) and Goldman-Cecil Medicine:
Multiple Myeloma: Treatment
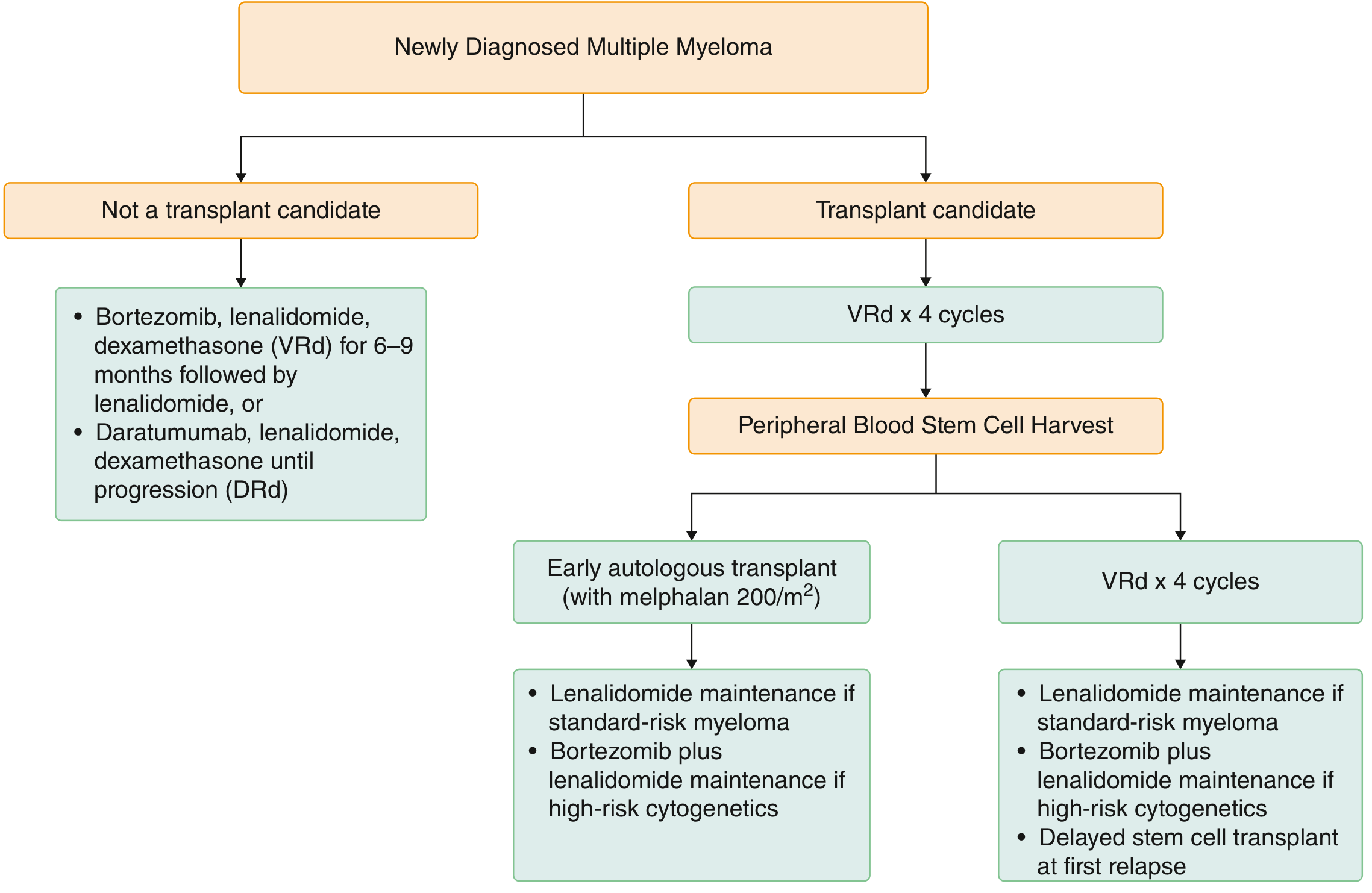
Treatment Algorithm
Step 1: Determine Transplant Eligibility
The first and most critical step in management is determining whether the patient is eligible for autologous stem cell transplantation (ASCT). Eligibility is based on:
- Physiologic age (<65-70 years is a rough cut-off)
- Good performance status (ECOG 0-2)
- Absence of significant cardiopulmonary or other comorbidities
A. Transplant-Eligible Patients (~50% of newly diagnosed)
1. Induction Therapy (3-4 months)
Standard: VRd (bortezomib + lenalidomide + dexamethasone)
- Bortezomib 1.3 mg/m² SC days 1, 8, 15; Lenalidomide 25 mg oral days 1-14; Dexamethasone 20-40 mg
Alternatives:
- DVRd (Daratumumab + VRd) - particularly favored in high-risk disease
- DRd (Daratumumab + lenalidomide + dexamethasone)
- VCd/CyBorD (Bortezomib + cyclophosphamide + dexamethasone) - especially if renal failure
2. Stem Cell Collection
- Granulocyte colony-stimulating factor (G-CSF) +/- plerixafor or cyclophosphamide
- Collect within 6 months if patient is on lenalidomide (prolonged use compromises stem cell yield)
3. Autologous Stem Cell Transplant (ASCT)
- Conditioning: Melphalan 200 mg/m² (high-dose) followed by infusion of peripheral blood stem cells
- Mortality very low (<1%)
- Not curative but prolongs event-free and overall survival
- Early vs. Delayed ASCT: In standard-risk patients, delaying transplant until first relapse (with stem cells cryopreserved) is an acceptable alternative
4. Maintenance Therapy (post-ASCT)
- Standard-risk: Lenalidomide monotherapy (prolongs PFS and OS)
- High-risk cytogenetics [del17p, t(4;14), t(14;16)]: Bortezomib + lenalidomide combination maintenance, or daratumumab post-ASCT
B. Transplant-Ineligible Patients (~50%)
Standard options:
| Regimen | Notes |
|---|---|
| VRd x 6-9 months → lenalidomide maintenance | Most commonly used |
| DRd (Daratumumab + Rd) until progression | High ORR of 93%, CR 47% |
| RVD-lite (modified low-dose VRd) | For elderly/frail patients |
| VCd (Bortezomib + Cy + Dex) | If lenalidomide unavailable or severe renal failure |
| IRd (Ixazomib + Rd) | All-oral; for high-risk patients without IV access |
MP (melphalan + prednisone) combinations are no longer standard given availability of newer agents.
C. High-Risk Smoldering Myeloma
- Low/intermediate-risk: Observation every 3-4 months only
- High-risk (≥2 of: M-protein >2 g/dL, FLC ratio >20, BM plasma cells >20%): Lenalidomide 25 mg days 1-21 per 28-day cycle x ~2 years; reduces progression to symptomatic myeloma and overall mortality
Key Drug Classes
| Class | Agents | Key Side Effects |
|---|---|---|
| IMiDs (Immunomodulatory) | Thalidomide, Lenalidomide, Pomalidomide | DVT (requires antithrombotic prophylaxis), teratogenicity, cytopenias |
| Proteasome Inhibitors (PI) | Bortezomib (V), Carfilzomib (K), Ixazomib (I) | Peripheral neuropathy (bortezomib), cardiac toxicity (carfilzomib) |
| Anti-CD38 antibodies | Daratumumab, Isatuximab | Infusion reactions, infections, interfere with cross-matching |
| Anti-SLAMF7 | Elotuzumab | Infusion reactions |
| BCMA-targeted | Belantamab mafodotin, Ide-cel (CAR-T), Cilta-cel (CAR-T), Teclistamab (bispecific Ab) | Ocular toxicity (belantamab), CRS, neurotoxicity (CAR-T) |
| BCL-2 inhibitor | Venetoclax | Only for t(11;14) subtype |
| XPO1 inhibitor | Selinexor | Fatigue, nausea, cytopenias |
Important: Acyclovir prophylaxis is mandatory in all patients receiving bortezomib (herpes zoster reactivation risk). DVT prophylaxis (aspirin or anticoagulant) required with all IMiD-containing regimens.
D. Relapsed/Refractory Myeloma
- Goal: choose a regimen with 2+ agents the patient has not previously received or to which disease is not refractory
- If relapse >6 months after stopping therapy: reintroduction of initial regimen is reasonable
- If delayed ASCT planned: perform ASCT at first relapse
- Second ASCT: considered if first remission lasted >18 months (no maintenance) or >36 months (with maintenance)
Newer options for later-line RRMM:
- CAR-T therapy: Idecabtagene vicleucel (ide-cel) and Ciltacabtagene autoleucel (cilta-cel) - both target BCMA
- Bispecific antibodies: Teclistamab, elranatamab, talquetamab
- Pomalidomide-based regimens: Effective even in lenalidomide-refractory disease
- Carfilzomib (KRd): Effective in bortezomib-refractory disease
- Venetoclax: Exclusively for t(11;14) myeloma
A recent meta-analysis (PMID 39551604) showed that CAR-T and bispecific antibodies have comparable efficacy in third-line or later MM, though CAR-T may offer deeper responses.
E. Supportive Care / Complication Management
| Complication | Management |
|---|---|
| Bone disease/pain | Zoledronic acid or pamidronate (bisphosphonates); palliative RT 20-30 Gy for focal, chemo-refractory pain or spinal cord compression |
| Hypercalcemia | IV hydration + steroids + bisphosphonates |
| Renal failure (cast nephropathy) | Aggressive hydration, furosemide to maintain urine output 100 mL/hr; plasmapheresis x5 days if FLC >150 mg/dL; VCd or Dara-VCd for myeloma control |
| Infections | TMP-SMX prophylaxis with high-dose steroids; acyclovir with bortezomib; IVIG reserved for hypogammaglobulinemia + recurrent infections |
| Anemia | Erythropoiesis-stimulating agents; treat underlying disease |
Response Assessment
Responses are graded by International Myeloma Working Group (IMWG) criteria:
- sCR (stringent CR), CR, VGPR (very good partial response), PR (partial response)
- Minimal Residual Disease (MRD) negativity is associated with better survival outcomes, though therapy is not routinely changed based on MRD status alone
"NCCN Guidelines for Multiple Myeloma, Version 1.2025 (PMID 40340857)" - updates include new systemic therapy recommendations for both newly diagnosed and relapsed/refractory MM.
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 116
- Goldman-Cecil Medicine, Chapter 173: Plasma Cell Disorders
What is VTD therapy
Finding Sources
Searching the Web
VTD regimen bortezomib thalidomide dexamethasone multiple myeloma induction
Finding Sources
Reading Web Page
https://www.chemoexperts.com/vtd.html
Reading File
Reading File
Here is a complete breakdown of VTD therapy:
VTD (Bortezomib + Thalidomide + Dexamethasone)
V = Velcade (Bortezomib) - Proteasome Inhibitor
T = Thalidomide - Immunomodulatory drug (IMiD)
D = Dexamethasone - Corticosteroid
Mechanism of Action
| Drug | Class | How It Works |
|---|---|---|
| Bortezomib | Proteasome inhibitor | Blocks the 26S proteasome, causing accumulation of misfolded proteins → myeloma cell apoptosis |
| Thalidomide | IMiD (1st generation) | Enhances T-cell and NK-cell activity, inhibits pro-survival cytokines (TNF-α, IL-6, VEGF), anti-angiogenic |
| Dexamethasone | Corticosteroid | Directly induces apoptosis in myeloma cells; enhances activity of partner drugs |
Indication
Newly diagnosed multiple myeloma (NDMM) - primarily as pre-transplant induction therapy in transplant-eligible patients.
Standard Dosing Schedule (21-day cycles)
| Drug | Dose | Route | Days |
|---|---|---|---|
| Bortezomib | 1.3 mg/m² | SC or IV | Days 1, 4, 8, 11 (or weekly: days 1, 8, 15) |
| Thalidomide | 100-200 mg | Oral (at bedtime) | Days 1-21 (continuous) |
| Dexamethasone | 40 mg | Oral | Days 1-4, 9-12 (or on bortezomib days) |
- Typically 4-6 cycles are given before proceeding to stem cell transplant
- Bortezomib is preferably given subcutaneously (SC) rather than IV to reduce peripheral neuropathy risk
Clinical Evidence
Two pivotal phase III trials established VTD's superiority:
- Cavo et al., Lancet 2010 - VTD vs. TD (thalidomide + dexamethasone) before and after double ASCT: VTD achieved significantly higher CR rates
- Rosinol et al. (PETHEMA/GEM), Blood 2012 - VTD superior to VCD and TD as pre-transplant induction; higher rates of CR + VGPR
VTD achieves >90% overall response rate, which is comparable to VRd.
VTD vs. VRd - Key Differences
| Feature | VTD | VRd |
|---|---|---|
| IMiD used | Thalidomide (older, 1st gen) | Lenalidomide (newer, 2nd gen) |
| Neuropathy risk | Higher (both drugs are neurotoxic) | Lower |
| DVT risk | High (thalidomide) | High (lenalidomide) |
| Cost/availability | Thalidomide cheaper, wider availability | Lenalidomide more expensive |
| Stem cell mobilization | Does not impair | Lenalidomide may impair if used >6 months |
| Current preference | Less preferred in high-income settings | Preferred standard in most guidelines |
| Special use | Still used in Europe and resource-limited settings | Standard in US/NCCN guidelines |
"Other similar three-drug combinations (bortezomib, thalidomide, and dexamethasone or bortezomib, cyclophosphamide, and dexamethasone) also achieve >90% response rate." - Harrison's Principles of Internal Medicine 22E
Key Side Effects
| Drug | Main Toxicities |
|---|---|
| Bortezomib | Peripheral neuropathy, fatigue, GI symptoms, herpes zoster reactivation |
| Thalidomide | Peripheral neuropathy (cumulative, dose-dependent), DVT, sedation, constipation, teratogenicity |
| Dexamethasone | Hyperglycemia, infections, insomnia, mood changes, osteoporosis |
Mandatory prophylaxis with VTD:
- Antithrombotic (aspirin or low-molecular-weight heparin) - DVT risk from thalidomide
- Acyclovir - herpes zoster reactivation risk from bortezomib
- Thalidomide is teratogenic - strict pregnancy prevention program (STEPS program) required
DVTd Variant
A 4-drug variant, DVTd (Daratumumab + VTD), was studied in the CASSIOPEIA trial (Moreau et al., Lancet 2019) and showed that adding daratumumab to VTD before and after ASCT significantly improved stringent CR rates and MRD negativity compared to VTD alone. DVTd has become a standard option in transplant-eligible patients in Europe.
Summary
VTD is an effective, well-established induction regimen for transplant-eligible newly diagnosed multiple myeloma. It is gradually being replaced by VRd (which uses the better-tolerated lenalidomide instead of thalidomide) in most Western guidelines, but remains widely used globally, particularly in Europe and in settings where lenalidomide is unavailable. The addition of daratumumab to form DVTd represents the next evolution of this backbone.
- Harrison's Principles of Internal Medicine 22E, Chapter 116
- Goldman-Cecil Medicine, Chapter 173 (ref A4: CASSIOPEIA trial)
What so HDT?
Finding Sources
Reading File
HDT - High-Dose Therapy in Multiple Myeloma
HDT stands for High-Dose Therapy, and in myeloma it specifically means high-dose melphalan (HDM) at 200 mg/m² used as myeloablative conditioning, immediately followed by Autologous Stem Cell Transplantation (ASCT) to rescue the bone marrow. The full process is called HDT-ASCT.
Why It's Done
Standard-dose chemotherapy alone cannot eradicate enough myeloma cells. HDT uses a dose of melphalan high enough to destroy virtually all bone marrow cells (including myeloma cells), but this dose also ablates normal blood cell production - so pre-harvested stem cells are infused back to "rescue" and regenerate the bone marrow.
The HDT-ASCT Process Step by Step
Induction (VRd / VTD / DVRd x 3-6 cycles)
↓
Stem Cell Mobilization
(G-CSF ± plerixafor or cyclophosphamide)
↓
Peripheral Blood Stem Cell Harvest
(collect enough for 1-2 transplants)
↓
HDT: Melphalan 200 mg/m² IV
(conditioning/myeloablative chemotherapy)
↓
ASCT: Infusion of stored stem cells (Day 0)
↓
Engraftment (typically Day +10 to +14)
↓
Maintenance therapy (lenalidomide ± bortezomib)
Key Facts
| Feature | Detail |
|---|---|
| Conditioning drug | Melphalan 200 mg/m² |
| Stem cell source | Autologous (patient's own) peripheral blood |
| Mortality | Very low (<1%) in eligible patients |
| Effect | 25-40% additional complete responses (CRs) beyond induction alone |
| Curative? | No - prolongs event-free and overall survival but rarely cures |
| Timing | Early (after induction) OR delayed (at first relapse) - both are valid |
| Tandem transplant | 2nd HDT-ASCT only beneficial if 1st failed to achieve CR/VGPR |
"Randomized studies comparing standard-dose therapy to high-dose melphalan therapy with hematopoietic stem cell support have shown that HDT can achieve higher overall response rates, with up to 25-40% additional CRs and prolonged progression-free and overall survival; however, few, if any, patients are cured." - Harrison's Principles of Internal Medicine 22E
Who is Eligible?
| Eligible | Not Eligible |
|---|---|
| Age <65-70 years (physiologic) | Age >70 years or frail |
| Good performance status (ECOG 0-2) | Poor performance status |
| Adequate organ function | Significant cardiopulmonary disease |
| No significant comorbidities | Severe renal failure, liver disease |
Early vs. Delayed HDT-ASCT
- Early: Proceed to ASCT right after induction - preferred because it is convenient, avoids prolonged chemotherapy, and achieves deep early response
- Delayed: Collect and cryopreserve stem cells after induction, continue therapy, perform ASCT at first relapse - acceptable option in standard-risk patients. Randomized trials showed no significant difference in overall survival between the two approaches.
Maintenance After HDT-ASCT
| Risk Group | Maintenance |
|---|---|
| Standard-risk | Lenalidomide monotherapy (indefinitely or until progression) |
| High-risk cytogenetics [del17p, t(4;14), t(14;16)] | Bortezomib + lenalidomide combination, or daratumumab |
Lenalidomide maintenance post-HDT improves both PFS and OS, though it carries a small increased risk of second primary malignancies - the benefit far outweighs this risk.
Allogeneic Transplant?
Allogeneic transplantation (using a donor's stem cells) can exploit a graft-versus-myeloma effect but carries significant toxicity. It is very rarely used today, and only within clinical trials, due to the availability of more effective and safer cellular therapies (CAR-T, bispecific antibodies).
- Harrison's Principles of Internal Medicine 22E, Chapter 116
This is a shared conversation. Sign in to Orris to start your own chat.