Make notes of migraine for mbbs exam refrence from kd Tripathi
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
I now have more than enough comprehensive content to write complete MBBS-level migraine notes in the style of KD Tripathi. Let me now compile these into well-structured exam notes.
MIGRAINE - MBBS Exam Notes
(Based on standard pharmacology & medicine references - KD Tripathi style)
DEFINITION
Migraine is a primary headache disorder characterized by recurrent attacks of moderate to severe, often unilateral, throbbing headache lasting 4-72 hours, frequently accompanied by nausea, vomiting, photophobia, and phonophobia.
EPIDEMIOLOGY
- Affects ~16% of the population (2nd most common primary headache after tension-type)
- Female > Male (3:1) - hormonal influence
- Strong genetic/familial predisposition
- Onset usually in adolescence or early adulthood
CLASSIFICATION (ICHD-3)
| Type | Feature |
|---|---|
| Migraine without aura ("Common migraine") | Most common (~80%). No premonitory neurological symptoms |
| Migraine with aura ("Classic migraine") | Preceded by transient focal neurological symptoms (aura) |
| Chronic migraine | ≥15 headache days/month for >3 months |
| Menstrual migraine | Linked to menstrual cycle (estrogen withdrawal) |
| Vestibular migraine | Vertigo as a prominent feature |
| Status migrainosus | Attack lasting >72 hours |
PHASES OF A MIGRAINE ATTACK
1. Prodrome (hours to days before)
- Mood changes (depression/euphoria), food cravings, yawning, fatigue, neck stiffness
2. Aura (20-60 minutes, reversible)
- Visual (most common): scintillating scotoma, fortification spectra, homonymous hemianopia
- Sensory: unilateral paresthesias/numbness spreading in "march" pattern
- Speech: dysphasia
- Motor: weakness (hemiplegic migraine)
- Mechanism: Cortical Spreading Depression (CSD) - a wave of neuronal depolarization followed by sustained suppression, moving at 3-5 mm/min across cortex, triggering aura symptoms
3. Headache Phase (4-72 hours)
- Unilateral (60%), throbbing/pulsating
- Moderate to severe intensity
- Worsened by physical activity
- Associated with: nausea, vomiting, photophobia, phonophobia, osmophobia
- Associated with cerebral vasodilation and lower-than-normal serotonin levels
4. Postdrome
- Fatigue, difficulty concentrating ("migraine hangover"), lasting hours to a day
PATHOPHYSIOLOGY
Trigeminovascular Theory (Most accepted)
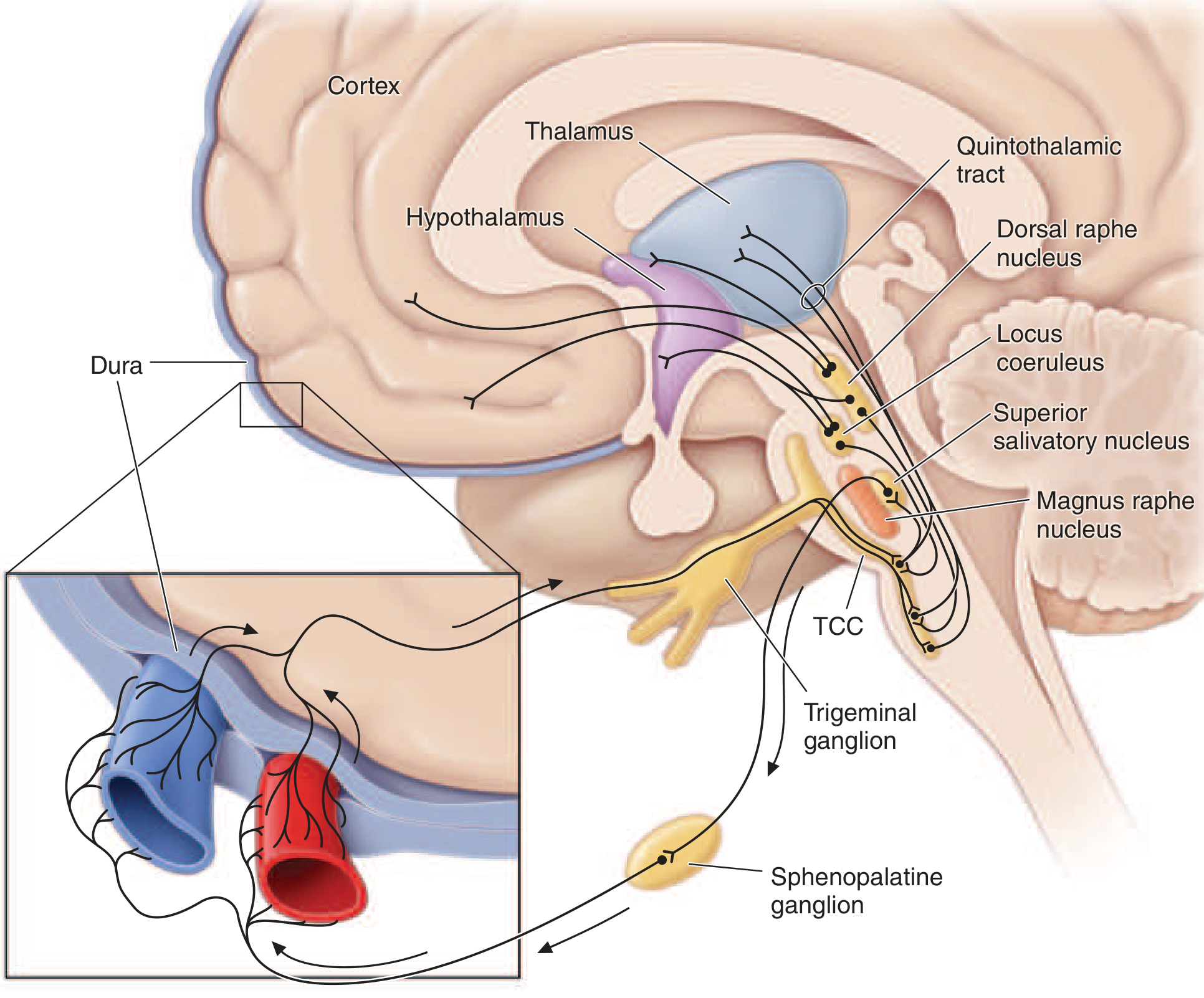
Key pathway:
- Trigeminal nerve innervates intracranial vessels and dura mater (trigeminovascular system)
- Neurogenic inflammation: trigeminal nerve endings release CGRP (Calcitonin Gene-Related Peptide), Substance P, Neurokinin A
- CGRP causes potent vasodilation + plasma protein extravasation into perivascular space
- Perivascular edema → mechanical stretching → activation of pain endings in dura
- Pain signals pass: Trigeminal ganglion → Trigeminocervical Complex (TCC) → Quintothalamic tract → Thalamus → Cortex
Modulating centers: Dorsal raphe nucleus (serotonergic), Locus coeruleus (noradrenergic), Nucleus raphe magnus
Key point: Migraine is a brain disorder - NOT a "vascular headache." Vascular changes are secondary events, not causative.
Serotonin (5-HT) Role
- Serotonin levels FALL during headache phase → vasodilation
- Platelet serotonin release during prodrome → vasoconstriction
- Migraine drugs act on 5-HT1B/1D receptors
DIAGNOSTIC CRITERIA (IHS/ICHD-3)
Migraine WITHOUT Aura (≥5 attacks):
- Duration 4-72 hours (untreated)
- At least 2 of: Unilateral, Pulsating, Moderate/severe, Aggravated by routine activity
- At least 1 of: Nausea/vomiting OR Photophobia + Phonophobia
Migraine WITH Aura (≥2 attacks):
- One or more fully reversible aura symptoms
- Each aura lasts 5-60 minutes
- Headache during or following aura within 60 minutes
MIDAS Score (Migraine Disability Assessment Score) - validated tool to assess disability and guide treatment intensity.
TRIGGERS (Mnemonic: STRESS)
- S - Sleep changes (too much/too little)
- T - Tyramine-containing foods (cheese, red wine, chocolate)
- R - Red wine/alcohol
- E - Estrogen changes (menstruation, OCP)
- S - Stress (or let-down after stress)
- S - Sensory stimuli (bright lights, loud noise, strong smells)
Other triggers: caffeine withdrawal, skipping meals, weather changes, altitude
TREATMENT
Diagram Summary
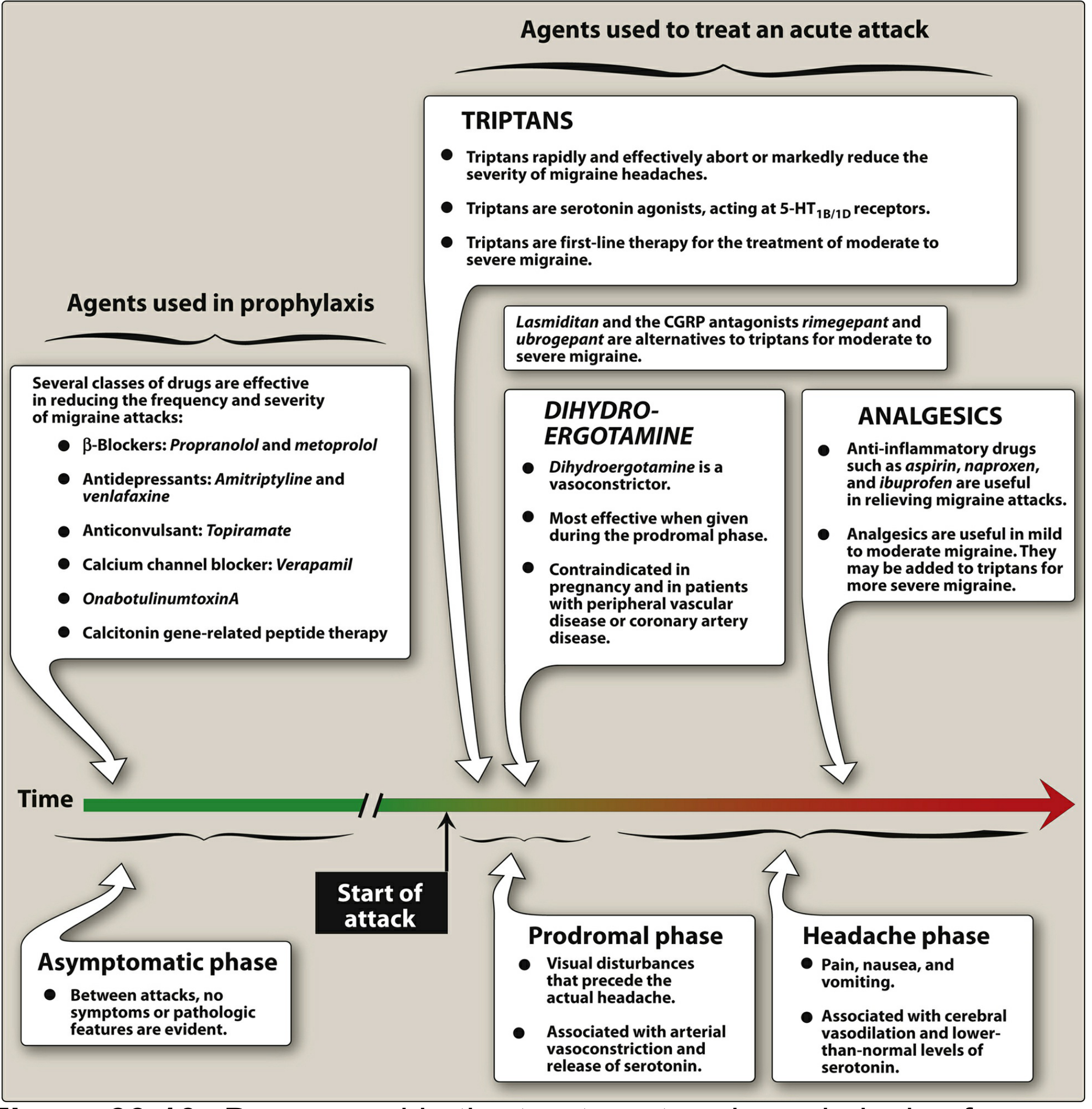
A. ACUTE (ABORTIVE) TREATMENT
Step 1 - Mild to Moderate Attacks
NSAIDs / Simple Analgesics (first choice for mild attacks)
- Aspirin 600-900 mg, Ibuprofen 400-800 mg, Naproxen 500-1000 mg
- Paracetamol + Aspirin + Caffeine combination (FDA approved)
- Aspirin + Metoclopramide (comparable to oral sumatriptan)
- Take early in attack for best effect
Step 2 - Moderate to Severe Attacks
TRIPTANS (5-HT1B/1D Agonists) - DRUGS OF CHOICE
| Drug | Route | Dose |
|---|---|---|
| Sumatriptan (prototype) | PO, SC, IN, PR | 50-100 mg PO; 6 mg SC; 20 mg IN |
| Rizatriptan | PO, MLT wafer | 10 mg |
| Zolmitriptan | PO, nasal spray | 2.5 mg PO; 5 mg IN |
| Almotriptan | PO | 12.5 mg |
| Eletriptan | PO | 40 mg |
| Naratriptan | PO | 2.5 mg (slower onset, better tolerability, less recurrence) |
| Frovatriptan | PO | 2.5 mg (longest half-life, menstrual migraine) |
Mechanism: Selective 5-HT1B/1D receptor agonists
- Activate presynaptic receptors on trigeminal nerve endings → inhibit release of CGRP, Substance P
- Cause vasoconstriction of dilated intracranial vessels
Pharmacokinetics of Sumatriptan:
- Oral bioavailability: ~15% (high first-pass)
- SC injection: fastest onset (relief in 30-60 min)
- Metabolized by MAO-A
- Do NOT combine with MAO inhibitors or ergotamine (within 24 hours)
Contraindications of Triptans:
- Coronary artery disease / ischemic heart disease (most important)
- Uncontrolled hypertension
- Cerebrovascular disease / history of stroke
- Hemiplegic/basilar migraine
- Pregnancy
- Peripheral vascular disease
Adverse Effects:
- "Triptan sensations": chest tightness, tingling, flushing, neck pressure (usually benign but alarming)
- Nausea, dizziness
- Medication overuse headache (if used >10 days/month)
Rizatriptan and Eletriptan - most efficacious on population basis
Sumatriptan SC - fastest onset; best for severe vomiting
Naratriptan/Almotriptan - best tolerated, lowest recurrence rate
ERGOT ALKALOIDS
| Drug | Route | Notes |
|---|---|---|
| Ergotamine + Caffeine | PO/PR | 1-2 mg; caffeine enhances absorption |
| Dihydroergotamine (DHE) | IM, IV, IN | 1 mg IM/IV; 2 mg nasal spray |
Mechanism: Non-selective 5-HT1 agonist + vasoconstriction (also α-adrenergic agonist)
- Most effective when given during prodromal phase
- DHE preferred over ergotamine (less nausea, less arterial spasm)
Contraindications:
- Coronary artery disease
- Hypertension
- Peripheral vascular disease
- Pregnancy (oxytocic)
- Renal/hepatic impairment
Do NOT combine with triptans (within 24 hours - risk of additive vasoconstriction)
NEWER AGENTS
Gepants (CGRP Receptor Antagonists)
| Drug | Use |
|---|---|
| Rimegepant 75 mg PO | Acute + Prevention |
| Ubrogepant 50/100 mg PO | Acute (triptan-intolerant) |
| Zavegepant 10 mg nasal spray | Acute (fast onset) |
| Atogepant | Prevention only |
- Advantage over triptans: No vasoconstriction → safe in cardiovascular disease
- Avoid with strong CYP3A4 inhibitors (ubrogepant)
- Can be re-dosed at 2 hours (unlike triptans)
Ditans (5-HT1F Agonists)
- Lasmiditan 50-200 mg PO
- Does NOT cause vasoconstriction → safe in cardiovascular disease
- Causes CNS side effects (dizziness, sedation) - do not drive for 8 hours
Antiemetics (Adjunctive)
- Metoclopramide 10 mg IV/IM - for severe nausea/vomiting; also enhances analgesic absorption
- Prochlorperazine - also has antimigraine properties
- Domperidone - enhances GI absorption of analgesics
Clinical Guide: Which drug when?
| Situation | Treatment |
|---|---|
| Mild attack | NSAIDs / Paracetamol + Caffeine |
| Moderate-severe | Triptans (oral) |
| Early nausea/vomiting | Nasal spray (sumatriptan 20 mg / zolmitriptan 5 mg) |
| Very rapid symptoms | Sumatriptan SC 6 mg |
| Contraindication to triptans (CVS) | Gepants or Lasmiditan |
| Headache recurrence | Naratriptan / Eletriptan / Rimegepant (re-dosable) |
| Menstrual migraine | Frovatriptan / Estrogen patches / Rimegepant perimenstrually |
B. PROPHYLACTIC TREATMENT
Indications for Prophylaxis:
- ≥2 attacks per month
- Attacks severely disabling despite acute treatment
- Contraindication to acute treatments
- Medication overuse headache
- Complicated migraine (hemiplegic, basilar)
First-Line Prophylactic Agents
| Drug Class | Drugs | Notes |
|---|---|---|
| β-Blockers (DOC) | Propranolol 40-240 mg/day, Metoprolol | Avoid in asthma, diabetes |
| Anticonvulsants | Topiramate 50-200 mg/day, Valproic acid (divalproex) | Valproate - avoid in pregnancy |
| Tricyclics | Amitriptyline 10-75 mg at night | Also for comorbid depression/TTH |
| Calcium Channel Blockers | Flunarizine (preferred), Verapamil | Flunarizine used in India |
Second-Line Prophylactic Agents
| Drug | Notes |
|---|---|
| Anti-CGRP monoclonal antibodies | Erenumab, Galcanezumab, Fremanezumab, Eptinezumab (injectable, monthly/quarterly) |
| OnabotulinumtoxinA | 155-195 units injected every 12 weeks (chronic migraine ≥15 days/month) |
| SSNRIs | Venlafaxine |
| Oral CGRP antagonists | Rimegepant, Atogepant |
KD Tripathi Key Points for Exam:
- DOC for prophylaxis = Propranolol
- DOC for acute severe migraine = Sumatriptan
- Ergotamine is no longer first-line (replaced by triptans)
- Flunarizine - preferred calcium channel blocker for migraine prophylaxis in India
NON-PHARMACOLOGICAL MANAGEMENT
- Identify and avoid personal triggers (keep headache diary)
- Regular sleep schedule, meals, exercise
- Stress management: yoga, meditation, biofeedback, relaxation therapy
- Avoid excess caffeine/alcohol
- Non-invasive vagus nerve stimulation, transcranial magnetic stimulation (newer options)
SPECIAL SITUATIONS
Migraine in Pregnancy
- Avoid: Ergotamine (oxytocic), triptans (limited data), valproate (teratogenic), NSAIDs in 3rd trimester
- Safe options: Paracetamol, Metoclopramide, Magnesium
- Prophylaxis: Propranolol (if needed), Amitriptyline
Menstrual Migraine
- Occurs 1-2 days before to 3 days after onset of menstruation
- Due to estrogen withdrawal
- Perimenstrual prophylaxis: Frovatriptan, Estrogen patches, Naproxen, Rimegepant
Status Migrainosus (attack >72 hours)
- IV hydration, IV Metoclopramide, IV Valproate, IV Dihydroergotamine
- Short course of corticosteroids (Dexamethasone)
Medication Overuse Headache (MOH)
- Occurs with >10 days/month use of triptans or >15 days/month of analgesics
- Treatment: Withdraw offending drug; bridge with NSAIDs or corticosteroids; start prophylaxis
QUICK REVISION TABLE - Drugs Acting on 5-HT in Migraine
| Drug | Receptor | Action |
|---|---|---|
| Triptans | 5-HT1B/1D agonist | Vasoconstriction + ↓CGRP/Substance P release |
| Ergotamine/DHE | 5-HT1 agonist (non-selective) + α-adrenergic | Vasoconstriction |
| Lasmiditan | 5-HT1F agonist | ↓Trigeminal activation, NO vasoconstriction |
| Methysergide* | 5-HT2 antagonist | Prophylaxis (historical, rarely used now) |
| Pizotifen* | 5-HT2 antagonist + antihistamine | Prophylaxis |
*Largely historical/rarely used now
HIGH-YIELD EXAM POINTS (KD Tripathi Style)
- Triptans MOA: 5-HT1B/1D agonists → vasoconstriction + inhibit CGRP/SP release
- Sumatriptan CI: Coronary artery disease (vasoconstriction risk)
- Ergotamine + Triptan should NOT be combined (additive vasoconstriction - gap of 24 h)
- Sumatriptan + MAO inhibitor - contraindicated (reduced metabolism → toxicity)
- CGRP is the key neuropeptide in migraine pathophysiology
- Frovatriptan - longest half-life (26 h), preferred for menstrual migraine
- Naratriptan - best tolerated triptan, least headache recurrence
- Propranolol = DOC for migraine prophylaxis
- Topiramate = anticonvulsant used in migraine prophylaxis (also causes weight loss)
- Valproate - avoid in pregnancy (teratogen - neural tube defects)
- Gepants - safe in CVS disease (no vasoconstriction); can be re-dosed at 2 h
- Botulinum toxin - prophylaxis for chronic migraine (≥15 days/month)
- Cortical spreading depression (CSD) - mechanism of aura
- Medication overuse headache - warn patients using triptans/NSAIDs too frequently
- Migraine is a BRAIN disorder - NOT a vascular headache
Sources: Harrison's Principles of Internal Medicine 22E, Katzung Basic & Clinical Pharmacology 16E, Lippincott Illustrated Reviews Pharmacology - aligned with KD Tripathi Essentials of Medical Pharmacology content on 5-HT agonists and migraine management
This is a shared conversation. Sign in to Orris to start your own chat.