Here is the fully combined, exam-ready answer integrating Gray's Anatomy for Students, Bailey & Love's Surgery, Fishman's Pulmonary Diseases, and Murray & Nadel's Respiratory Medicine:
MEDIASTINAL ANATOMY AND APPLIED ANATOMY
Complete 10-Mark Answer for MD Examinations
1. DEFINITION AND BOUNDARIES
The mediastinum is a thick midline partition - the potential space between the two pleural cavities - extending from the sternum anteriorly to the thoracic vertebrae posteriorly, and from the superior thoracic aperture (thoracic inlet) above to the diaphragm below. Laterally, it is bounded on each side by the mediastinal parietal pleura.
It contains all thoracic viscera except the lungs, and communicates freely with the neck (via deep cervical fascial planes) and the retroperitoneum - allowing infection, air, or hemorrhage to disseminate widely.
2. SUBDIVISIONS OF THE MEDIASTINUM
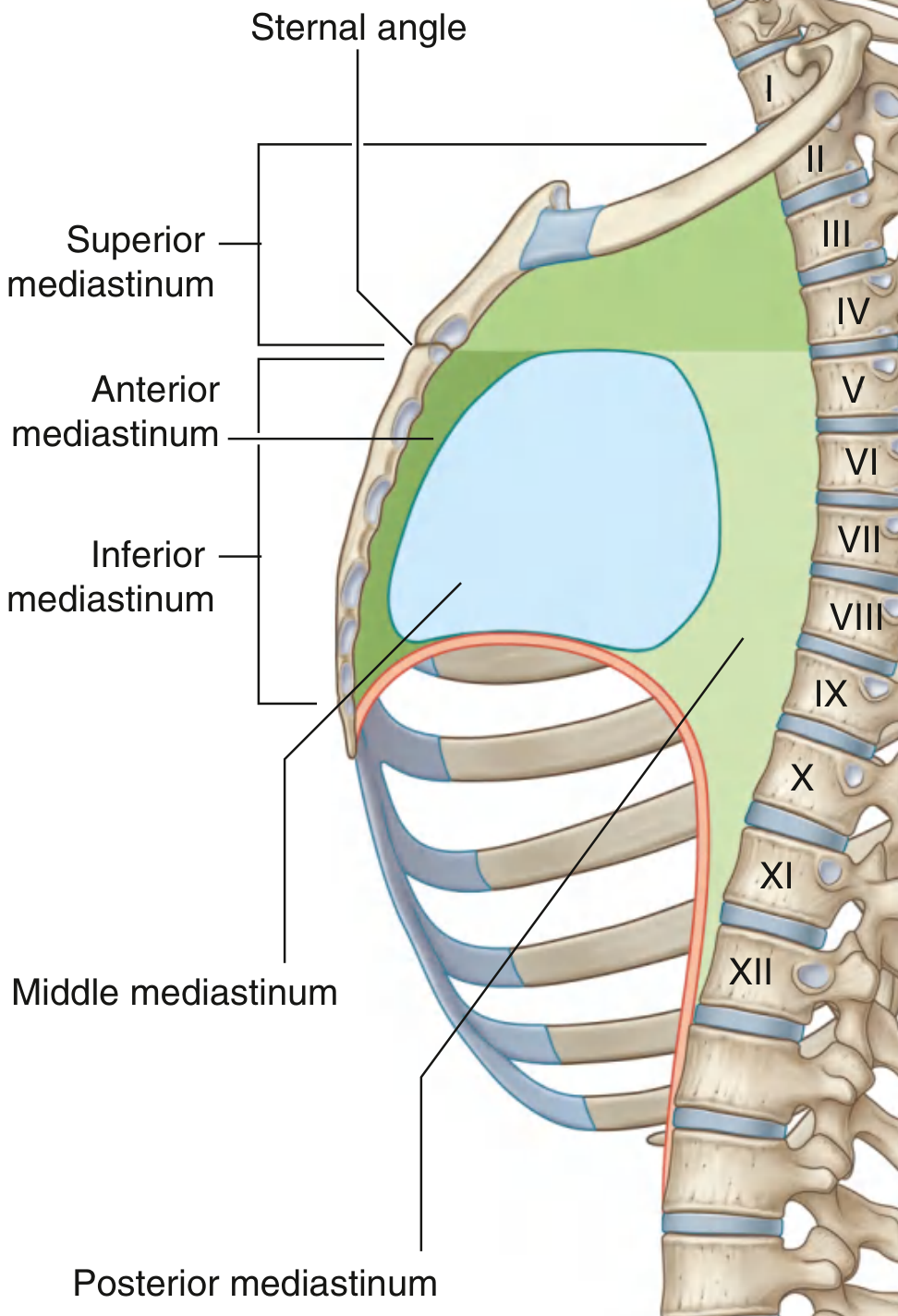
A horizontal plane through the sternal angle of Louis (anteriorly) and the intervertebral disc between T4 and T5 (posteriorly) divides the mediastinum into:
- Superior mediastinum (above the plane)
- Inferior mediastinum (below the plane), further divided by the pericardium into:
- Anterior - between sternum and pericardium
- Middle - the pericardium and heart
- Posterior - between pericardium and vertebral column
Fig. Subdivisions of the Mediastinum (Gray's Anatomy for Students)
A surgically practical alternative - the Shields three-compartment model - divides the mediastinum into anterior (prevascular), middle (visceral), and posterior (paravertebral) compartments, all extending from the thoracic inlet to the diaphragm. The ITMIG CT-based classification has refined this further using axial imaging.
3. SUPERIOR MEDIASTINUM
Boundaries
| Wall | Structure |
|---|
| Anterior | Manubrium sterni |
| Posterior | Bodies of T1-T4 vertebrae |
| Superior | Oblique plane from jugular notch to upper border of T1 |
| Inferior | Sternal angle / T4-T5 disc plane |
| Lateral | Mediastinal pleura on each side |
Contents
Mnemonic: "TV Ate Ten Pints As A Tipple"
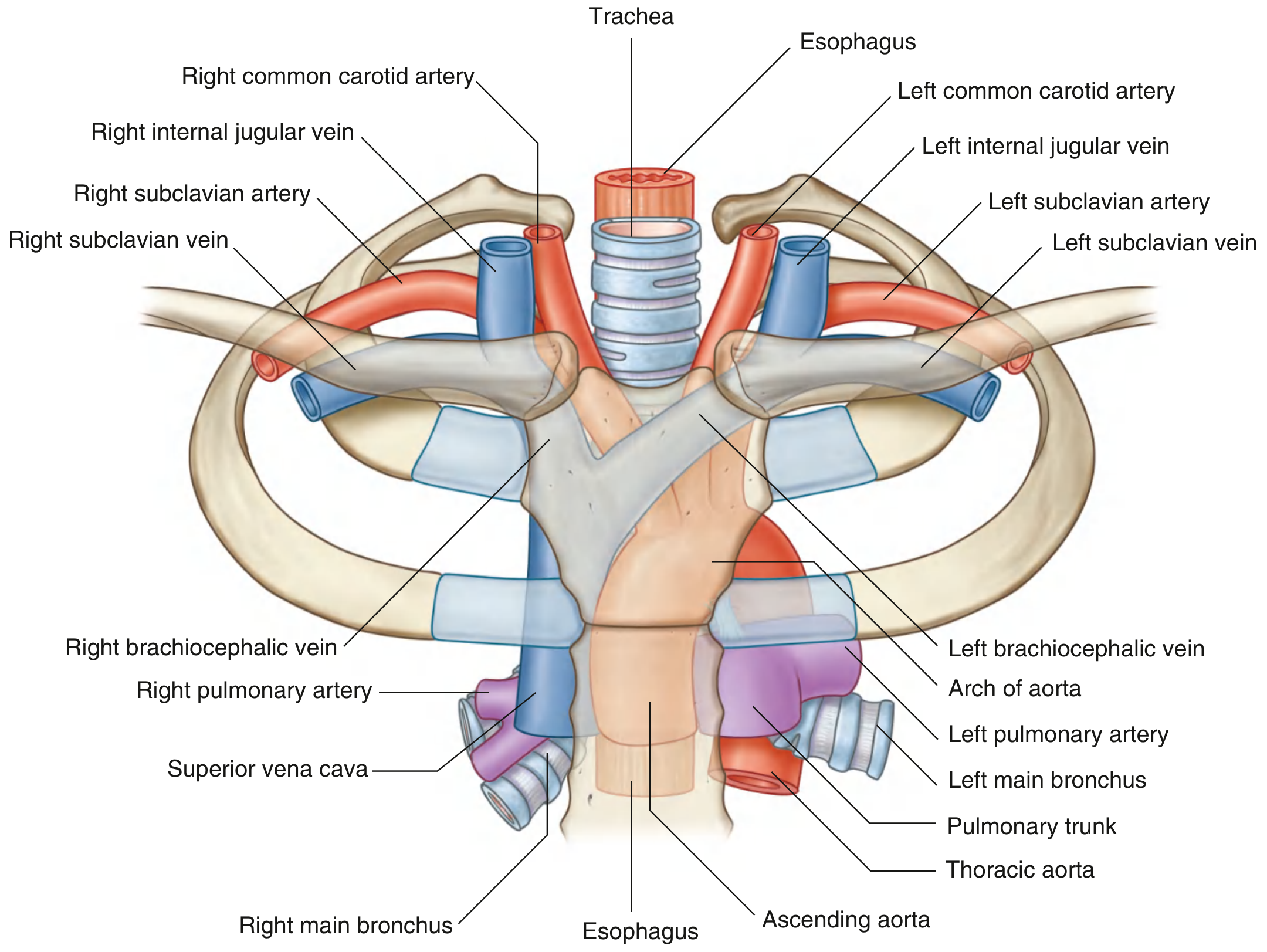
- Thymus - most anterior structure, immediately posterior to manubrium; large in childhood, atrophies after puberty
- Veins - right and left brachiocephalic veins (unite to form SVC); upper half of SVC; left superior intercostal vein
- Arch of Aorta - begins at right 2nd sternocostal joint; arches upward, backward, and to the left; ends at T4/T5 on the left; gives three branches (right to left): brachiocephalic trunk, left common carotid artery, left subclavian artery. All three are crossed anteriorly by the left brachiocephalic vein
- Trachea - bifurcates at T4/T5 = carina
- Esophagus - lies posterior to trachea
- Phrenic nerves (C3, C4, C5)
- Vagus nerves (both sides)
- Left recurrent laryngeal nerve - branches from left vagus at aortic arch, hooks under ligamentum arteriosum, ascends in tracheo-esophageal groove
- Thoracic duct (upper portion)
- Lymph nodes, fat, smaller vessels
Fig. Superior Mediastinum Structures (Gray's Anatomy for Students)
4. ANTERIOR MEDIASTINUM
Boundaries
| Wall | Structure |
|---|
| Anterior | Body of sternum |
| Posterior | Pericardial sac |
| Superior | T4/T5 plane (sternal angle) |
| Inferior | Diaphragm |
| Lateral | Mediastinal pleura |
Contents
- Inferior extension of the thymus - the major structure
- Fat, areolar tissue, lymph nodes
- Mediastinal branches of internal thoracic vessels
- Sternopericardial ligaments - connect posterior sternum to fibrous pericardium, maintaining cardiac position
This is the smallest subdivision and most surgically accessible (median sternotomy). It is the site of the classic "4 T's" anterior mediastinal masses.
5. MIDDLE MEDIASTINUM
Contents
- Pericardium (fibrous and serous) and pericardial cavity
- Heart
- Roots/origins of great vessels: ascending aorta, pulmonary trunk, upper SVC, pulmonary veins
- Phrenic nerves and pericardiacophrenic vessels (travel within/on fibrous pericardium, C3-C5)
- Proximal main bronchi
- Lymph nodes
Pericardium
A fibroserous sac with two components:
1. Fibrous pericardium - tough outer cone-shaped layer; base fused to central tendon of diaphragm; apex continuous with great vessel adventitia; anteriorly attached to sternum via sternopericardial ligaments. Limits cardiac distension.
2. Serous pericardium (two layers):
- Parietal layer - lines inner surface of fibrous pericardium
- Visceral layer (epicardium) - adheres to myocardium
Between the two serous layers: the pericardial cavity (15-50 mL fluid normally), allowing uninhibited cardiac movement.
Sinuses of the Pericardium
- Transverse sinus - posterior to ascending aorta and pulmonary trunk, anterior to SVC. Surgically critical: a finger or clamp passed through this sinus controls both great arterial outflow tracts simultaneously during cardiac surgery.
- Oblique sinus - a cul-de-sac posterior to the left atrium, bounded by pulmonary veins and IVC. Fluid tends to pool here, detectable on echocardiography.
6. POSTERIOR MEDIASTINUM
Boundaries
| Wall | Structure |
|---|
| Anterior | Posterior pericardium and diaphragm |
| Posterior | Bodies of T5-T12 vertebrae |
| Superior | T4/T5 plane |
| Inferior | Diaphragm |
| Lateral | Mediastinal pleura |
Contents
- Esophagus and esophageal nerve plexus
- Thoracic (descending) aorta and branches
- Azygos system of veins
- Thoracic duct and lymph nodes
- Sympathetic trunks
- Thoracic splanchnic nerves
A. Esophagus
Descends anterior to vertebral bodies (midline), deviates left and anterior as it nears the diaphragm, crossing to the left of the thoracic aorta. Passes through the esophageal hiatus at T10.
Four normal constrictions (high-yield for foreign body impaction, carcinoma sites, and barium swallow interpretation):
| Level | Cause | Vertebral Level |
|---|
| 1st | Pharyngo-esophageal junction (cricopharyngeus) | C6 |
| 2nd | Aortic arch crosses the esophagus | T4 |
| 3rd | Left main bronchus crosses | T5/T6 |
| 4th | Esophageal hiatus in diaphragm | T10 |
B. Thoracic (Descending) Aorta
Begins at lower edge of T4 (continuous with arch), ends at T12 (passes through the aortic hiatus posterior to the diaphragm). Initially left of midline, approaches midline inferiorly.
Branches:
| Branch | Details |
|---|
| Posterior intercostal arteries (9 pairs) | Supply lower 9 intercostal spaces (upper 2 supplied by supreme intercostal from costocervical trunk) |
| Bronchial arteries | Usually 2 left from aorta; 1 right from 3rd posterior intercostal |
| Esophageal branches (4-5) | Form continuous anastomotic chain |
| Superior phrenic arteries | Posterior diaphragm |
| Subcostal artery | Below rib XII |
| Pericardial, mediastinal branches | Small vessels |
C. Azygos System of Veins
Provides collateral drainage between SVC and IVC. Drains thoracic wall and posterior mediastinal structures.
- Azygos vein (right): arises from right ascending lumbar + right subcostal veins; ascends to T4 where it arches over the root of the right lung to drain into the SVC; drains lower 8-9 right intercostal spaces
- Hemiazygos vein (inferior left): ascends to ~T9, crosses midline posterior to aorta and thoracic duct to join azygos; drains lowest 4-5 left intercostal spaces
- Accessory hemiazygos vein (superior left): descends from T4 to T8; crosses to join azygos or hemiazygos; drains 4th-8th left intercostal spaces
D. Thoracic Duct
The largest lymphatic channel in the body. Drains all lymph from below the diaphragm and left side above it.
- Begins as cisterna chyli at L2 (confluence of intestinal + bilateral lumbar trunks)
- Enters thorax through aortic hiatus (T12), posterior to the aorta
- Ascends in posterior mediastinum - right of midline, between thoracic aorta (left) and azygos vein (right)
- At T4-T5 crosses to the left
- Terminates at the left venous angle (junction of left internal jugular and left subclavian veins)
- The right lymphatic duct drains the right head/neck/thorax/upper limb into the right venous angle
E. Sympathetic Trunks and Splanchnic Nerves
Thoracic sympathetic trunks lie on either side of the vertebral column, anterior to costovertebral joints.
Thoracic splanchnic nerves (preganglionic sympathetic fibers to abdomen):
- Greater splanchnic nerve (T5-T9) - celiac plexus
- Lesser splanchnic nerve (T10-T11) - aorticorenal ganglion
- Least splanchnic nerve (T12) - renal plexus
7. MEDIASTINAL LYMPH NODES (Naruke Map)
- Stations 1-9 = true mediastinal nodes (N2 disease in lung cancer)
- Stations 10 and above = hilar/intrapulmonary nodes (N1 disease, within pleural sac)
Key groups:
| Station | Name | Compartment |
|---|
| 1 | Highest mediastinal | Superior |
| 2R/2L | Upper paratracheal | Superior |
| 4R/4L | Lower paratracheal | Superior |
| 5 | Subaortic (AP window) | Anterior/Superior |
| 6 | Para-aortic | Anterior/Superior |
| 7 | Subcarinal | Middle |
| 8 | Paraesophageal | Posterior |
| 9 | Inferior pulmonary ligament | Posterior |
8. APPLIED ANATOMY - CLINICAL CORRELATIONS
1. Superior Vena Cava (SVC) Syndrome
The SVC is thin-walled with low intravascular pressure, making it vulnerable to extrinsic compression by any middle mediastinal mass.
Features: Facial/neck/upper limb edema and plethora, dilated collateral veins on thorax and neck, headache, disturbed consciousness.
Common causes: Bronchogenic carcinoma (right upper lobe), lymphoma, fibrosing mediastinitis. The azygos system acts as the principal collateral channel.
2. Left Recurrent Laryngeal Nerve Palsy
The long course of the left RLN through the superior mediastinum makes it vulnerable to:
- Bronchogenic carcinoma (left hilar/mediastinal nodes)
- Aortic aneurysm
- Enlarged mediastinal lymph nodes (lymphoma, sarcoidosis)
- Surgical injury during esophagectomy or thyroidectomy
Ortner's syndrome = cardiovascular cause (aortic aneurysm, enlarged left atrium) of RLN palsy causing hoarseness. The right RLN loops around the right subclavian artery in the neck - less prone to mediastinal pathology.
3. Cardiac Tamponade
Acute accumulation of fluid in the pericardial cavity (pathological when >100 mL acutely) prevents cardiac filling. The inelastic fibrous pericardium cannot stretch acutely.
Beck's Triad: (1) Hypotension, (2) Raised JVP, (3) Muffled heart sounds.
Also: pulsus paradoxus (>10 mmHg fall in systolic BP on inspiration), Kussmaul sign.
Pericardiocentesis - Anatomical Basis:
Preferred route: subxiphoid (epigastric) - needle inserted between xiphoid process and left costal margin, angled at 45 degrees toward the left shoulder. This approach avoids:
- Internal thoracic vessels (risk with lateral approach)
- Phrenic nerve and pericardiacophrenic vessels
- Coronary vessels
4. Mediastinoscopy
Surgical endoscopy of the superior mediastinum via a small suprasternal incision, passing the scope in the pretracheal plane. Used for biopsy of mediastinal lymph nodes (lung cancer staging, lymphoma, sarcoidosis).
Structures at risk: left RLN, phrenic nerve, SVC, azygos vein, aortic arch branches, innominate artery (right side).
5. Mediastinal Masses - Compartment-Based Diagnosis
The compartment of origin strongly predicts the nature of the mass - a core exam principle:
| Compartment | Masses ("4 T's" for Anterior) |
|---|
| Anterior | Thymoma (most common overall 26.5%), Teratoma/germ cell tumor, Thyroid (substernal goiter), Terrible lymphoma |
| Middle | Lymphoma, bronchogenic cyst, pericardial cyst, aortic aneurysm, tracheal tumors, sarcoidosis |
| Posterior | Neurogenic tumors (most common in children 41%), esophageal lesions, thoracic aortic aneurysm, meningocele |
"About 80% of asymptomatic masses are benign, whereas more than half of those that produce symptoms are malignant." - Murray & Nadel
6. Pneumomediastinum (Macklin Effect)
Mechanism (Macklin, 1944): Alveolar rupture → air enters perivascular interstitium → dissects proximally within bronchovascular sheaths → reaches mediastinum. From there: pneumopericardium, cervical/subcutaneous emphysema, or retroperitoneal air.
Hamman sign: Crunching/clicking sound over precordium synchronous with heartbeat - pathognomonic of pneumomediastinum.
Common causes: mechanical ventilation (barotrauma), severe Valsalva, asthma, esophageal perforation.
7. Boerhaave Syndrome (Esophageal Rupture)
Spontaneous esophageal perforation from sudden rise in intraluminal pressure (typically vomiting). Tears occur in the lower left esophagus, causing:
- Left-sided pleural effusion with gastric contents
- Mediastinitis (rapidly progressive, high mortality)
- Subcutaneous emphysema
Surgical emergency - requires urgent exploration and repair.
8. Chylothorax (Thoracic Duct Injury)
Milky pleural fluid rich in chylomicrons (triglyceride level >110 mg/dL). The thoracic duct is at risk during:
- Esophagectomy
- Left thoracotomy
- Left subclavian vein catheterization (thoracic duct terminates at left venous angle)
Management: conservative (low-fat/MCT diet, octreotide) or surgical/thoracoscopic ligation.
9. Horner Syndrome
Posterior mediastinal mass or paravertebral sulcus mass compressing the cervicothoracic sympathetic chain (stellate ganglion, T1).
Features: Ptosis, miosis, anhidrosis, enophthalmos (all ipsilateral). Look for this in Pancoast tumor (superior sulcus tumor - also causes C8/T1 brachial plexus involvement).
10. Central Venous Access - Anatomical Basis
Lines inserted via internal jugular or subclavian veins pass through the brachiocephalic veins into the SVC. The optimal tip position is the SVC-right atrial junction.
The left subclavian/jugular approach carries a higher risk of injury to the thoracic duct (which terminates at the left venous angle). The superior and inferior venae cavae share a common vertical axis, allowing passage of guidewires through the right heart into the IVC for: transjugular liver biopsy, TIPS insertion, IVC filter placement.
9. CT-BASED CLASSIFICATION (ITMIG - Modern)
The International Thymic Malignancy Interest Group revised the classification using axial CT:
| CT Compartment | Traditional Equivalent | Posterior Boundary |
|---|
| Prevascular | Anterior | Anterior pericardium |
| Visceral | Middle | 1 cm posterior to anterior vertebral margin |
| Paravertebral | Posterior | Lateral margin of transverse processes |
10. SUMMARY TABLE FOR QUICK REVISION
| Feature | Key Point |
|---|
| Boundaries | Sternum (ant), vertebrae (post), thoracic inlet (sup), diaphragm (inf) |
| Dividing plane | Sternal angle / T4-T5 disc |
| Only true anatomic compartment | Pericardial sac |
| Communicates with | Neck and retroperitoneum via fascial planes |
| Most common adult mediastinal mass | Thymoma (anterior) |
| Most common pediatric mass | Neurogenic tumor (posterior) |
| 4 T's of anterior mediastinum | Thymoma, Teratoma, Thyroid, Terrible lymphoma |
| SVC syndrome | Middle mass compresses thin-walled, low-pressure SVC |
| Hamman sign | Crunching precordial sound = pneumomediastinum |
| Horner syndrome | Posterior mass compressing sympathetic chain |
| Macklin effect | Alveolar rupture → bronchovascular sheath → mediastinum |
| Transverse sinus | Surgical access to control aorta + pulmonary trunk |
| Pericardiocentesis route | Subxiphoid, toward left shoulder |
| Thoracic duct termination | Left venous angle (left IJ + subclavian junction) |
| Naruke stations 1-9 | True mediastinal nodes (N2 in lung cancer) |
| Recurrent laryngeal palsy | Left RLN vulnerable in superior mediastinum (aortic arch loop) |
| Boerhaave syndrome | Lower left esophageal rupture → left effusion + mediastinitis |
| Chylothorax | Thoracic duct injury → milky effusion, TG >110 mg/dL |
| Beck's triad | Hypotension + raised JVP + muffled heart sounds = tamponade |
Sources: Gray's Anatomy for Students 4th Ed. | Bailey & Love's Short Practice of Surgery 28th Ed. | Fishman's Pulmonary Diseases & Disorders | Murray & Nadel's Textbook of Respiratory Medicine