Mri spine basics
MRI spine basics sequences anatomy radiology
https://pmc.ncbi.nlm.nih.gov/articles/PMC7571515
MRI Spine - Basics
Why MRI?
Standard Protocol (Routine Sequences)
| Sequence | Plane | Purpose |
|---|---|---|
| T1-weighted | Sagittal | Anatomy, bone marrow, fat |
| T2-weighted | Sagittal | Discs, CSF, cord, pathology |
| STIR or T2 fat-sat | Sagittal | Edema, marrow changes, ligament injury |
| T2-weighted | Axial | Canal, foramina, disc herniations |
| T1-weighted | Axial | Added in lumbar spine; foraminal fat around nerve roots |
Core Sequences Explained
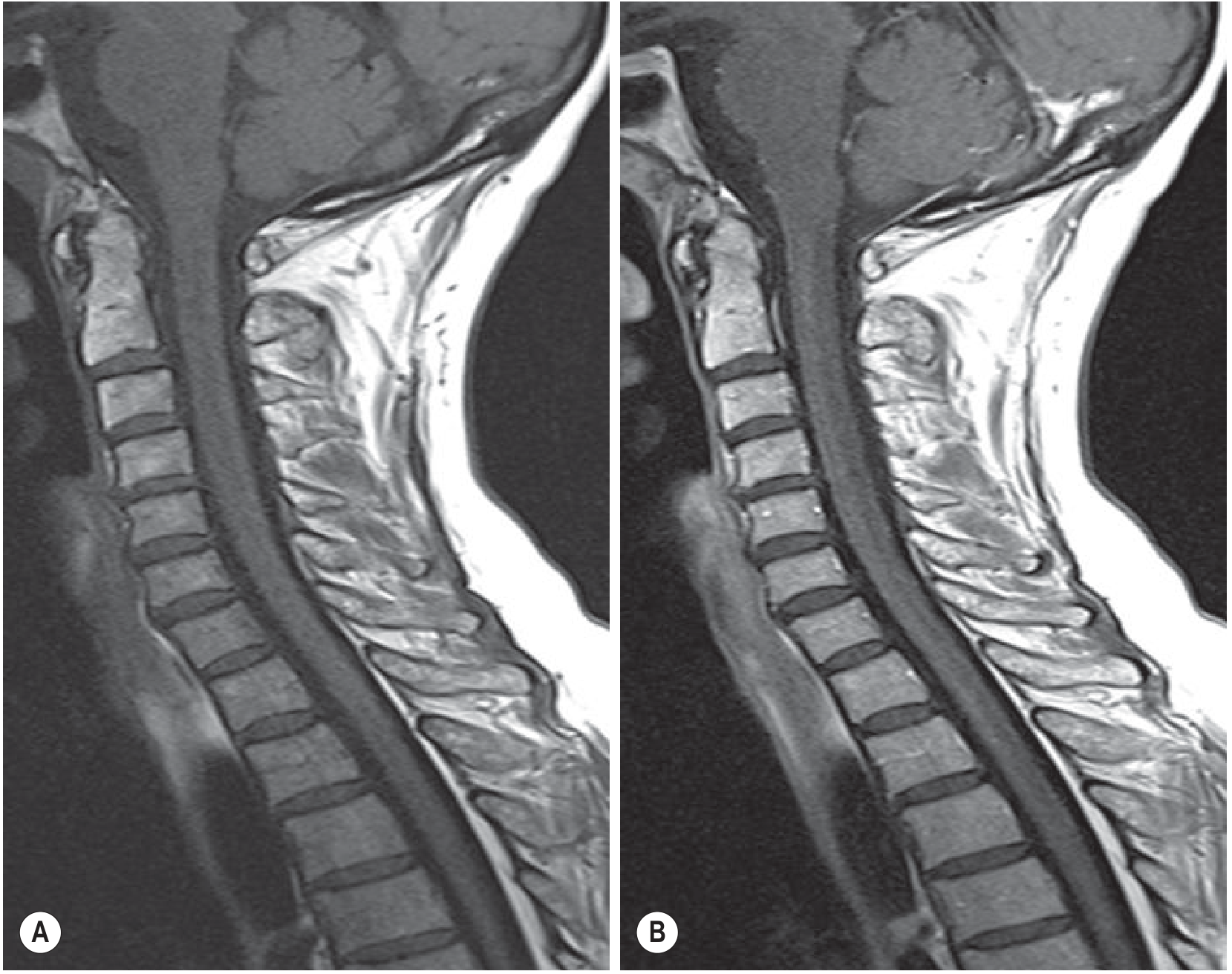
T1-Weighted Imaging
- Short TR (300-700 ms) and short TE (<30 ms)
- Fat = bright (high signal) - bone marrow appears bright
- CSF = dark (low signal)
- Excellent for: bone marrow changes, anatomical detail, osseous structures, discs, soft tissue
- Before/after gadolinium: detects neoplastic and infectious processes
T2-Weighted Imaging
- Long TR (2000-3000 ms) and long TE (80-120 ms)
- CSF = bright ("myelographic effect") - acts as natural contrast for the cord
- Healthy nucleus pulposus = bright (high water content)
- Degenerated disc = dark (loss of water/proteoglycans)
- Used as Fast Spin Echo (FSE) in practice to reduce acquisition time
- Best for: disc assessment, cord compression, edema, tumor, infection
STIR (Short Tau Inversion Recovery)
- Fat-suppression sequence using an inversion pulse
- Fat signal is nulled; pathological fluid and edema become very bright
- Excellent for: bone marrow edema, occult fractures (acute vs. chronic), ligament injury, Modic changes, vertebral metastases, multiple sclerosis lesions
- More robust fat suppression than frequency-selective saturation in large fields of view
- Preferred over T2 fat-sat in trauma because it is more reliable
Gradient Echo (GRE / T2*)
- Shorter acquisition times, less CSF pulsation artifact
- Best demonstrates hemorrhage and blood products - important prognostic indicator in neurological injury
- More susceptible to metallic susceptibility artifacts (avoid in post-surgical spines with implants)
- Useful in cervical and thoracic spine
Contrast-Enhanced T1 (Gadolinium)
- Gd chelates shorten T1 - enhancement = bright on T1
- Blood-brain/spinal barrier breakdown = intra-axial enhancement
- Hypervascularity = extra-axial enhancement
- Key uses:
- Distinguish post-op scar (enhances immediately and uniformly) from recurrent disc (peripheral enhancement)
- Neoplastic and infectious workup
- Fat suppression after Gd improves conspicuity of epidural enhancement
DWI (Diffusion-Weighted Imaging)
- High signal on DWI + low ADC = restricted diffusion (cell death)
- Uses in spine: abscess, cord infarction, metastatic disease
- Increasingly added to routine spine protocols
Signal Characteristics - Quick Reference
| Structure / Finding | T1 | T2 | STIR |
|---|---|---|---|
| Normal bone marrow (fat) | Bright | Bright | Dark (suppressed) |
| CSF | Dark | Bright | Bright |
| Healthy nucleus pulposus | Intermediate | Bright | Bright |
| Degenerated disc | Intermediate | Dark | Variable |
| Acute bone marrow edema | Dark | Bright | Bright |
| Fat (epidural) | Bright | Bright | Dark |
| Cord (normal) | Intermediate | Intermediate | Intermediate |
| Acute cord injury/edema | Iso/hypointense | Hyperintense | Hyperintense |
| Hemorrhage (subacute) | Bright | Variable | Variable |
Modic Changes (Vertebral Endplate)
| Type | T1 | T2 | Gadolinium | Pathology |
|---|---|---|---|---|
| Type I | Low | High | Present | Marrow edema/inflammation |
| Type II | High | High | Absent | Fatty marrow conversion |
| Type III | Low | Low | Absent | Subchondral sclerosis |
Intervertebral Disc on MRI
- Young adult normal disc: low-intermediate T1, high T2 (bright nucleus pulposus indistinguishable from inner annulus)
- Outer annulus fibrosus: low signal on both T1 and T2 (high collagen)
- Degeneration: T2 signal decreases with loss of water/proteoglycans; disc height loss; annular tears
- Third decade change: intranuclear cleft appears as a dark horizontal band on T2 - normal aging
- Disc herniation is best assessed on both sagittal and axial images; foraminal herniation confirmed on sagittal T1 (loss of bright epidural fat around nerve root)
Artifacts to Know
| Artifact | Cause | Notes |
|---|---|---|
| Susceptibility artifact | Metal implants | Worsened with GRE; use SE/FSE instead; use metal artifact reduction sequences (MARS) |
| Motion artifact | Patient movement; swallowing (cervical); cardiac (thoracic) | Reduced by spatial presaturation |
| Truncation artifact | Fourier transformation imperfection | Dark/bright lines at cord-CSF interface; can overestimate stenosis; worse at 3T; reduce by increasing matrix size |
| CSF pulsation artifact | Pulsatile CSF in systole | Linear artifacts simulating intramedullary lesions, especially thoracic |
Regional Notes
Clinical Indications by Sequence
| Clinical Question | Best Sequence |
|---|---|
| Disc herniation / nerve compression | T2 sag + axial |
| Cord compression | T2 sagittal |
| Bone marrow edema / acute fracture | STIR |
| Infection / tumor | T1 + T2 + Gd |
| Post-op scar vs. disc | T1 + Gd with fat sat |
| Ligament injury (trauma) | T2 fat-sat / STIR |
| Hemorrhage in cord | GRE T2* |
| Epidural abscess | T1 Gd + STIR |
- Grainger & Allison's Diagnostic Radiology, Chapter 47 (Spine Imaging)
- Campbell's Operative Orthopaedics 15th Ed 2026 (MRI sections)
- Schwartz's Principles of Surgery 11th Ed (Diagnostic Studies, Ch. 42)
- PMC review - MRI of the spine
How to interpret a specific MRI spine finding (disc herniation, stenosis, disc bulge , tranvserse nerve roots, exiting nerve roots, indenting abutting, nerve root compression,tear
MRI spine disc herniation bulge exiting traversing nerve root interpretation radiology
https://pmc.ncbi.nlm.nih.gov/articles/PMC7571515
https://www.racgp.org.au/afp/2012/november/making-sense-of-m…
MRI spine stenosis grading central canal lateral recess foraminal nerve root contact displacement compression terminology
MRI Spine: Interpreting Specific Findings
PART 1 — DISC PATHOLOGY SPECTRUM
1.1 Normal Disc
- Sagittal T2: Bright (high signal) nucleus pulposus surrounded by dark outer annulus
- T1: Low-intermediate signal disc against bright bone marrow
- Disc margins should not extend beyond the vertebral apophyses (ring edges)
- In the 3rd decade, an intranuclear cleft (dark horizontal band on T2) is normal ageing
1.2 Disc Bulge
| Feature | Detail |
|---|---|
| Circumference involved | >50% (>180°) |
| Annulus | Intact but stretched |
| Shape | Smooth, symmetric or asymmetric |
| MRI appearance | Disc extends beyond apophyses uniformly |
- Symmetric bulge: Equal extension in all directions (seen normally at L5-S1 or with ligamentous laxity)
- Asymmetric bulge: More on one side (e.g., in scoliosis)
- May cause mild lateral recess narrowing
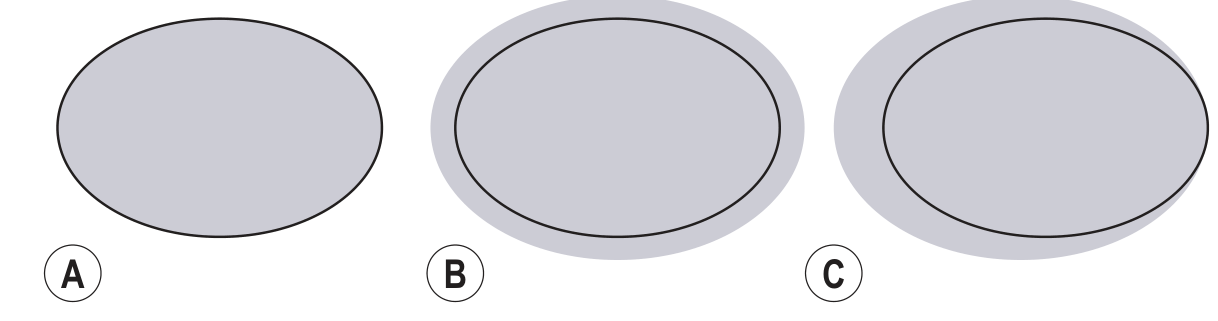
Key rule: Bulge = >50% circumference. Herniation = <50% (focal). This distinction is critical and often confused.
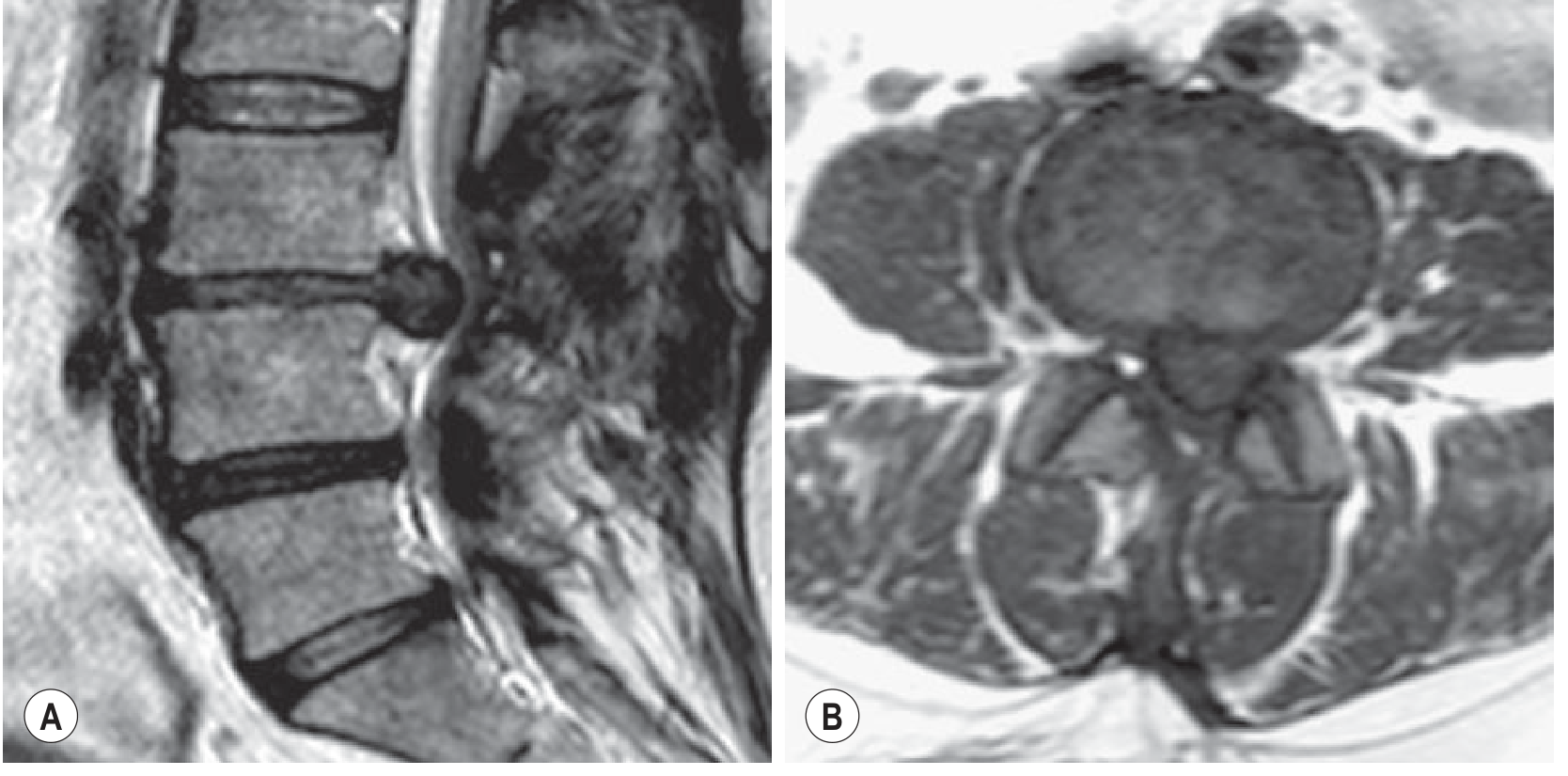
1.3 Disc Herniation
A. Protrusion
- Base (neck where it contacts the disc) is wider than the apex in ALL planes
- Think of a blister that hasn't fully popped
- Most common and mildest form
- Focal protrusion: <25% of circumference
- Broad-based protrusion: 25-50% of circumference
B. Extrusion
- Base is narrower than the herniated material in at least one plane - the "toothpaste sign"
- Material has squeezed through a narrow neck
- Can migrate cranially or caudally within the spinal canal (migrated extrusion)
- Important: Any herniation that extends above or below the disc level is an extrusion by definition
- Rarely asymptomatic - extrusion in an asymptomatic patient is uncommon
C. Sequestration / Free Fragment
- Disc material is completely disconnected from the parent disc
- Also called a "free fragment"
- High T2 signal and peripheral gadolinium enhancement → predicts spontaneous regression
- On imaging, often difficult to confirm discontinuity → the term "migration" is more practical (disc material displaced away from extrusion site regardless of continuity)
Contained vs. Uncontained
- Contained: Annulus fibrosus still covers the herniated material
- Uncontained: No annular cover; disc material is in direct contact with epidural space
- Usually impossible to distinguish on MRI (requires discography)
1.4 Summary Comparison Table
| Feature | Bulge | Protrusion | Extrusion | Sequestration |
|---|---|---|---|---|
| Circumference | >50% | <50% (focal or broad-based) | <50% | <50% |
| Base vs. apex | N/A | Base > apex | Base < apex | No base (free) |
| Annulus | Intact | Intact or torn | Torn | Disrupted |
| Migration | No | No | Possible | Yes (free fragment) |
| Likely symptomatic | Sometimes | Often | Usually | Usually |
| Spontaneous regression | Rare | Possible | Common (if free) | Common |
PART 2 — DISC LOCATION ZONES (Axial Classification)
← Posterior ←
Central (midline)
Paracentral (right/left of centre)
Subarticular / Lateral recess (right/left)
Foraminal (neural foramen, right/left)
Extraforaminal / Far lateral (outside foramen, right/left)
Anterior zone
- Pedicle level
- Infrapedicle level
- Disc level
- Suprapedicle level
PART 3 — TRAVERSING vs. EXITING NERVE ROOTS
The Key Concept
| Term | Definition | Location |
|---|---|---|
| Traversing (transiting) nerve root | The nerve root travelling DOWNWARD through the spinal canal before it exits at a level below | Lateral recess / subarticular zone |
| Exiting nerve root | The nerve root that has left the thecal sac and is passing through the neural foramen at its own level | Foraminal zone |
The Lumbar Rule (Most Important)
| Zone of Herniation | Nerve Root Affected | Clinical Level | Example |
|---|---|---|---|
| Central / Paracentral | Traversing root (one level below) | Level below the disc | L4-L5 central → affects L5 root (traversing) |
| Subarticular / Lateral recess | Traversing root | Level below the disc | L4-L5 subarticular → L5 radiculopathy |
| Foraminal | Exiting root (same level as disc) | Same level as disc | L4-L5 foraminal → L4 radiculopathy |
| Extraforaminal / Far lateral | Exiting root (same level as disc) | Same level as disc | L4-L5 extraforaminal → L4 radiculopathy |
Memory rule: Central/paracentral/subarticular = ONE LEVEL DOWN (traversing root). Foraminal/extraforaminal = SAME LEVEL (exiting root).
Practical Example (L4-L5 disc):
- Paracentral herniation → L5 radiculopathy (foot drop, weak EHL)
- Foraminal herniation → L4 radiculopathy (weak quad, knee jerk reduced)
How to Identify on MRI
- Seen on axial T2 as a dot of intermediate signal in the lateral corner of the spinal canal, between the posterior vertebral body and the facet joint
- Surrounded by bright CSF
- Normally distinct and separate; compression = effacement of surrounding CSF, deviation, or loss of root outline
- Seen on sagittal T1 as a structure surrounded by bright epidural fat within the "keyhole"-shaped foramen
- Normal: fat clearly visible around the root = open foramen
- Abnormal: fat effaced = foraminal stenosis
PART 4 — NERVE ROOT RELATIONSHIP TERMINOLOGY
| Term | What it means | Clinical significance |
|---|---|---|
| Abutting / Contacting | Disc material touches the nerve root but does not deform it | Possible early compression; correlate clinically |
| Indenting | Disc material deforms the surface of the nerve root or thecal sac | More significant; suggests pressure |
| Displacing | Nerve root is shifted from its normal position | Significant compression |
| Compressing | Disc material deforms the nerve root with morphological change | Definite compression; high clinical significance |
PART 5 — SPINAL STENOSIS
Central Canal Stenosis
| Grade | Finding on Axial T2 | Meaning |
|---|---|---|
| 0 - Normal | Nerve rootlets separated, surrounded by CSF | No stenosis |
| 1 - Mild | Nerve rootlets still separated but CSF space reduced | Mild narrowing |
| 2 - Moderate | Some nerve root clumping inside dural sac | CSF partially obliterated |
| 3 - Severe | All nerve roots clumped as single bundle, no separation | Marked stenosis |
- Cord signal change on T2 (in cervical/thoracic) = severe stenosis regardless of morphology
- Mild: <1/3 narrowing
- Moderate: 1/3 to 2/3
- Severe: >2/3
Neural Foraminal Stenosis
| Grade | Finding |
|---|---|
| Normal | "Keyhole" foramen - fat clearly surrounds exiting root |
| Mild | Partial fat effacement, root not deformed |
| Moderate | Fat effaced, root contacted/indented |
| Severe | Root compressed with morphological deformity, or foramen <3mm AP diameter |
- Causes: disc protrusion/extrusion, osteophytes, facet hypertrophy, loss of disc height
- AP diameter <3 mm = diagnostic for foraminal stenosis
Lateral Recess Stenosis
| Grade | Finding |
|---|---|
| 0 | Normal - root bathed in CSF, no contact |
| 1 | Recess narrowed, no root deviation |
| 2 | Recess narrowed + root deviation |
| 3 | Frank root compression with morphological change |
- Lateral recess height <3 mm = significant stenosis
- Lateral recess angle <30° = further evidence of stenosis
PART 6 — ANNULAR FISSURE / TEAR
- T2: Linear bright signal (hyperintense zone / HIZ) within the disc, usually posteriorly
- Post-gadolinium T1: Enhancement from vascularized granulation tissue ingrowth
- Represents a chronic degenerative process (the term "annular tear" is still in common use but "annular fissure" is preferred to avoid implying acute trauma)
| Type | Orientation |
|---|---|
| Radial | Runs from nucleus to periphery (most clinically significant) |
| Transverse | Horizontal, through annular fibres |
| Concentric | Parallel to outer disc contour |
PART 7 — QUICK INTERPRETATION CHECKLIST
- Normal (bright NP)? Mildly degenerate (reduced signal)? Severely degenerate (dark/collapsed)?
- Bulge / protrusion / extrusion / sequestration?
- Focal or broad-based?
- Any annular fissure (HIZ)?
- Central / paracentral / subarticular / foraminal / extraforaminal?
- CSF space preserved? Roots clumped? Grade 0-3?
- In cervical/thoracic: cord deformity? T2 cord signal change?
- Fat surrounding root preserved bilaterally?
- Any effacement = foraminal stenosis
- Abutting / indenting / displacing / compressing?
- Which root: traversing or exiting?
- Correlate with clinical level
- Modic changes? (I = edema, II = fat, III = sclerosis)
- Endplate erosion (infection)?
- Grainger & Allison's Diagnostic Radiology, Chapters 47 & 48 (Spine)
- PMC MRI Spine Review (Safriel et al.)
- Radsource Spine Nomenclature (Combined Task Forces)
- RACGP - Making Sense of MRI Lumbar Spine
- Lee Grading System for Stenosis (KJR/PMC)
Why is it not loading?
-
Slow internet connection - The app relies on a live connection to the AI server. Check your Wi-Fi or mobile data.
-
Server load - High traffic on the platform's servers can cause slow responses or timeouts.
-
Browser/app cache - Stale cache can cause the interface to hang. Try a hard refresh (
Ctrl + Shift + Ron Windows,Cmd + Shift + Ron Mac) or clear your browser cache. -
Browser compatibility - Try a different browser (Chrome, Firefox, Edge) or update your current one.
-
Extensions blocking requests - Ad blockers or privacy extensions can interfere. Try disabling them or opening in an incognito/private window.
-
Large conversation context - Very long conversations (like ours with detailed medical content) can sometimes slow down rendering. Starting a new chat may help.
-
Device performance - Low RAM or an older device can struggle to render complex responses with many images and tables.
- Refresh the page
- Clear cache and cookies
- Open in a new tab or incognito window
- Try on a different device
- Check if the platform has a status page for outages
How to interpret a specific MRI spine finding (disc herniation, stenosis, disc bulge , tranvserse nerve roots, exiting nerve roots, indenting abutting, nerve root compression,tear and everything with images
MRI Spine: Interpreting Specific Findings (with Images)
PART 1 — DISC PATHOLOGY SPECTRUM
Normal Disc (T2 signal)
- Bright nucleus pulposus on T2 = healthy, hydrated disc
- Dark outer annulus on T2 = normal collagen-rich ring
- Disc margin must NOT extend beyond the vertebral apophyses
Disc Bulge vs. Herniation - The Core Distinction
| Disc Bulge | Disc Herniation | |
|---|---|---|
| Circumference involved | >50% (>180°) | <50% (<180°) |
| Annulus | Intact, stretched | Torn or focally deficient |
| Shape | Smooth, diffuse | Focal |
| Nerve root risk | Lower | Higher |
PART 2 — HERNIATION SUBTYPES
2.1 Protrusion
- Base (neck) wider than apex in all planes
- Like a blister that hasn't burst
- Focal (<25% disc circumference) or broad-based (25-50%)
2.2 Extrusion
- Base narrower than the herniated part = "toothpaste sign"
- Can migrate cranially or caudally
- Any herniation extending above/below disc level = extrusion by definition
- Rarely asymptomatic
2.3 Sequestration / Free Fragment
- Completely disconnected from parent disc
- Best term on imaging: "migration" (displacement away from extrusion site)
- Peripheral Gd enhancement on T1 = ongoing resorption → predicts spontaneous regression
Summary Table
| Feature | Bulge | Protrusion | Extrusion | Sequestration |
|---|---|---|---|---|
| Circumference | >50% | <50% focal/broad | <50% | <50% |
| Base vs. apex | N/A | Base > apex | Base < apex | No base (free) |
| Migration | No | No | Yes (cranial/caudal) | Yes (free fragment) |
| Annulus | Intact | Intact/torn | Torn | Disrupted |
| Usually symptomatic | Sometimes | Often | Usually | Usually |
| Spontaneous regression | Rare | Possible | Common | Common |
PART 3 — LOCATION ZONES (Axial Plane)
POSTERIOR
┌─────────────────────────────────┐
│ CENTRAL (midline) │
│ PARACENTRAL (R/L of centre) │
│ SUBARTICULAR / LATERAL RECESS │
│ FORAMINAL (neural foramen) │
│ EXTRAFORAMINAL (far lateral) │
└─────────────────────────────────┘
ANTERIOR
| Zone | Nerve Root Affected | Level |
|---|---|---|
| Central / Paracentral | Traversing root | One level BELOW disc |
| Subarticular / Lateral recess | Traversing root | One level BELOW disc |
| Foraminal | Exiting root | SAME level as disc |
| Extraforaminal / Far lateral | Exiting root | SAME level as disc |
PART 4 — TRAVERSING vs. EXITING NERVE ROOTS
The Anatomy
Thecal sac (dural tube)
│
│ ← Traversing (transiting) root descends inside thecal sac
│ occupies the LATERAL RECESS
│
└──► Exiting root leaves sac, travels through NEURAL FORAMEN
at its own numbered level
Worked Example at L4-L5 Disc
L4 vertebra
└── L4-L5 DISC ──────────────────────────────────
│ │
CENTRAL/PARACENTRAL FORAMINAL/
SUBARTICULAR zone EXTRAFORAMINAL
│ │
L5 root (traversing L4 root (exiting
through L4-L5 recess) through L4-L5 foramen)
│ │
→ L5 RADICULOPATHY → L4 RADICULOPATHY
(foot drop, EHL weak) (knee jerk reduced,
quad weak)
How to Identify on MRI
- Small dot of intermediate signal in the lateral recess
- Should be surrounded by bright CSF
- Sign of compression: CSF effaced around root, root deviated or indistinct
- Seen passing through the "keyhole"-shaped foramen
- Should be surrounded by bright epidural fat
- Sign of foraminal stenosis: fat effaced, root contacted or morphologically deformed
PART 5 — NERVE ROOT RELATIONSHIP TERMINOLOGY
| Term | What it Means | Clinical Weight |
|---|---|---|
| Abutting / Contacting | Disc touches root - no deformation | Low - correlate clinically |
| Indenting | Disc deforms the surface of root or thecal sac | Moderate - likely significant |
| Displacing | Root shifted from normal position | Significant |
| Compressing | Root deformed with morphological change | Definite compression |
Critical caveat: Many herniations seen on MRI are asymptomatic. A disc "indenting" a root in a pain-free patient does not mean that finding is the cause of symptoms. Always correlate with the clinical level.
PART 6 — SPINAL STENOSIS
Central Canal Stenosis - Lee Grading (Axial T2)
| Grade | Finding | Notes |
|---|---|---|
| 0 - Normal | All nerve rootlets separated, bathed in CSF | No stenosis |
| 1 - Mild | CSF reduced but roots still separated | <1/3 canal narrowed |
| 2 - Moderate | Some root clumping inside dural sac | 1/3 to 2/3 narrowed |
| 3 - Severe | All roots clumped as single bundle, no separation | >2/3 narrowed |
Neural Foraminal Stenosis (Sagittal T1)
| Grade | Finding |
|---|---|
| Normal | Full "keyhole" foramen with fat clearly around root |
| Mild | Partial fat effacement, root not deformed |
| Moderate | Fat effaced, root contacted/indented |
| Severe | Root compressed + morphological change, or AP diameter <3 mm |
Lateral Recess Stenosis - Bartynski Grading (Axial T2)
| Grade | Finding |
|---|---|
| 0 | Normal - root bathed in CSF, no contact with walls |
| 1 | Recess narrowed, no root deviation |
| 2 | Recess narrowed + root deviation |
| 3 | Frank root compression with morphological change |
- Lateral recess height <3 mm = stenosis
- Lateral recess angle <30° = further evidence
PART 7 — ANNULAR FISSURE / TEAR
- T2: Bright linear signal (HIZ = High Intensity Zone) in posterior disc
- Post-Gd T1: Enhancement (granulation tissue / vascular ingrowth)
| Type | Orientation | Significance |
|---|---|---|
| Radial | Nucleus to periphery | Most significant - can transmit pain |
| Transverse | Horizontal | Moderate |
| Concentric | Parallel to outer disc | Usually incidental |
Preferred modern term: "annular fissure" (chronic degenerative) rather than "tear" (which implies acute trauma). Both terms are in common use.
PART 8 — SYSTEMATIC READING CHECKLIST
1. DISC SIGNAL (sag T2)
→ Normal bright? Mild degenerate? Severe dark/collapsed?
2. DISC CONTOUR (sag + axial T2)
→ Bulge / protrusion / extrusion / sequestration?
→ Focal or broad-based?
→ Any annular fissure (HIZ)?
3. LOCATION (axial T2)
→ Central / paracentral / subarticular / foraminal / extraforaminal?
4. CENTRAL CANAL (axial T2)
→ CSF preserved? Root clumping? Grade 0-3?
→ Cord signal change? (cervical/thoracic)
5. NEURAL FORAMINA (sag T1 both sides)
→ Fat around exiting root preserved?
→ Effaced = foraminal stenosis → grade it
6. NERVE ROOT RELATIONSHIP
→ Abutting / indenting / displacing / compressing?
→ Traversing or exiting root?
→ Does it match the clinical dermatomal level?
7. ENDPLATES (sag T1 + T2 + STIR)
→ Modic type I/II/III?
→ Erosion (infection)? Fracture? Schmorl's node?
- Grainger & Allison's Diagnostic Radiology (Chapters 47 & 48)
- PMC - MRI of the Spine
- Radsource Spine Nomenclature (Combined Task Forces)
- RACGP - Making Sense of Lumbar Spine MRI
- Lee Grading System for Stenosis - KJR