Case control study 15 mark
Asking for Preferences
Reading File
Searching the Web
case control study epidemiology design advantages disadvantages odds ratio
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have everything needed from Park's textbook. Here is a complete, exam-ready 15-mark answer.
Case-Control Study - 15 Mark Exam Answer
(Based on Park's Textbook of Preventive and Social Medicine)
Definition
A case-control study (also called a retrospective study or case-referent study) is an observational epidemiological study design in which a group of individuals with a disease (cases) is compared with a group without the disease (controls) to identify past exposures or risk factors that may be responsible for the disease. Both the exposure and the outcome have already occurred before the study begins, and the inquiry proceeds backwards from effect to cause.
The case-control method has three distinct features:
- Both exposure and outcome (disease) have occurred before the start of the study
- The study proceeds backwards - from effect to cause
- It uses a control group to support or refute an inference
Design
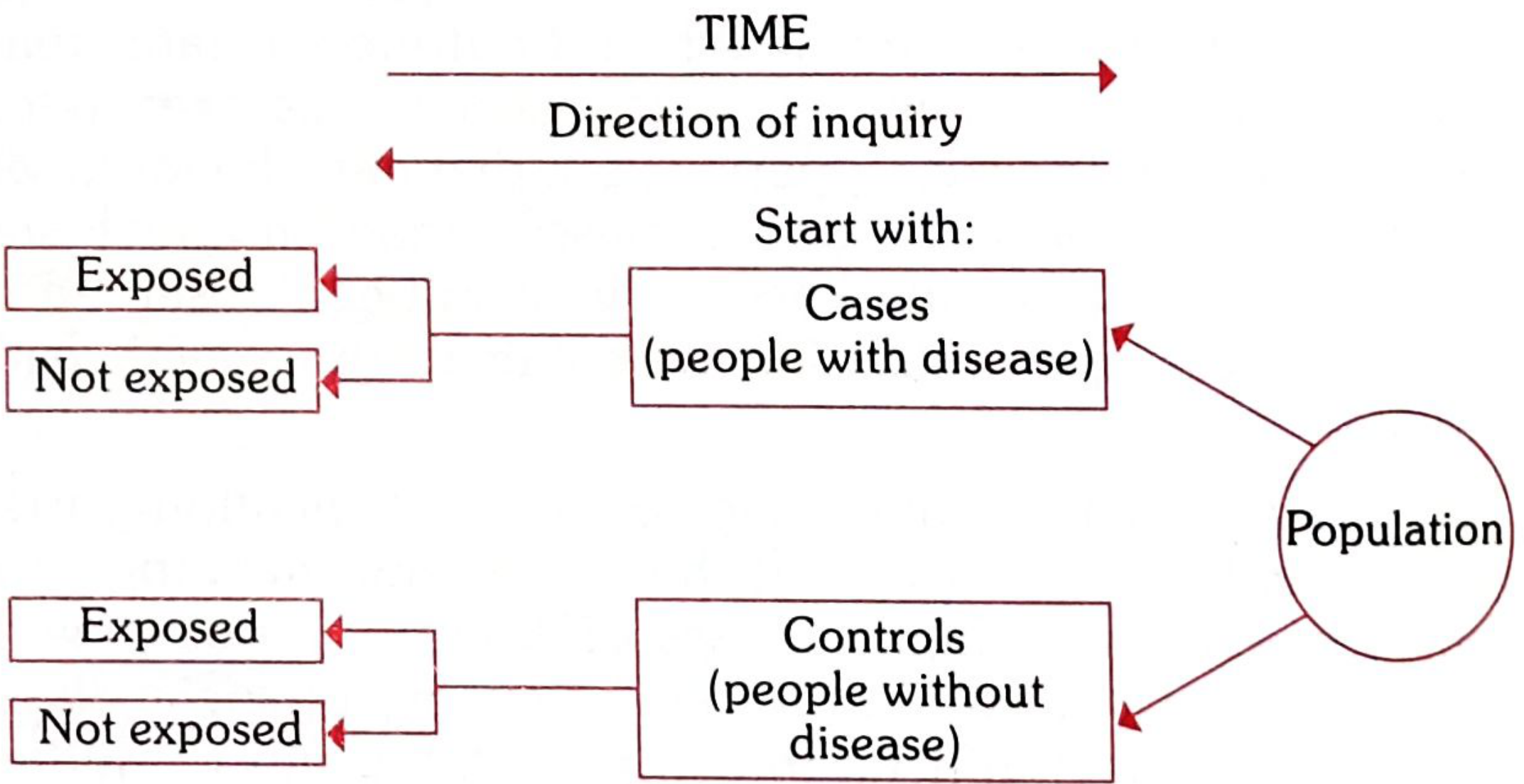
Fig: Schematic diagram of case-control study design - Park's Textbook of Preventive and Social Medicine
The basic framework is a 2 × 2 contingency table:
| Suspected Risk Factor | Cases (Disease Present) | Controls (Disease Absent) |
|---|---|---|
| Present | a | b |
| Absent | c | d |
| Total | a+c | b+d |
Steps in Conducting a Case-Control Study
There are four basic steps:
1. Selection of Cases and Controls
(a) Selection of Cases
- Diagnostic criteria must be defined before the study (e.g., histologically confirmed cancer). These criteria must not be altered during the study.
- Eligibility criteria: Newly diagnosed (incident) cases within a specified period are preferred over prevalent/old cases, as prevalent cases may reflect survival rather than disease onset.
- Sources: Cases may be drawn from hospitals (hospital-based) or from the general population via disease registries or surveys (population-based).
(b) Selection of Controls
- Controls must be free from the disease under study.
- They must be as similar to the cases as possible except for the absence of the disease.
- Sources of controls include: hospital patients with other conditions, general population, relatives, neighbours, or occupational groups.
- A key rule: controls should be subjects who might have been cases in the study but are selected independent of the exposure.
2. Matching
Matching is the process of selecting controls who are similar to cases in pertinent variables (e.g., age, sex, occupation, social status) that could confound the results.
A confounding factor is one associated both with exposure and disease, distributed unequally between cases and controls. Examples:
- Smoking is a confounder in a study of alcohol and oesophageal cancer (since smokers tend to drink and smoking independently causes cancer)
- Age is a confounder in a study of oral contraceptives and breast cancer
Types of matching:
- Group (frequency) matching: Cases and controls are matched in strata so the frequency distribution of matched variables is similar in both groups.
- Individual (pair) matching: For each case, one control is selected that closely matches on chosen variables (e.g., same age, sex, occupation). Analysis of matched pairs uses McNemar's test.
Important note: The suspected aetiological factor itself must NOT be matched, as doing so would eliminate its aetiological role in the study.
3. Measurement of Exposure
- Information on past exposure must be obtained in exactly the same manner for both cases and controls.
- Methods include interviews, questionnaires, medical records, and biological specimens.
- Exposure data is collected retrospectively, which introduces the risk of recall bias.
4. Analysis and Interpretation - Odds Ratio (OR)
In case-control studies, incidence rates cannot be calculated because groups are defined by disease status, not population at risk. Therefore, the measure of association used is the Odds Ratio (OR):
OR = ad / bc
Where:
- a = cases exposed
- b = controls exposed
- c = cases not exposed
- d = controls not exposed
Interpretation:
- OR = 1: No association
- OR > 1: Positive association (risk factor)
- OR < 1: Negative association (protective factor)
The OR is a good estimate of relative risk (RR) when the disease is rare in the general population (rare disease assumption).
Example from lung cancer study:
| Cases | Controls | |
|---|---|---|
| Smokers (<5 cigs/day) | 33 | 55 |
| Non-smokers | 2 | 27 |
OR = (33 × 27) / (55 × 2) = 8.1
Smokers of <5 cigarettes/day had 8.1 times the odds of lung cancer compared to non-smokers.
Bias in Case-Control Studies
| Type of Bias | Description |
|---|---|
| Recall (Memory) bias | Cases more likely to recall past exposures than healthy controls, since illness motivates retrospective scrutiny |
| Selection bias | Cases and controls may not represent the general population |
| Berkesonian bias | Arises when hospital-based studies have differential admission rates for different diseases |
| Confounding bias | Confounder distorts the true association; controlled by matching or stratified analysis |
| Interviewer bias | Interviewer knowing the hypothesis may question cases more rigorously than controls; prevented by blinding |
Advantages of Case-Control Studies
- Relatively easy to carry out
- Rapid and inexpensive compared to cohort studies
- Require few subjects
- Particularly suited to rare diseases (e.g., leukaemia in adolescents)
- No risk to subjects (no intervention)
- Allows study of multiple aetiological factors simultaneously (e.g., smoking, physical activity, personality in MI)
- Can identify risk factors to guide prevention programmes
- No attrition problems - no follow-up required
- Minimal ethical issues
Disadvantages
- Prone to bias - relies on memory or past records of uncertain accuracy
- Selection of controls is often difficult
- Cannot measure incidence rates - only OR (estimated RR)
- Does not easily distinguish causes from associations
- Not suited to evaluation of therapy or prophylaxis
- Representativeness of both cases and controls may be questionable
Classic Examples
-
Cigarette smoking and lung cancer - Doll and Hill (1950): First landmark case-control study showing a strong association between smoking and lung cancer.
-
DES and vaginal adenocarcinoma: 8 young women (15-22 years) with vaginal adenocarcinoma were compared with 32 matched controls. Seven of the 8 cases had been exposed to diethyl-stilboestrol (DES) in foetal life vs. none of the controls (p<0.00001), revealing DES as the cause 10-20 years after in utero exposure.
-
Oral contraceptives and thromboembolic disease - Vassey and Doll (1968-69): 50% of 84 women with venous thrombosis/pulmonary embolism had used oral contraceptives vs. only 14% of controls; relative risk 6.3:1.
-
Thalidomide and congenital malformations: Retrospective study of 46 mothers of deformed babies showed 41 had taken thalidomide in the first trimester.
Summary Table: Case-Control vs. Cohort Study
| Feature | Case-Control | Cohort |
|---|---|---|
| Direction | Retrospective (effect → cause) | Prospective (cause → effect) |
| Starts with | Disease status | Exposure status |
| Measure | Odds Ratio | Relative Risk / Incidence Rate |
| Time | Short | Long |
| Cost | Low | High |
| Best for | Rare diseases | Common diseases |
| Bias risk | High (recall bias) | Lower |
Source: Park's Textbook of Preventive and Social Medicine, pp. 83-87
Define epidemic discuss the steps of investigation in epidemic
Finding Sources
Searching the Web
steps of epidemic investigation epidemiology outbreak investigation
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have all 10 steps from Park's and the full definition. Let me compile the complete answer.
Epidemic - Definition and Steps of Investigation
(Source: Park's Textbook of Preventive and Social Medicine)
DEFINITION OF EPIDEMIC
(From the Greek: Epi = upon, demos = people)
An epidemic is defined as "the occurrence in a community or region of cases of an illness, specific health-related behaviour, or other health-related events clearly in excess of normal expectancy." The community or region and the period in which the cases occur must be specified precisely.
Key points in the definition:
- Epidemicity is relative - it depends on the usual frequency of the disease in the same area, among the specified population, at the same season of the year
- The number of cases indicating an epidemic varies according to: the agent, size and type of population exposed, previous immunity, time, and place
- Even a single case of a communicable disease long absent from a population may require immediate investigation and reporting
- Two cases associated in time and place of a disease not previously recognized in an area may be sufficient to constitute an epidemic
Related Terms
| Term | Definition |
|---|---|
| Endemic | Constant presence of a disease within a geographic area without importation from outside (e.g., common cold) |
| Epidemic | Disease occurrence clearly in excess of normal expectancy |
| Pandemic | An epidemic occurring over a very wide area, crossing international boundaries, usually affecting large numbers (e.g., influenza pandemics, COVID-19) |
| Sporadic | Cases occurring irregularly, infrequently, with no connection to a common source (e.g., tetanus, herpes zoster) |
| Hyperendemic | Constantly high incidence/prevalence affecting all age groups equally |
| Holoendemic | High infection levels beginning early in life; adults show disease less commonly (e.g., malaria) |
OBJECTIVES OF EPIDEMIC INVESTIGATION
Before the steps, it is important to understand why we investigate. The objectives are:
- To define the magnitude of the epidemic in terms of time, place, and person
- To determine the conditions and factors responsible for its occurrence
- To identify the cause, source of infection, and mode of transmission to guide control measures
- To make recommendations to prevent recurrence
STEPS OF INVESTIGATION OF AN EPIDEMIC
The epidemic investigation calls for both description and inference. While these steps are presented in logical order, several can be carried out concurrently in practice.
Step 1: Verification of Diagnosis
This is the first and essential step. Reports of epidemics may sometimes be spurious, arising from misinterpretation of signs and symptoms by the lay public or field workers.
- A clinical examination of a sample of cases is sufficient - not every case needs examination
- Laboratory investigations (wherever applicable) are most useful to confirm the diagnosis
- Epidemiological investigations should NOT be delayed until laboratory results are available - both proceed in parallel
Step 2: Confirmation of the Existence of an Epidemic
The next step is to confirm whether an epidemic actually exists by comparing current disease frequency with that of previous years during the same period.
- An epidemic is said to exist when the observed frequency exceeds the expected frequency based on past experience
- An arbitrary limit of two standard errors above endemic occurrence is used as the epidemic threshold for common diseases (e.g., influenza)
- Some epidemics are easily recognised (common-source epidemics of cholera, food poisoning, hepatitis A)
- Modern epidemics (cancer, cardiovascular diseases) may not be easily recognised without comparison to previous data
Step 3: Defining the Population at Risk
(a) Obtaining a map of the area:
- A detailed and current map of the area must be available before investigation begins
- The map should show: natural landmarks, roads, locations of all dwelling units
- The area is divided into segments using natural landmarks as boundaries, then subdivided further
(b) Counting the population (denominator):
- A complete census of the population by age and sex is carried out via house-to-house visits
- Lay health workers can be employed for this purpose
- Without an appropriate denominator of "population at risk," attack rates cannot be calculated
- Attack rates help identify risk factors and subgroups most affected
Step 4: Rapid Search for All Cases and Their Characteristics
(a) Medical survey:
A survey is carried out in the defined area to identify all cases, including those who have not sought medical care and those possibly exposed to risk.
(b) Epidemiological case sheet:
The investigator uses an "epidemiological case sheet" or "case interview form" to collect:
- Name, age, sex, occupation, social class, travel history
- History of previous exposure and immunity status
- Time of onset, signs and symptoms
- Personal contacts (home, work, school)
- Special events (parties attended, foods eaten, water and milk exposure)
- History of injections, blood products, or attendance at large gatherings
(c) Searching for more (secondary) cases:
- Patients are asked if they know of other cases in the home, family, neighbourhood, school, or workplace with onset within the incubation period of the index case
- Hospital records are also checked
- The search for new cases continues every day until the area is declared free of the epidemic - usually for a period equal to twice the incubation period after the last case
Step 5: Data Analysis
Data is analyzed on an ongoing basis using the classical epidemiological parameters - Time, Place, and Person (or the Agent-Host-Environment model).
(a) Time - Epidemic Curve:
- Prepare a chronological distribution of dates of onset - construct an "epidemic curve"
- The epidemic curve can suggest:
- A time relationship with exposure to a suspected source
- Whether it is a common-source (single sharp peak) or propagated (multiple successive peaks) epidemic
- Seasonal or cyclic patterns suggesting a particular infection
- The shape of the epidemic curve helps estimate the incubation period and the likely time of exposure
(b) Place - Spot Map:
- Prepare a "spot map" showing the geographic distribution of cases
- Clustering of cases in a particular area points to a localised source (e.g., contaminated water supply, food establishment)
(c) Person:
- Analyse data by age, sex, occupation, and other risk factors
- Calculate attack rates and case fatality rates for those exposed and not exposed
- In food-borne outbreaks, food-specific attack rates must be calculated for each food eaten to identify the vehicle of infection
- The purpose is to identify the common event or experience that delineates the group involved
Step 6: Formulation of Hypotheses
Based on the time-place-person analysis (or Agent-Host-Environment model), formulate hypotheses to explain the epidemic in terms of:
- Possible source of infection
- Causative agent
- Possible modes of spread
- Environmental factors that enabled it to occur
Hypotheses are placed in order of relative likelihood, and a tentative hypothesis guides further investigation.
Step 7: Testing of Hypotheses
All reasonable hypotheses must be weighed and compared by calculating attack rates in various groups - those exposed vs. not exposed to each suspected factor.
- The hypothesis that is consistent with all known facts is retained
- When divergent theories arise, distinguish between those that are sound and those that are merely plausible by looking at evidence from the subsequent course of events
- Statistical methods (chi-square, odds ratio) may be used to test the strength of associations
Step 8: Evaluation of Ecological Factors
The environmental circumstances that made the epidemic possible are investigated:
- Sanitary status of eating establishments
- Water supply and milk supply systems; breakdown in supply
- Movements of human population
- Atmospheric changes (temperature, humidity, air pollution)
- Population dynamics of insects and animal reservoirs
The outbreak may be studied in a case-control fashion to relate disease to environmental factors and identify sources of infection, reservoirs, and modes of transmission.
Step 9: Further Investigation of the Population at Risk
A study of the population at risk (or a sample of it) may be needed to obtain additional information:
- Medical examination and screening tests
- Examination of suspected food, faeces, or blood samples
- Biochemical studies
- Assessment of immunity status
- Serological study may reveal clinically inapparent (subclinical) cases and throw light on pathogenesis
- Healthy individuals from the same area are studied in a case-control fashion to classify all members as: (a) exposed to potential vehicles, and (b) whether ill or not
Step 10: Writing the Report
The final report must be complete and convincing, and should include:
| Section | Contents |
|---|---|
| Background | Geography, climate, demographics, health services, disease prevalence |
| Historical data | Previous epidemics, related diseases in same/other areas, first cases of present outbreak |
| Methodology | Case definition, questionnaire, survey teams, laboratory techniques |
| Data Analysis | Clinical data (signs, symptoms, CFR), epidemiological data (time, place, person), mode of transmission, sources of infection |
| Control measures | Measures taken, evaluation of their effectiveness |
| Recommendations | Steps to prevent recurrence, surveillance improvements |
Summary: 10 Steps at a Glance
| Step | Action |
|---|---|
| 1 | Verification of diagnosis |
| 2 | Confirmation of epidemic existence |
| 3 | Defining the population at risk |
| 4 | Rapid search for all cases and their characteristics |
| 5 | Data analysis (Time - Place - Person) |
| 6 | Formulation of hypotheses |
| 7 | Testing of hypotheses |
| 8 | Evaluation of ecological factors |
| 9 | Further investigation of population at risk |
| 10 | Writing the report |
Source: Park's Textbook of Preventive and Social Medicine, pp. 106, 151-152
Cold chain system 5 mark
Finding Sources
Searching the Web
cold chain system vaccines immunization levels equipment WHO
Reading File
Reading File
Reading File
Loading Image
Reading File
All the content is in hand. Here is the focused 5-mark answer.
Cold Chain System - 5 Mark Answer
(Source: Park's Textbook of Preventive and Social Medicine)
Definition
The cold chain is a system of storage and transport of vaccines at low temperature from the manufacturer to the actual vaccination site, ensuring that vaccine potency is maintained throughout.
The success of a national immunization programme is highly dependent on a supply chain that meets the "6 Rights":
The right vaccine - in the right quantity - at the right place - at the right time - in the right condition (no temperature breaks) - and at the right cost.
Why is it Necessary?
Vaccines are sensitive biological products. Vaccine potency (its ability to adequately protect the patient) can diminish when exposed to inappropriate temperatures. Once lost, vaccine potency cannot be regained. Vaccine failure may occur due to failure to store and transport under strict temperature controls, leading to vaccine-preventable diseases in populations thought to be immunized.
Temperature Sensitivities
| Sensitivity | Vaccines Affected |
|---|---|
| Heat sensitive (most) | OPV (Group A) > Influenza > IPV, Measles, BCG > Hep B |
| Freeze sensitive | DPT, TT, Td, Hep B, IPV, Pentavalent, Pneumococcal, HPV, Rotavirus |
| Light sensitive | BCG, Measles, MR, MMR, Rubella |
Recommended storage temperature: +2°C to +8°C for most vaccines
Levels of the Cold Chain
The cold chain operates at multiple levels from national to community:
| Level | Storage Equipment | Temperature |
|---|---|---|
| National / State | Walk-in-Freezer (WIF), Walk-in-Cooler (WIC) | -15 to -25°C / +2 to +8°C |
| District | Ice-Lined Refrigerator (ILR), Deep Freezer (DF) | +2 to +8°C / -15 to -25°C |
| Sub-district / PHC | ILR, Deep Freezer | +2 to +8°C |
| Field / outreach | Cold box, Vaccine carrier with ice packs | +2 to +8°C |
Cold Chain Equipment
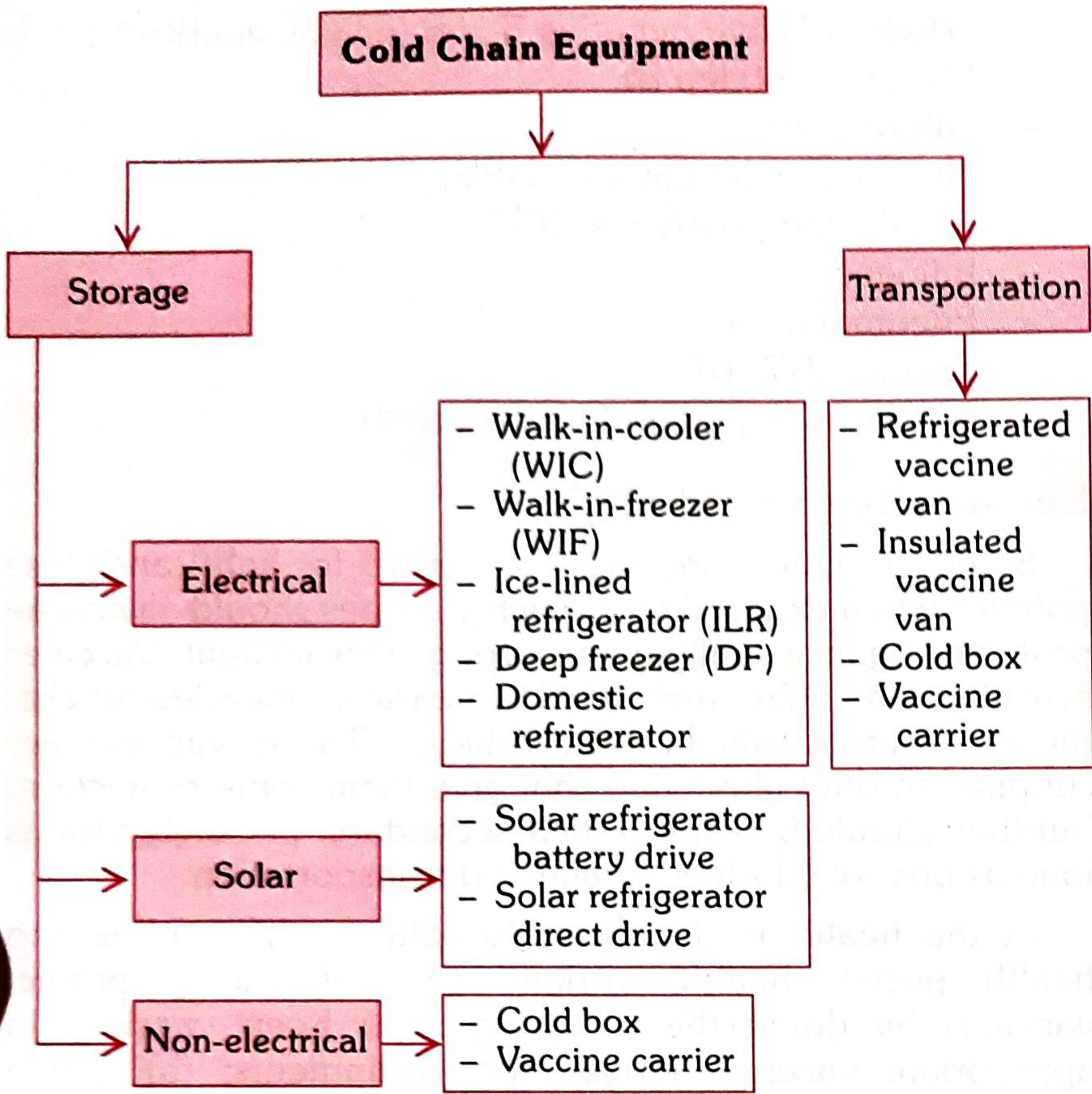
Fig: Classification of cold chain equipment - Park's Textbook of Preventive and Social Medicine
Storage Equipment
1. Walk-in-Freezer (WIF)
- Pre-fabricated polyurethane foam insulated cold room
- Temperature: -15°C to -25°C
- Has standby generator (auto-starts on power cut)
- Used at national/state level for bulk OPV storage and ice pack preparation
2. Walk-in-Cooler (WIC)
- Similar construction to WIF
- Temperature: +2°C to +8°C
- Used for storage of all UIP vaccines at national/state level
3. Deep Freezer (DF)
- Top-opening lid (prevents cold air loss)
- Temperature: -15°C to -25°C
- Stores OPV at district level; also freezes ice packs at sub-district level
4. Ice-Lined Refrigerator (ILR)
- Most important link in the cold chain
- Temperature: +2°C to +8°C
- Top-opening design retains cold air better than front-opening fridges
- Has a lining of frozen water containers around walls - maintains safe temperature for minimum 8 hours without electricity
- Used at district and sub-district (PHC) level
5. Solar refrigerators - battery drive and direct drive types; used in areas with unreliable electricity
Transportation Equipment
- Refrigerated/insulated vaccine vans - for district to sub-district transport
- Cold boxes - passive insulated containers; carry vaccines for 3-5 days with ice packs
- Vaccine carriers - smaller portable containers for field/outreach sessions; maintain +2°C to +8°C for 6-8 hours
Vaccine Vial Monitor (VVM)
A VVM is a heat-sensitive label attached to each vaccine vial. It changes colour irreversibly when the vaccine has been exposed to excessive heat, indicating the vaccine should be discarded. VVMs are a critical tool for monitoring cold chain integrity at the point of use.
Key Points for Cold Chain Maintenance
- Temperatures must be checked and recorded twice daily (morning and end of session)
- Freeze-sensitive vaccines (DPT, TT, Hep B) must be stored in the upper basket of the ILR - never on the floor
- Heat-sensitive vaccines (OPV, BCG, Measles) are kept at the bottom
- Vaccines should never be kept directly on the floor of the refrigerator
- One designated person at each health facility must have overall responsibility for the cold chain
Source: Park's Textbook of Preventive and Social Medicine, pp. 121-124
This is a shared conversation. Sign in to Orris to start your own chat.