BPH in detail
Reading File
Finding Sources
Searching PubMed
"benign prostatic hyperplasia"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple major textbooks. Let me compile the full detailed response.
Benign Prostatic Hyperplasia (BPH)
1. Definition and Overview
Benign prostatic hyperplasia (BPH) is a benign proliferation of both stromal and glandular elements of the prostate, originating specifically in the periurethral transition zone. It is a histologic diagnosis defined by the proliferation of smooth muscle and epithelial cells within the prostatic transition zone that results in enlargement - formally defined as a calculated prostate volume exceeding 30 mL.
Normal prostate volume in young men is ~20 mL, rising to an average of 24-38 mL between ages 50-80. The degree of enlargement that causes symptoms is highly variable and does not correlate tightly with prostate volume.
- Robbins & Kumar Basic Pathology
- Goldman-Cecil Medicine
2. Anatomy of the Prostate
The prostate is composed of four zones:
- Peripheral zone - largest; site of most prostate cancers
- Central zone - surrounds ejaculatory ducts
- Transition zone - surrounds the proximal urethra; site of BPH
- Anterior fibromuscular stroma
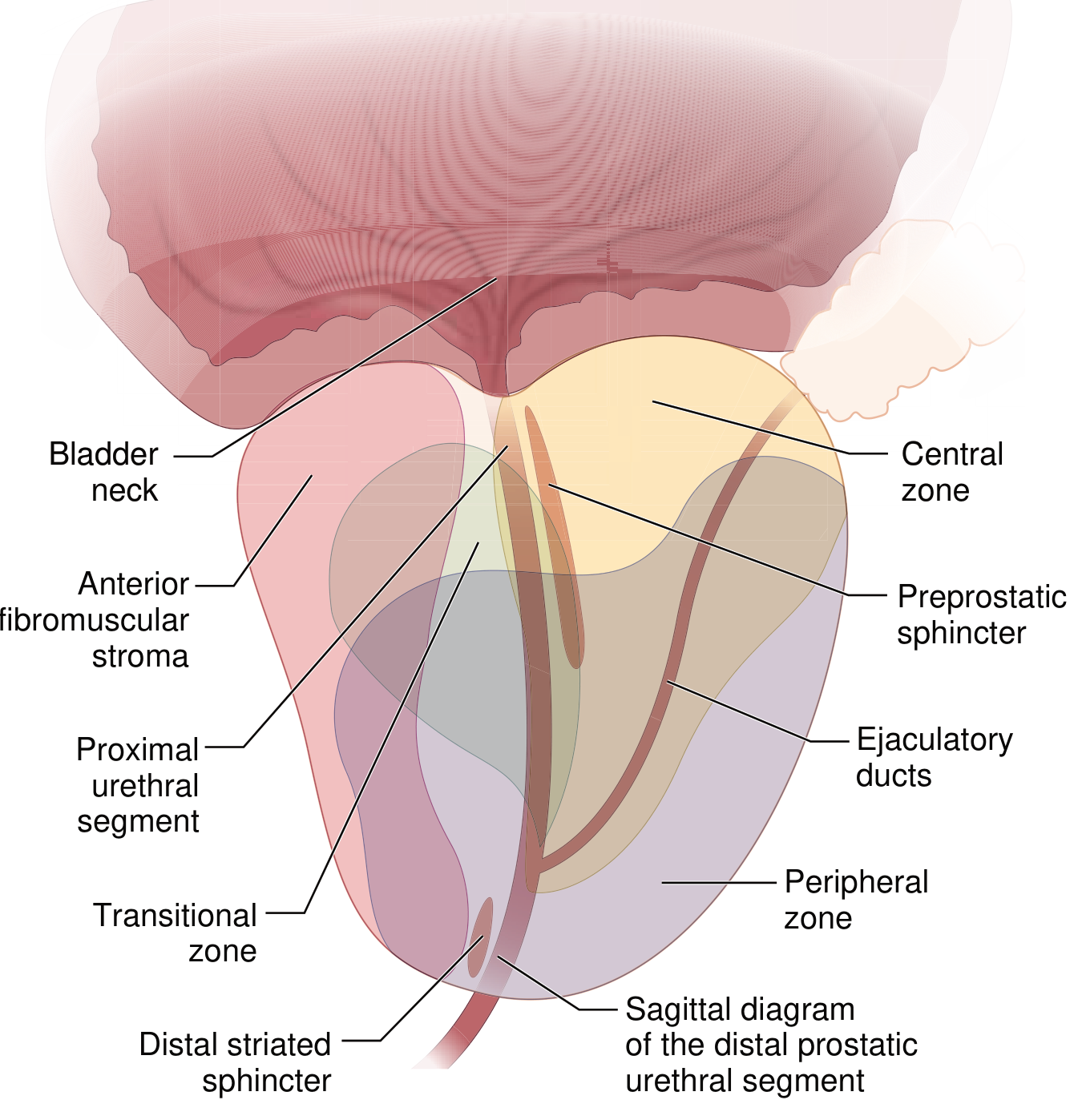
Figure: Zones of the prostate (Goldman-Cecil Medicine)
3. Epidemiology
-
Histologic BPH develops in approximately 50% of men over age 50 and 90% of men in their 80s
-
Of those with histologic BPH, approximately 50% develop clinically significant lower urinary tract symptoms (LUTS)
-
BPH affects approximately 70% of males between ages 60-69
-
LUTS prevalence increases linearly between ages 40 and 80
-
Age is the single strongest risk factor
-
Goldman-Cecil Medicine; Sabiston Textbook of Surgery
4. Pathogenesis
Hormonal Mechanism
The key driver is DHT (dihydrotestosterone):
- Circulating testosterone is converted to DHT within prostatic stromal cells by the enzyme 5α-reductase type 2
- DHT is 10x more potent than testosterone
- DHT binds nuclear androgen receptors, regulating genes that support growth and survival of both prostatic epithelium and stromal cells
- DHT-induced growth factors increase stromal cell proliferation and decrease epithelial cell apoptosis
BPH does not occur in men castrated before puberty or in those with genetic diseases blocking androgen activity.
Role of Estrogen
With aging, testosterone levels decline while estrogen levels remain unchanged (or increase via peripheral conversion of androgens). Estrogens act synergistically with DHT to drive growth, because both epithelial and stromal cells express estrogen receptors.
Bladder Outlet Obstruction Mechanism
An enlarged prostate causes LUTS by:
- Directly obstructing urinary outflow (mechanical component)
- Increasing smooth muscle tone of the prostate and bladder neck (dynamic component)
- Triggering overactive detrusor function in response to obstruction, causing storage symptoms
Changes in vascularity of the prostate and bladder wall also contribute.
- Robbins & Kumar; Goldman-Cecil Medicine
5. Pathology (Gross and Microscopic)
Gross Appearance
- Prostate weight increases 3- to 5-fold (60-100 g or more)
- BPH arises from the transition zone, compressing the urethra to a slit-like orifice
- Cross-section shows hyperplastic nodules that vary in color and consistency
- Nodules may be solid or contain cystic spaces (dilated glands)
Microscopic Appearance
- Variable proportions of proliferating glandular elements and fibromuscular stroma
- Hyperplastic glands are lined by two cell layers:
- Inner: tall, columnar epithelial cells
- Outer: flattened basal cells (KEY distinguishing feature from prostate carcinoma, which lacks basal cells)
- Glandular lumina often contain corpora amylacea (laminated proteinaceous secretory material)
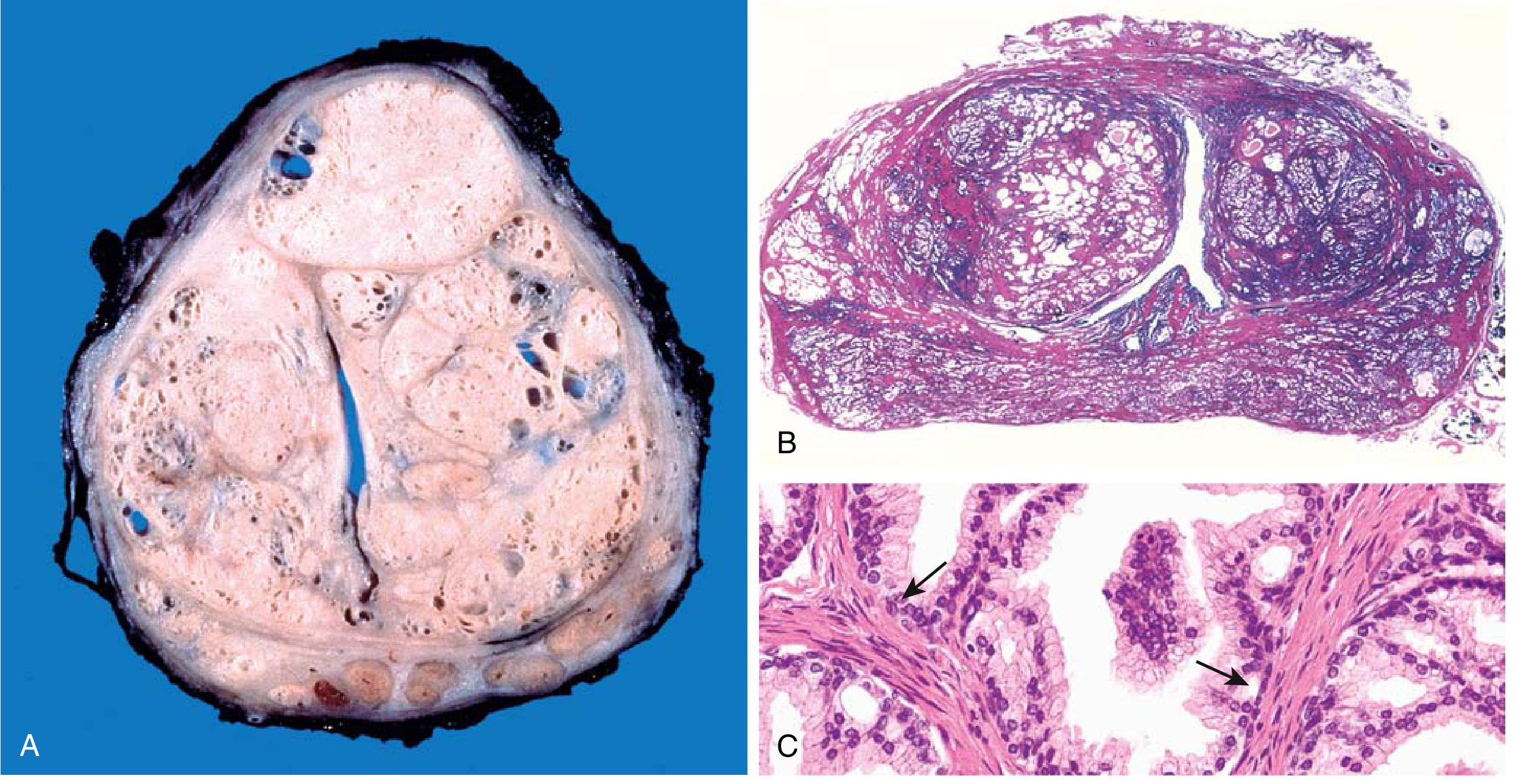
Figure: BPH pathology. (A) Gross cross-section: nodules compressing urethra into a slit-like lumen. (B) Low-power: nodules on both sides of urethra. (C) High-power: papillary infoldings with basal cells (arrows) - distinguishing from carcinoma. (Robbins & Kumar)
6. Clinical Features
Symptoms - Classified into Three Categories
| Category | Symptoms |
|---|---|
| Voiding (obstructive) | Hesitancy, weak/interrupted stream, straining to void, prolonged voiding, terminal dribbling |
| Storage (irritative) | Urgency, frequency, nocturia, urge incontinence, small voided volumes |
| Post-micturition | Post-void dribble, sensation of incomplete emptying |
Most patients present with a mix of all three categories.
Complications of Chronic Obstruction
- Bladder hypertrophy and distension (trabeculation, diverticula)
- Residual urine - culture medium for bacteria
- Recurrent urinary tract infections
- Bladder calculi
- Hydronephrosis (bilateral) from chronic retention
- Acute urinary retention - a urologic emergency
- Chronic renal insufficiency from long-standing bilateral hydroureteronephrosis
- Hematuria
Note: There is little correlation between prostate volume and the severity of symptoms or degree of obstruction.
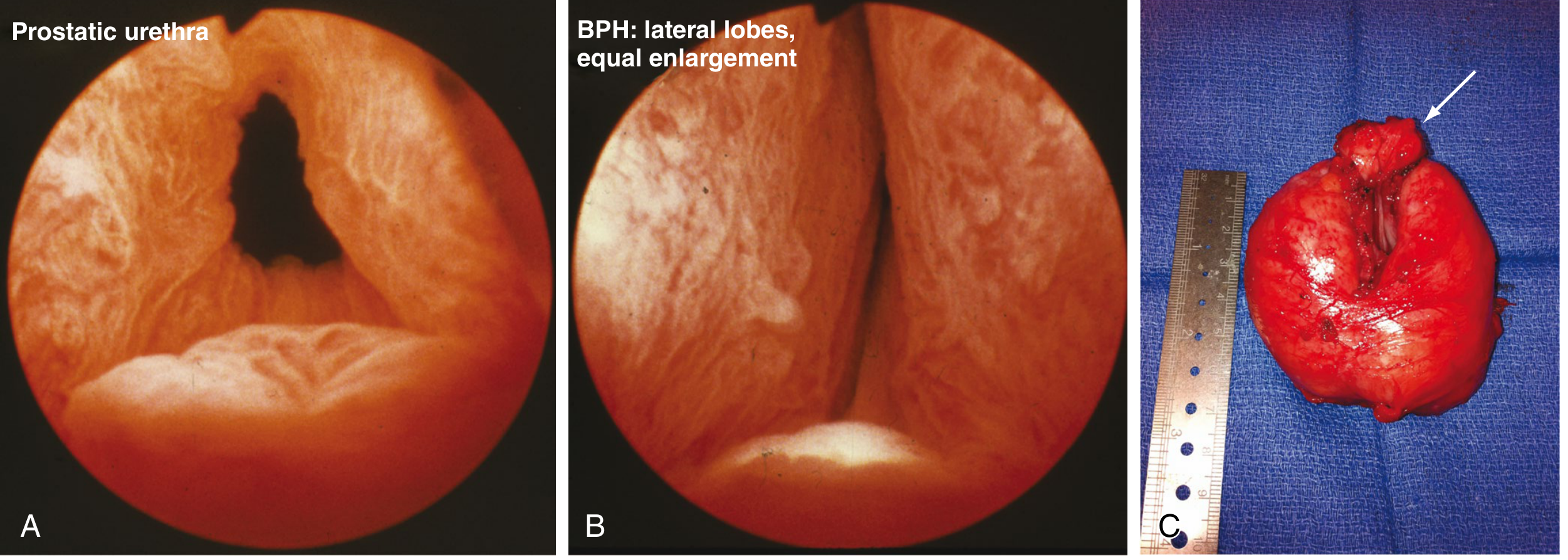
Figure: BPH appearances. (A) Normal prostatic urethra cystoscopically. (B) Moderate BPH - lateral lobe enlargement. (C) 130g prostatic adenoma after open prostatectomy with small medial lobe (arrow). (Sabiston)
7. Diagnosis and Evaluation
History
- Symptom assessment using the International Prostate Symptom Score (IPSS)
- Medications review: diuretics, nasal decongestants, antihistamines can worsen symptoms
- Dietary factors: caffeine, alcohol, artificial sweeteners, fluid intake
Physical Examination
- Digital rectal examination (DRE) - assesses prostate size and nodularity; only the posterior half is palpable, giving an approximate estimate
- Abdominal examination - palpable bladder suggests retention
- Focused neurologic examination (mental status, lower extremity function, anal sphincter tone)
Laboratory Tests
- Urinalysis - screen for hematuria, UTI
- PSA - in appropriate patients (life expectancy >10 years); correlates with prostate volume and predicts symptom progression; 5α-reductase inhibitors reduce PSA by ~50%
- Serum creatinine - assess for renal insufficiency
Objective Urological Tests
- Uroflowmetry - measure maximum urinary flow rate
- Post-void residual (PVR) ultrasound
- Prostate volume by transabdominal or transrectal ultrasound
- Cystoscopy - if hematuria is present or prior to minimally invasive procedures
- Urodynamic studies - if diagnosis is in question
Differential Diagnosis to Consider
- Prostate cancer
- Bladder cancer (especially with hematuria)
- Urethral stricture
- Bladder stones
- Neurogenic bladder (Parkinson disease, multiple sclerosis, diabetes)
- Overactive bladder
8. Treatment
Treatment follows the AUA Guidelines (2023 amendment) and aims to improve symptoms/quality of life and prevent disease progression.
Step 1: Watchful Waiting / Behavioral Therapy
- For IPSS ≤ 7 (mild symptoms) or moderately symptomatic but not bothered
- Measures include: fluid restriction, timed voiding, double voiding, caffeine/alcohol reduction
Step 2: Medical Therapy
A. α1-Adrenergic Receptor Blockers (First-Line)
- Mechanism: relax smooth muscle in bladder neck and prostate, reducing outflow resistance
- Selective α1a subtype blockers preferred (prostate-specific)
- Examples: tamsulosin, alfuzosin, silodosin, terazosin, doxazosin
- Onset of action: rapid (days)
- Side effects: orthostatic hypotension, retrograde ejaculation, rhinitis, floppy iris syndrome (discontinue before cataract surgery)
B. 5α-Reductase Inhibitors (5-ARIs)
- Mechanism: block conversion of testosterone → DHT, reducing prostate glandular volume
- Examples: finasteride (5-ARI type 2), dutasteride (dual 5-ARI types 1 and 2; evidence suggests dutasteride preferred)
- Onset: slow (months for full effect)
- Reduces prostate volume, episodes of acute urinary retention, and need for surgery
- Most effective for larger prostates (>30 mL)
- Side effects: erectile dysfunction, reduced libido, decreased ejaculate volume
- Reduces PSA by ~50% (must be accounted for in cancer screening)
C. Phosphodiesterase Type 5 Inhibitors (PDE5i)
- Example: tadalafil (daily dosing approved for BPH)
- Useful in patients who also have erectile dysfunction
- Can be used as initial therapy in such patients
D. Antimuscarinics
- Target muscarinic receptors in the bladder to reduce overactivity
- Examples: tolterodine, solifenacin, fesoterodine
- Used for storage symptoms/overactive bladder component
E. β3-Agonists
- Examples: mirabegron, vibegron
- Stimulate β3 receptors → smooth muscle relaxation in bladder wall
- Alternative to antimuscarinics for storage symptoms
Combination Therapy
- Alpha blocker + 5-ARI = best documented combination (superior to either alone)
- Alpha blocker + PDE5i = efficacious
- Tamsulosin + dutasteride + antimuscarinic/β3-agonist for refractory OAB symptoms
- Saw palmetto: not recommended - randomized trials show no benefit at 12 months
Step 3: Surgical Intervention
Indications for surgery:
- Acute urinary retention
- Recurrent UTI
- Recurrent hematuria refractory to 5-ARI
- Bladder calculi
- Azotemia / renal insufficiency
- Failure or inadequacy of medical therapy
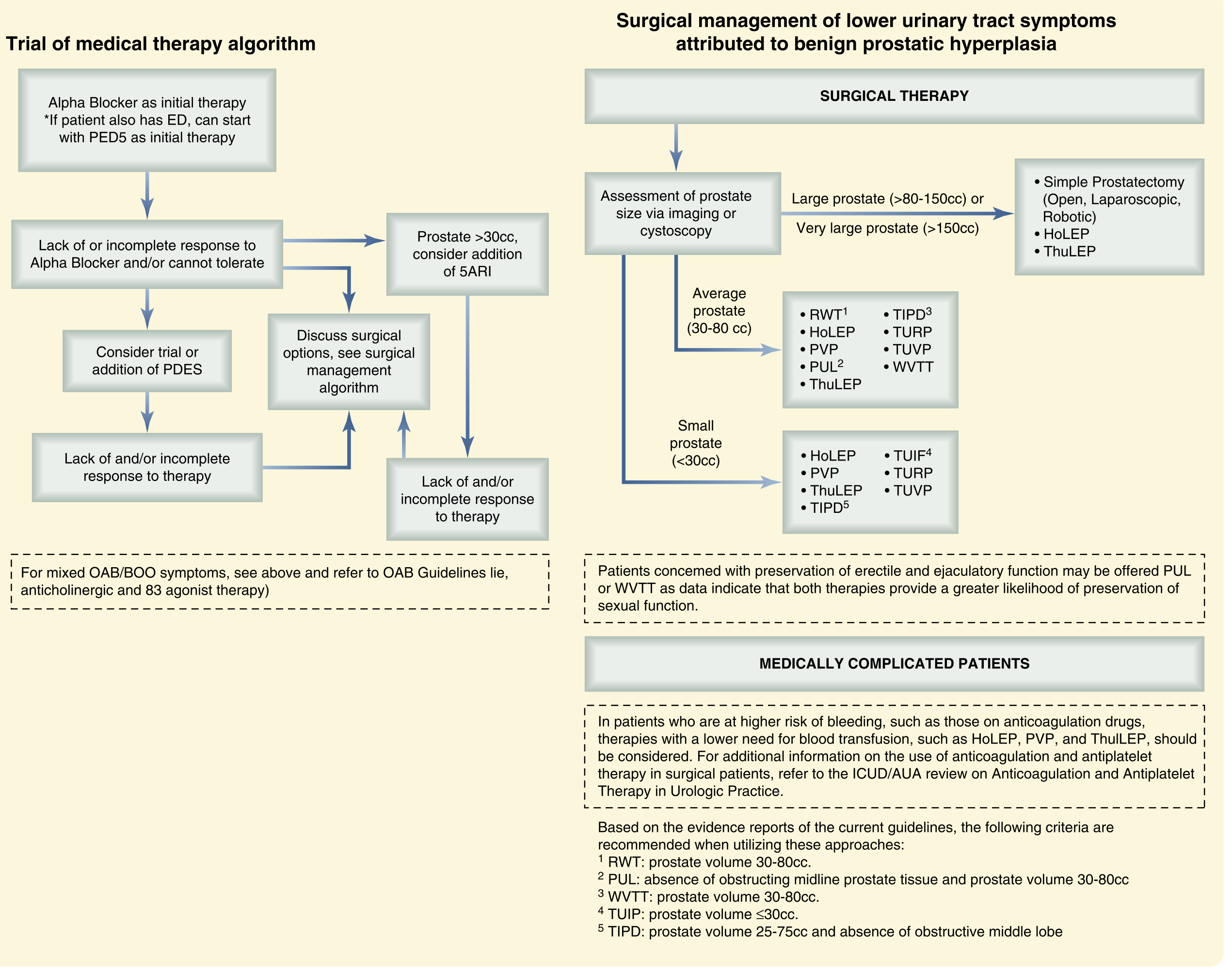
Figure: AUA 2023 BPH management algorithm - medical therapy trial (left) and surgical management stratified by prostate size (right). (Sabiston, adapted from AUA 2023)
Surgical Options by Prostate Size
| Prostate Size | Options |
|---|---|
| Small (<30 mL) | HoLEP, ThuLEP, PVP, TURP, TUVP, TIPD |
| Average (30-80 mL) | TURP, HoLEP, ThuLEP, PVP, PUL, RWT, TIPD, TUVP, WVTT |
| Large (>80-150 mL) or Very Large (>150 mL) | Simple prostatectomy (open/laparoscopic/robotic), HoLEP, ThuLEP |
Key Surgical Procedures
TURP (Transurethral Resection of the Prostate) - the "gold standard"
- Electrosurgical resection of transition zone tissue
- Bipolar TURP (with saline irrigation) has replaced monopolar in many centers - eliminates dilutional hyponatremia from glycine absorption (TURP syndrome)
- Complications: persistent bleeding, UTI, urinary incontinence, urethral stricture, retrograde ejaculation
Laser procedures:
- HoLEP (Holmium Laser Enucleation) - effective for all prostate sizes; lower bleeding risk, preserves ejaculatory function better
- ThuLEP (Thulium Laser Enucleation) - similar outcomes to HoLEP
- PVP (Photoselective Vaporization of the Prostate, "GreenLight") - vaporization rather than resection
Minimally Invasive Procedures (office-based):
-
PUL (Prostatic Urethral Lift, Urolift): mechanical implants open prostatic parenchyma - limited to prostate <80 g with no significant middle lobe; preserves ejaculatory/erectile function
-
WVTT (Water Vapor Thermal Therapy, Rezum): radiofrequency-induced water vapor causes coagulation necrosis; prostate 30-80 mL; also ejaculation-preserving
-
RWT (Rezum Water Therapy): prostate 30-80 mL
-
TUIF/TUIP (Transurethral Incision of Prostate): for small prostates ≤30 mL
-
Prostatic artery embolization (PAE): efficacy and safety data limited; option in selected patients
-
Sabiston Textbook of Surgery; Goldman-Cecil Medicine (AUA 2023 guidelines)
9. PSA in BPH
- PSA levels correlate with prostate volume even without cancer
- PSA and prostate volume generally predict worsening of symptoms over time
- 5α-reductase inhibitors reduce PSA by ~50%; when interpreting PSA, double the measured value in patients on these medications
- Hematuria in BPH requires cystoscopy to rule out bladder cancer
10. BPH in Special Situations
Renal transplant patients:
-
Estimated 3-year incidence of BPH post-transplant: ~9.7%
-
Associated with increased UTI risk and graft loss
-
Prophylactic alpha-blocker and constipation management before Foley removal recommended
-
TURP is safe ≥3 weeks post-transplant; avoid in first 2 weeks and in the presence of a ureteral stent (associated with sepsis and death)
-
Campbell-Walsh-Wein Urology
Summary Table
| Feature | Details |
|---|---|
| Location of origin | Transition zone (periurethral) |
| Key hormone | DHT (via 5α-reductase type 2 from testosterone) |
| Histology | Nodules with glands + stroma; two-cell layer glands with basal cells; corpora amylacea |
| Gross | 60-100 g; slit-like urethra |
| Symptoms | Obstructive + storage + post-void |
| Diagnosis | IPSS, DRE, PSA, urinalysis, PVR, uroflowmetry |
| 1st-line medical | α1-blockers (tamsulosin) ± 5-ARI (dutasteride) |
| PDE5i role | Tadalafil, especially when ED coexists |
| Gold standard surgery | TURP (bipolar preferred) |
| Best for large glands | HoLEP, ThuLEP, simple prostatectomy |
| Ejaculation-preserving | PUL, WVTT |
| Key complication | Acute urinary retention, hydronephrosis |
Sources: Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease; Goldman-Cecil Medicine; Sabiston Textbook of Surgery; Campbell-Walsh-Wein Urology
This is a shared conversation. Sign in to Orris to start your own chat.