In detail about antibiotics
Reading File
Finding Sources
Finding Sources
Searching the Web
antibiotics classification mechanism of action overview 2024
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content. Let me compose the detailed response.
Antibiotics: A Detailed Overview
Antibiotics are chemical agents that kill bacteria (bactericidal) or inhibit their growth (bacteriostatic). They were transformed into clinical medicine after Alexander Fleming's discovery of penicillin in 1928. Today they are grouped by their mechanism of action, spectrum, chemical structure, and pharmacokinetics.
1. Classification by Mechanism of Action
There are five major targets:
| Target | Drug Classes |
|---|---|
| Cell wall synthesis | Beta-lactams, Glycopeptides |
| Cell membrane integrity | Polymyxins, Daptomycin |
| Protein synthesis (30S ribosome) | Aminoglycosides, Tetracyclines |
| Protein synthesis (50S ribosome) | Macrolides, Clindamycin, Linezolid, Chloramphenicol |
| DNA/RNA synthesis | Fluoroquinolones, Rifampin, Metronidazole, Nitrofurantoin |
| Folic acid synthesis | Sulfonamides, Trimethoprim |
2. Beta-Lactam Antibiotics (Cell Wall Inhibitors)
Beta-lactams are the largest and most widely used antibiotic class. They all share a four-membered beta-lactam ring that is essential for activity.
Penicillin core structure (from Katzung's Pharmacology):
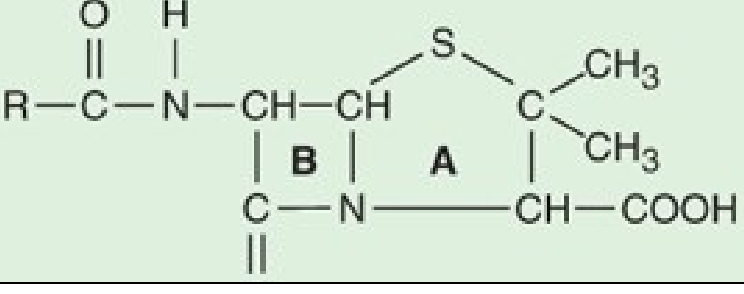
Ring A = thiazolidine ring; Ring B = beta-lactam ring. Hydrolysis of ring B by bacterial beta-lactamases yields penicilloic acid, which is inactive.
Mechanism of Action
Beta-lactams inhibit penicillin-binding proteins (PBPs), which are transpeptidase enzymes responsible for cross-linking peptidoglycan in the bacterial cell wall. Without cross-linking, the wall weakens, water rushes in, and the cell lyses. Importantly, beta-lactams are only active against growing bacteria - they require active cell wall synthesis to exert their bactericidal effect. - Katzung's Basic and Clinical Pharmacology, 16th Edition
Sub-classes of Beta-Lactams
A. Penicillins
- Natural penicillins (Penicillin G, Penicillin V): Narrow spectrum; active against Gram-positive cocci (Streptococcus, non-MRSA Staphylococcus), Neisseria, some spirochetes.
- Penicillinase-resistant (Nafcillin, Oxacillin, Methicillin): Designed to resist beta-lactamase; used specifically for MSSA.
- Aminopenicillins (Ampicillin, Amoxicillin): Extended spectrum including some Gram-negatives (E. coli, H. influenzae, Salmonella), Listeria, enterococci. Amoxicillin is better absorbed orally.
- Antipseudomonal (Piperacillin/tazobactam): Broad Gram-negative coverage including Pseudomonas.
Adverse effects of penicillins: Hypersensitivity reactions are the most serious concern. About 5-8% of people report a penicillin allergy, though only a small fraction have true type I hypersensitivity. Anaphylaxis can occur. Penicillin skin testing helps evaluate genuine IgE-mediated allergy. - Katzung's, Ch. 43
B. Cephalosporins
Organized into generations based on spectrum:
| Generation | Examples | Coverage |
|---|---|---|
| 1st | Cefazolin, Cephalexin | Gram-positives, basic Gram-negatives (E. coli, Klebsiella, Proteus) |
| 2nd | Cefuroxime, Cefaclor, Cefoxitin | Broader Gram-negative; cefoxitin covers anaerobes |
| 3rd | Ceftriaxone, Cefotaxime, Ceftazidime | Extended Gram-negative (including CNS penetration); ceftazidime covers Pseudomonas |
| 4th | Cefepime | Broad - both Gram+ and Gram-, Pseudomonas |
| 5th | Ceftaroline | MRSA activity |
C. Carbapenems
(Imipenem-cilastatin, Meropenem, Ertapenem) - Broadest spectrum beta-lactams. Their distinct stereochemical configuration in the lactam ring makes them resistant to most beta-lactamases. Active against Gram-positives, Gram-negatives (including Pseudomonas - except ertapenem), anaerobes, ESBL-producers. Drugs of last resort for severe hospital-acquired infections.
D. Monobactams
(Aztreonam) - Active only against aerobic Gram-negative rods, including Pseudomonas. No activity against Gram-positives or anaerobes. Can be used in penicillin-allergic patients (no cross-reactivity).
E. Beta-Lactamase Inhibitors
(Clavulanate, Sulbactam, Tazobactam) - These are not antibiotics alone but irreversibly bind and inactivate beta-lactamases. Used in combination: amoxicillin-clavulanate (Augmentin), piperacillin-tazobactam (Tazocin), ampicillin-sulbactam.
3. Glycopeptides (Cell Wall - Gram Positives Only)
Vancomycin binds to the D-Ala-D-Ala terminus of peptidoglycan precursors, blocking transglycosylation and transpeptidation. Unlike beta-lactams which target the enzyme, vancomycin targets the substrate. It is active only against Gram-positive bacteria (it cannot penetrate the outer membrane of Gram-negatives).
Key uses: MRSA bacteremia, endocarditis, C. difficile colitis (oral), MRSA/penicillin-resistant pneumococcal meningitis (combined with ceftriaxone/rifampin). For serious infections, target trough levels of 15-20 mcg/mL or AUC/MIC ratio 400-600 mcg·h/mL.
Adverse effects: Nephrotoxicity, ototoxicity (especially with aminoglycosides), "Red Man Syndrome" (infusion-related histamine release - prevented by slow infusion over 1-2 hours). - Katzung's, Ch. 43
Teicoplanin is a related glycopeptide with a longer half-life, allowing once-daily dosing.
4. Aminoglycosides (30S Protein Synthesis Inhibitors)
(Gentamicin, Amikacin, Tobramycin, Streptomycin, Neomycin)
Mechanism: Bind irreversibly to the 30S ribosomal subunit, causing misreading of mRNA codons, production of faulty proteins, and ultimately bactericidal cell death. They require an active proton gradient to enter cells, so they are inactive against anaerobes (no electron transport chain).
Spectrum: Aerobic Gram-negative bacilli, including Pseudomonas. Gentamicin covers Enterobacteriaceae broadly. Streptomycin is used in tuberculosis.
PK/PD: Concentration-dependent killing - the higher the peak concentration, the greater the kill. Once-daily dosing (high peak) takes advantage of this and minimizes nephrotoxicity.
Adverse effects:
- Nephrotoxicity (proximal tubular injury) - usually reversible; monitor creatinine
- Ototoxicity (cochlear > vestibular) - may be permanent; avoid prolonged use
- Neuromuscular blockade (especially in myasthenia gravis patients)
- Avoid in pregnancy (fetal eighth nerve damage)
5. Macrolides and Related Agents (50S Protein Synthesis)
(Azithromycin, Clarithromycin, Erythromycin; and related: Clindamycin, Linezolid, Chloramphenicol)
Mechanism: Bind to the 23S rRNA of the 50S ribosomal subunit, blocking translocation and elongation of the peptide chain. Macrolides are generally bacteriostatic (bactericidal at high concentrations for some organisms).
Spectrum: Gram-positives, atypicals (Mycoplasma, Chlamydia, Legionella), H. influenzae. Azithromycin (Z-pack) achieves high tissue concentrations due to extensive distribution.
Clindamycin: Binds the same 50S site but is used predominantly for Gram-positive anaerobic infections (B. fragilis, oral anaerobes), MRSA skin infections. Classic cause of C. difficile colitis.
Linezolid: Oxazolidinone class; binds 50S to block initiation complex. Active against MRSA, VRE, drug-resistant tuberculosis. Adverse: serotonin syndrome (MAOI-like), myelosuppression with prolonged use.
6. Tetracyclines (30S Protein Synthesis)
(Tetracycline, Doxycycline, Minocycline, Tigecycline)
Mechanism: Bind reversibly to the 30S subunit, blocking aminoacyl-tRNA attachment to the ribosome. Bacteriostatic.
Spectrum: Broad - Gram-positives, Gram-negatives, atypicals (Chlamydia, Mycoplasma, Rickettsia), spirochetes (Lyme disease, syphilis), Brucella.
Adverse effects: GI upset, photosensitivity, hepatotoxicity (high dose), teeth/bone deposition (avoid in children < 8 years and pregnancy), esophageal irritation.
Doxycycline is the most commonly used - once-daily dosing, broader tissue penetration, used for CAP, STIs, Lyme disease, malaria prophylaxis.
7. Fluoroquinolones (DNA Gyrase Inhibitors)
(Ciprofloxacin, Levofloxacin, Moxifloxacin, Norfloxacin)
Mechanism: Inhibit DNA gyrase (topoisomerase II) and topoisomerase IV, which are essential for DNA replication, transcription, and repair. Inhibition causes double-stranded DNA breaks. Bactericidal.
| Drug | Coverage |
|---|---|
| Ciprofloxacin | Gram-negatives, Pseudomonas; minimal Gram-positive/anaerobic |
| Levofloxacin | MSSA, Streptococcus, Gram-negatives, atypicals ("respiratory quinolone") |
| Moxifloxacin | Streptococcus, anaerobes, atypicals; NOT Pseudomonas |
Adverse effects: QTc prolongation (avoid with other QT-prolonging drugs), tendinopathy and tendon rupture (especially Achilles; risk with corticosteroids), arthropathy (avoid in children/pregnancy), Stevens-Johnson syndrome, CNS effects (seizures, confusion). - Lee's Essential Otolaryngology
8. Sulfonamides and Trimethoprim (Folate Synthesis)
Mechanism: Bacteria must synthesize their own folate (humans absorb it from diet). Sulfonamides are structural analogs of PABA and competitively inhibit dihydropteroate synthase. Trimethoprim inhibits dihydrofolate reductase (a later step). The combination TMP-SMX (Co-trimoxazole) provides sequential blockade of the folate pathway, which is synergistically bactericidal.
Uses: UTIs (E. coli), Pneumocystis jirovecii pneumonia (PCP) prophylaxis/treatment, Toxoplasma (with pyrimethamine), MRSA skin infections (TMP-SMX).
Adverse effects: Sulfonamides - hypersensitivity (Stevens-Johnson), hemolytic anemia (G6PD), kernicterus (neonates), crystalluria. TMP - hyperkalemia (blocks renal K+ secretion), megaloblastic anemia.
9. Metronidazole and Nitrofurantoin (DNA Damage)
Metronidazole (Bactericidal) - reduced to a reactive intermediate by anaerobic organisms, which then binds DNA and causes strand breakage. Active against strict anaerobes (Bacteroides, Clostridium) and certain protozoa (Trichomonas, Giardia, Entamoeba). Penetrates blood-brain barrier well. Adverse: metallic taste, disulfiram-like reaction with alcohol, peripheral neuropathy with prolonged use.
Nitrofurantoin - active metabolites damage bacterial DNA; concentrated in urine. Used only for uncomplicated UTIs. Adverse: pulmonary fibrosis (chronic use), hemolytic anemia (G6PD deficiency), peripheral neuropathy.
10. Rifamycins
Rifampicin (Rifampin) - inhibits bacterial DNA-dependent RNA polymerase, blocking transcription. Bactericidal. Key uses: tuberculosis (always in combination to prevent resistance), MRSA (in combination, never alone), Neisseria meningitidis prophylaxis, leprosy. Major adverse effect: orange discoloration of body fluids, hepatotoxicity, potent CYP450 inducer (major drug interactions).
11. Polymyxins
(Polymyxin B, Colistin/Polymyxin E) - Act on the cell membrane like detergents, disrupting the lipopolysaccharide layer of Gram-negative outer membranes and causing leakage. Reserved for pan-resistant Gram-negative infections (Acinetobacter, Pseudomonas, Klebsiella carbapenemase-producers). Significant nephrotoxicity and neurotoxicity.
12. Bactericidal vs. Bacteriostatic
| Property | Bactericidal | Bacteriostatic |
|---|---|---|
| Definition | Kills bacteria (99.9% reduction) | Inhibits growth; depends on host immunity to clear |
| Examples | Beta-lactams, Aminoglycosides, Fluoroquinolones, Metronidazole, Vancomycin | Tetracyclines, Macrolides (usually), Sulfonamides, Chloramphenicol |
| Clinical importance | Preferred in immunocompromised patients, endocarditis, meningitis | Often adequate for mild-moderate infections with intact immunity |
13. Spectrum of Activity
- Narrow spectrum: Penicillin G (primarily Gram+), Aztreonam (only aerobic Gram-)
- Broad spectrum: Carbapenems, TMP-SMX, Tetracyclines, Fluoroquinolones
- Gram-positive specific: Vancomycin, Linezolid, Daptomycin
- Gram-negative specific: Aztreonam, Polymyxins
- Anaerobic coverage: Metronidazole, Clindamycin, Carbapenems, Moxifloxacin
14. Antibiotic Resistance
From Harrison's Principles of Internal Medicine (22nd Ed., 2025) and Medical Microbiology 9e, resistance mechanisms fall into three main categories:
A. Alteration/Bypass of Drug Target
- Beta-lactam resistance - mutation of PBPs (e.g., MRSA has PBP2a, encoded by mecA gene, with very low affinity for beta-lactams)
- Fluoroquinolone resistance - mutations in DNA gyrase and topoisomerase IV genes
- Rifampin resistance - mutation in RNA polymerase gene
- Vancomycin resistance (VRE) - D-Ala-D-Ala terminus modified to D-Ala-D-Lac, reducing vancomycin binding >1000-fold
B. Reduced Drug Access (Decreased Uptake / Efflux)
- Efflux pumps - bacteria actively pump antibiotics out of the cell. Pseudomonas uses MexAB-OprM efflux system conferring broad resistance. E. coli efflux pumps (e.g., emrE) confer multi-drug resistance.
- Porin loss - Gram-negative bacteria reduce outer membrane porins, limiting antibiotic entry.
- Biofilm formation - extracellular polymeric substances reduce antibiotic penetration by up to 9x the bacterial mass. Bacteria in biofilms enter slow growth states, reducing susceptibility to cell wall-active agents.
C. Drug Modification/Destruction
- Beta-lactamases - enzymes that open the beta-lactam ring, destroying activity. Extended-spectrum beta-lactamases (ESBLs) inactivate most cephalosporins. Carbapenemases (KPC, NDM, OXA-48) inactivate carbapenems.
- Aminoglycoside-modifying enzymes - acetyltransferases, phosphotransferases, nucleotidyltransferases.
- Chloramphenicol acetyltransferase - acetylates chloramphenicol.
Mechanisms of Resistance Transfer
Resistance genes spread through:
- Plasmid-mediated horizontal gene transfer (most common route between species)
- Chromosomal mutations during DNA replication
- Transposons ("jumping genes") that carry resistance cassettes
- Integrons - gene capture elements found in many MDR organisms
15. Antibiotic Pharmacokinetics/Pharmacodynamics (PK/PD)
Understanding how antibiotics kill relative to time and concentration guides optimal dosing:
| PK/PD Parameter | Drug Class | Implication |
|---|---|---|
| Time-dependent killing (T > MIC) | Beta-lactams | Prolonged infusions or frequent dosing; kill plateaus above 4x MIC |
| Concentration-dependent killing (Cmax/MIC) | Aminoglycosides, Fluoroquinolones | High peak doses (once-daily aminoglycosides) |
| AUC-dependent (AUC/MIC) | Vancomycin, Azithromycin | Total drug exposure drives efficacy |
16. Principles of Clinical Use
- Empiric therapy - Initial broad-spectrum coverage based on likely pathogens; narrow once culture/susceptibility results are available ("de-escalation").
- Targeted therapy - Chosen based on organism identity and MIC data.
- Prophylactic use - Surgical site infection prevention (single preoperative dose of cefazolin), endocarditis prophylaxis, meningitis contacts (rifampin/ciprofloxacin), malaria (doxycycline).
- Combination therapy - Rationale: broaden empiric coverage, prevent resistance (TB, HIV co-infection), synergy (e.g., ampicillin + gentamicin for Enterococcal endocarditis).
- Antibiotic stewardship - Appropriate selection, dose, duration, and route to minimize resistance, C. difficile, side effects, and cost.
Summary Quick-Reference Table
| Class | Example | Target | Bactericidal? | Key Uses | Key Toxicity |
|---|---|---|---|---|---|
| Penicillins | Amoxicillin, Pip-Tazo | Cell wall PBPs | Yes | Strep, dental, UTI, broad Gram- | Allergy, anaphylaxis |
| Cephalosporins | Ceftriaxone, Cefazolin | Cell wall PBPs | Yes | CAP, UTI, surgical prophylaxis | Allergy, diarrhea |
| Carbapenems | Meropenem | Cell wall PBPs | Yes | MDR Gram-, severe infections | Seizures (imipenem) |
| Glycopeptides | Vancomycin | Cell wall substrate | Yes | MRSA, C. diff (oral) | Nephrotox, Red Man |
| Aminoglycosides | Gentamicin | 30S ribosome | Yes | Gram-negatives, Pseudomonas | Nephrotox, ototox |
| Macrolides | Azithromycin | 50S ribosome | Static | Atypicals, CAP, STI | QTc, GI, drug interactions |
| Tetracyclines | Doxycycline | 30S ribosome | Static | Lyme, atypicals, malaria | Photosensitivity, teeth |
| Fluoroquinolones | Ciprofloxacin | DNA gyrase | Yes | UTI, respiratory, Pseudomonas | Tendinopathy, QTc |
| Sulfonamides | TMP-SMX | Folate pathway | Yes | UTI, PCP, MRSA skin | Stevens-Johnson, hemolysis |
| Metronidazole | Metronidazole | DNA | Yes | Anaerobes, C. diff, protozoa | Metallic taste, disulfiram |
| Rifamycins | Rifampin | RNA polymerase | Yes | TB, MRSA adjunct | CYP inducer, orange secretions |
| Polymyxins | Colistin | Cell membrane | Yes | Pan-resistant Gram- | Nephrotox, neurotox |
Sources:
- Katzung's Basic and Clinical Pharmacology, 16th Ed., Ch. 43 - Beta-Lactam & Other Cell Wall Antibiotics
- Harrison's Principles of Internal Medicine 22E (2025), Ch. 149-150 - Antimicrobial Therapy and Bacterial Resistance
- Medical Microbiology 9e - Antibiotic Resistance Mechanisms
- Lee's Essential Otolaryngology - Antibiotic Classification Table
This is a shared conversation. Sign in to Orris to start your own chat.