Steps of thyriodectomy with pics and some original pics
Reading File
Finding Sources
Searching the Web
thyroidectomy surgical steps procedure photos
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have rich textbook content and images. Let me compile the full comprehensive answer.
Thyroidectomy - Surgical Steps with Illustrations
Source: Sabiston Textbook of Surgery (20th ed.) and Scott-Brown's Otorhinolaryngology
Indications
- Thyroid cancer
- Symptomatic goitre (compressive symptoms: dysphagia, dyspnea, hoarseness)
- Hyperthyroidism unresponsive to medical management (Graves disease, toxic multinodular goitre)
- Suspicious or indeterminate thyroid nodules
Types of Resection
| Type | Tissue Removed |
|---|---|
| Total thyroidectomy | All visible thyroid tissue |
| Near-total thyroidectomy | <1 g remnant left at Berry's ligament |
| Thyroid lobectomy (hemithyroidectomy) | One lobe + isthmus ± pyramidal lobe |
| Subtotal thyroidectomy | 3-5 g remnant left bilaterally |
| Isthmusectomy | Isthmus + pyramidal lobe only |
Preoperative Preparation
- Biochemical assessment - thyroid function tests, serum calcium (to screen for concurrent hyperparathyroidism)
- Neck ultrasound + FNA biopsy of suspicious nodules
- For hyperthyroidism - render patient euthyroid with propylthiouracil or methimazole; Lugol's iodine within 10 days of surgery reduces gland vascularity
- Voice assessment - preoperative laryngoscopy or transcutaneous laryngeal ultrasound to document baseline vocal cord function
- Airway assessment - CT neck for deviation/tracheal compression, especially with large goitres
Surgical Steps
Step 1 - Anesthesia and Positioning
- General endotracheal anesthesia; if intraoperative nerve monitoring (IONM) is planned, a specialized neuromonitoring ETT with vocal cord contact electrodes is used
- Patient supine, both arms tucked at sides
- Back raised 20 degrees (shoulder roll), neck extended to expose the anterior neck
- A "beach chair" position with a roll under the shoulders provides optimal exposure
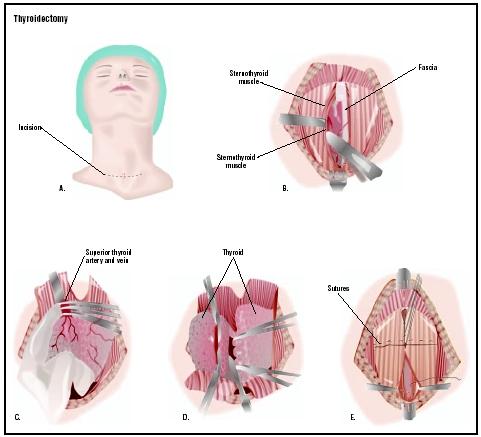
Step 2 - Skin Incision (Kocher's Incision)

- A collar (transverse) incision is made approximately 2 cm above the sternal notch, placed in a natural skin crease for cosmesis
- Length typically 4-6 cm; extended for large goitres
- Incision deepened through skin, subcutaneous fat, and the platysma muscle
Step 3 - Raising Subplatysmal Flaps
- Superior flap raised to the level of the thyroid notch
- Inferior flap raised to the sternal notch
- Dissection proceeds in the avascular plane deep to the platysma
Step 4 - Division of Strap Muscles and Exposure of the Thyroid

- The midline raphe between the sternohyoid muscles is divided vertically along the linea alba
- Strap muscles (sternohyoid and sternothyroid) are retracted laterally to expose the thyroid gland
- The isthmus can be divided at this stage to allow separate lobe mobilization and to work through a smaller incision
- The inferior thyroid vein is identified and ligated
Step 5 - Mobilization of the Superior Pole
- The superior pole of the thyroid is retracted inferiorly and medially
- The avascular space between the cricothyroid muscle and the superior pole is developed by blunt dissection
- The superior thyroid artery and vein are individually ligated and divided close to the thyroid capsule - this protects the external branch of the superior laryngeal nerve (EBSLN)
- The EBSLN runs within 1 cm of the superior thyroid vessels in most patients and injury causes loss of the upper pitch register ("opera singer's nerve")
Step 6 - Ligation of the Middle Thyroid Vein
- The middle thyroid vein drains the middle third of each lobe
- It is ligated and divided to allow medial rotation of the thyroid lobe for posterior dissection
Step 7 - Identification and Preservation of the Recurrent Laryngeal Nerve (RLN)

- The RLN is the most critical structure to identify and protect during thyroidectomy
- On the right side - the RLN loops around the subclavian artery and approaches the tracheoesophageal groove obliquely from lateral to medial
- On the left side - the RLN loops around the aortic arch and ascends more medially in the tracheoesophageal groove
- The RLN is identified either where it crosses the inferior thyroid artery or at its entry into the larynx at the cricothyroid joint
- IONM (intraoperative neuromonitoring) via vagal stimulation provides real-time electromyographic confirmation of nerve integrity
- The nerve is traced and kept under direct vision throughout dissection
Step 8 - Preservation of the Parathyroid Glands
- There are typically 4 parathyroid glands (superior and inferior pairs), each the size of a lentil (~50 mg)
- The superior parathyroids lie posterior to the upper thyroid lobe near where the RLN enters the larynx
- The inferior parathyroids are more variable in position - often near the inferior thyroid pole or within the thyrothymic ligament
- Each gland is identified and carefully preserved with its blood supply (branches of the inferior thyroid artery)
- If a gland is inadvertently removed or devascularized, it is minced and auto-transplanted into the sternocleidomastoid or brachioradialis muscle
Step 9 - Ligation of the Inferior Thyroid Artery
- The inferior thyroid artery is a branch of the thyrocervical trunk from the subclavian artery
- It is ligated at the level of the tracheoesophageal groove, distal to the parathyroid branches, to preserve parathyroid blood supply
Step 10 - Division of Berry's Ligament

- Berry's (suspensory) ligament is the posterolateral attachment of the thyroid to the tracheal rings
- It is the final attachment of the thyroid lobe to the trachea
- The RLN often passes within or immediately adjacent to Berry's ligament - this is the highest-risk point for nerve injury during dissection
- The ligament is carefully divided with fine scissors or energy device to release the lobe
- The freed lobe is now removed
Step 11 - Hemostasis and Wound Closure
- Meticulous hemostasis is achieved with bipolar diathermy or energy-based devices (e.g., LigaSure, Harmonic)
- The wound is irrigated and inspected
- A drain (closed suction) may be placed if there is concern for ooze or in cases with large dead space - though routine drainage is not universally required
- The strap muscles are re-approximated with absorbable sutures in the midline
- The platysma is closed as a separate layer
- Skin is closed with subcuticular sutures or surgical glue for a cosmetically acceptable scar
Key Structures at Risk
| Structure | Risk | Consequence if Injured |
|---|---|---|
| Recurrent laryngeal nerve | Highest | Hoarseness (unilateral), aphonia/stridor (bilateral) |
| External branch of superior laryngeal nerve | Moderate | Loss of high-pitch voice, voice fatigue |
| Parathyroid glands | Moderate | Hypocalcemia (temporary or permanent) |
| Inferior thyroid artery | Moderate | Parathyroid devascularization |
| Trachea | Low | Tracheal injury, tracheomalacia in long-standing goitre |
Postoperative Care
- Monitor calcium (PTH within 1 hour of resection is most predictive of hypoparathyroidism)
- Calcium and vitamin D supplementation as needed
- Voice assessment before discharge
- Wound check at 1-2 weeks
- Thyroid hormone replacement after total thyroidectomy (levothyroxine)
- RAI ablation if indicated for differentiated thyroid cancer
Sources: Sabiston Textbook of Surgery, 21st ed. (Elsevier); Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th ed.
This is a shared conversation. Sign in to Orris to start your own chat.