Hepatorenal syndrome management
Reading File
Finding Sources
Searching PubMed
"hepatorenal syndrome"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information. Let me compile the full management guide.
Hepatorenal Syndrome (HRS) — Management
Pathophysiology
HRS is a form of functional renal failure without renal pathology that complicates advanced cirrhosis, acute liver failure, or severe alcoholic hepatitis. The kidneys are histologically normal. The core mechanism is illustrated below:
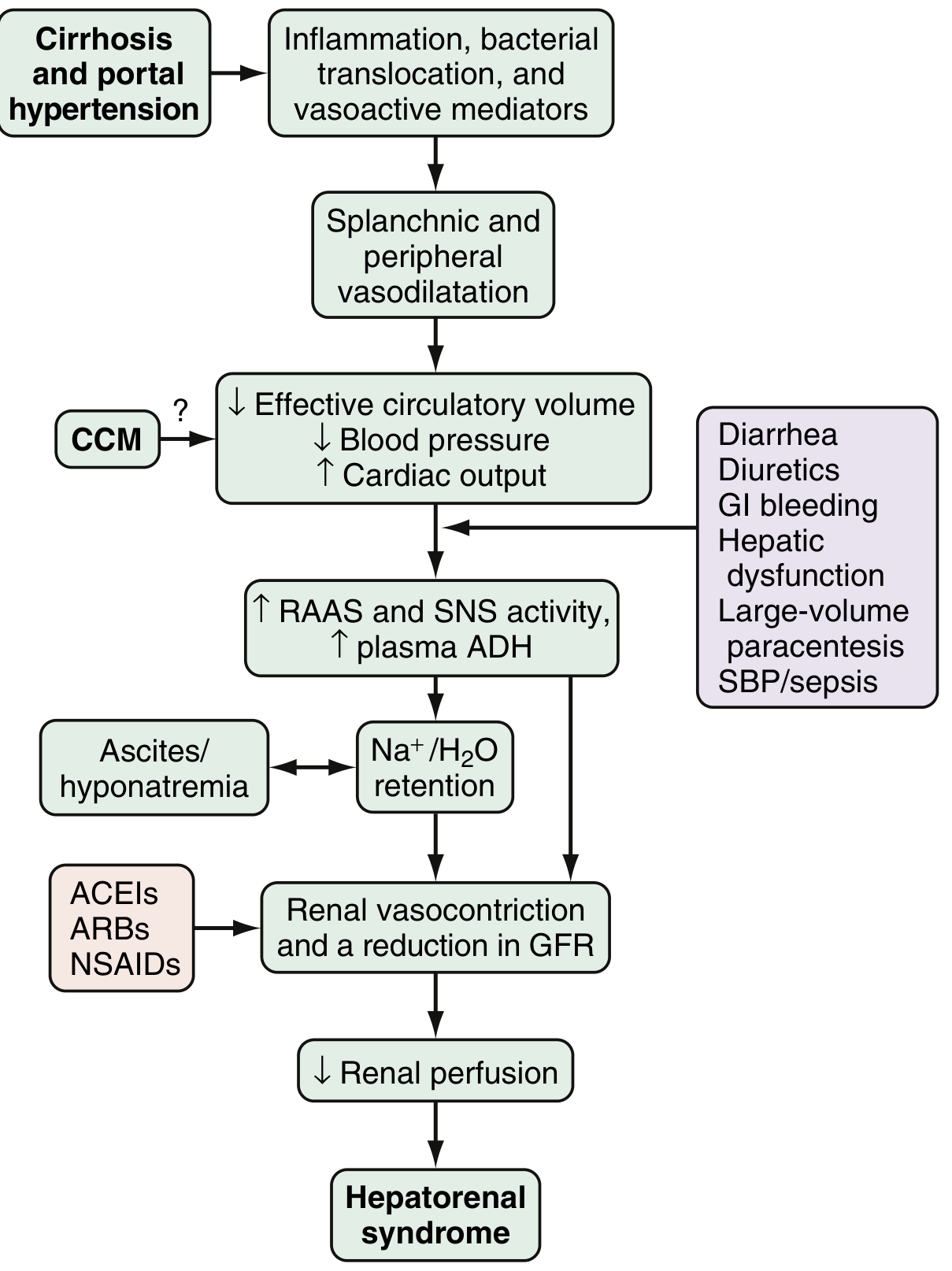
Three components drive it:
- Splanchnic arterial vasodilation (mediated by NO, CO, glucagon, prostacyclin, adrenomedullin) — the primary driver
- Compensatory renal vasoconstriction via RAAS, SNS, and ADH activation
- Cardiac dysfunction (cirrhotic cardiomyopathy further reduces effective output)
Classification (Updated Terminology)
| Old Term | New ICA Term | Characteristics |
|---|---|---|
| Type 1 HRS | HRS-AKI | Rapid, progressive AKI (≥0.3 mg/dL rise in creatinine in 48 h, or ≥50% from baseline); worse prognosis |
| Type 2 HRS | HRS-CKD | Stable, slowly progressive; GFR reduced but creatinine relatively stable; often seen with refractory ascites |
Diagnostic Criteria (ICA 2015 Revised)
All of the following must be present (Box 94.2, Sleisenger & Fordtran's):
- Cirrhosis with ascites
- AKI by ICA criteria (creatinine rise ≥0.3 mg/dL in 48 h OR ≥50% from baseline)
- No response after ≥48 hours of diuretic withdrawal + IV albumin 1 g/kg/day (max 100 g/day)
- Absence of shock
- No current/recent nephrotoxic drugs
- No parenchymal renal disease (proteinuria <500 mg/day, no microhematuria >50 RBC/hpf, normal renal ultrasound)
Key point: Urine output criteria are NOT used in cirrhotic patients because they are frequently oliguric at baseline due to sodium retention.
Management
Step 1 — Identify and Remove Precipitants
Before diagnosing HRS, actively exclude and treat:
- SBP/sepsis (present in ~30% preceding HRS; treat with antibiotics ± albumin)
- Volume depletion — overdiuresis, GI hemorrhage, diarrhea (lactulose overdose)
- Nephrotoxins — NSAIDs, aminoglycosides, contrast agents
- Vasodilators — ACEIs, ARBs
Diuretics must be stopped immediately on suspicion of HRS.
Step 2 — Volume Expansion with Albumin
- IV albumin 1 g/kg/day (max 100 g/day) for 48 hours
- Serves both as a volume expander and to bind circulating vasoactive mediators
- Lack of response after 48 h is required to confirm HRS diagnosis
Step 3 — Vasoconstrictors (First-Line Treatment)
The goal is to counteract splanchnic vasodilation and improve effective circulating volume, thereby relieving renal vasoconstriction. All regimens are combined with IV albumin.
🥇 Terlipressin + Albumin (First-Line, where available)
- Selective vasopressin V1 receptor agonist; IV bolus or continuous infusion
- Continuous infusion is better tolerated and effective at lower doses than bolus dosing
- Two pivotal RCTs (OT-0401 and REVERSE trials): terlipressin + albumin reversed HRS in 27% vs. 14% with albumin alone (P = 0.004)
- Creatinine improvement: 30–43% vs. 8–13% with albumin alone
- Response is better with lower baseline creatinine and lower bilirubin — supports early initiation
- Dosing (Box 94.3): bolus 0.5–2 mg IV q4–6h; or infusion 2–12 mg/day
- Adverse effects: cardiovascular complications (ischemia, arrhythmia) — close monitoring required; respiratory failure in ACLF patients
🥈 Norepinephrine + Albumin (Alternative, ICU setting)
- IV α1-agonist; requires ICU monitoring
- Two small RCTs: equal efficacy and safety to terlipressin
- Response rates 40–75%; relapse ~20%
- Significant cardiovascular side effects reported
- Preferred in ICU when terlipressin is unavailable
🥉 Midodrine + Octreotide + Albumin (Third-Line, USA)
- Midodrine: oral α1-agonist (titrated to ↑MAP); Octreotide: somatostatin analog (inhibits endogenous vasodilators)
- Easier to administer (oral midodrine); favorable safety profile
- Head-to-head RCT vs. terlipressin: renal recovery 28.6% vs. 70.4% (P = 0.01) — significantly inferior to terlipressin
- Used most commonly in the US where terlipressin availability has been limited, but now classified as third-line
- Dosing: Midodrine 7.5–15 mg PO TID; Octreotide 100–200 mcg SC TID; Albumin 20–40 g/day IV
Step 4 — Renal Replacement Therapy
- Initiated when pharmacologic therapy fails
- Bridge to liver transplantation, not a definitive treatment
- Does not improve underlying pathophysiology
Step 5 — TIPS (Transjugular Intrahepatic Portosystemic Shunt)
- Reduces portal hypertension, improving splanchnic hemodynamics
- Limited data in HRS specifically; more evidence in refractory ascites
- Contraindicated in advanced hepatic encephalopathy, severe hepatic insufficiency (bilirubin >5 mg/dL), MELD >18 in most protocols
Step 6 — Liver Transplantation (Definitive Therapy)
- Best and only curative treatment for HRS
- Recovery of renal function is typical post-transplant in HRS (kidneys are histologically normal)
- Pre-transplant treatment with vasoconstrictors may improve candidacy and bridge to transplant
- For HRS-CKD: simultaneous liver-kidney transplantation (SLKT) may be considered
- In both HRS-AKI and HRS-CKD, prognosis is poor without transplant
Prevention
| Trigger | Preventive Strategy |
|---|---|
| SBP | IV albumin 1.5 g/kg at diagnosis + 1 g/kg on day 3 |
| Large-volume paracentesis (>5 L) | IV albumin 6–8 g per liter removed |
| Primary prophylaxis in cirrhosis | Norfloxacin 400 mg/day (long-term) in advanced cirrhosis with low-protein ascites |
| Variceal bleeding | Antibiotics (ceftriaxone 1 g/day) + octreotide/terlipressin |
Prognosis
- HRS-AKI (Type 1): median survival without treatment is 2–4 weeks; with terlipressin bridge to transplant, outcomes improve substantially
- HRS-CKD (Type 2): median survival ~6 months
- HRS reversal with vasoconstrictors does not significantly improve overall survival unless transplantation is achieved
Recent Evidence
A 2024 systematic review and meta-analysis (PMID: 38285703) comparing terlipressin vs. norepinephrine for HRS-AKI confirmed broadly similar efficacy between the two agents, supporting norepinephrine as a reasonable terlipressin alternative. A 2026 meta-analysis (PMID: 41853888) found that continuous infusion terlipressin is preferred over bolus dosing for both variceal bleeding and HRS due to better tolerability and efficacy at lower doses.
Sources: Harrison's Principles of Internal Medicine 22E, p. HRS chapter; Sleisenger & Fordtran's Gastrointestinal and Liver Disease, Ch. 94; Goldman-Cecil Medicine, Ch. 139.
This is a shared conversation. Sign in to Orris to start your own chat.