Give me proper cardiac cycle note
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have excellent, comprehensive content from Costanzo Physiology and Medical Physiology. Let me compile the full, detailed cardiac cycle note.
The Cardiac Cycle
Sources: Costanzo Physiology 7th Ed., Guyton & Hall Medical Physiology, Medical Physiology (Boron & Boulpaep)
Definition
The cardiac cycle is the sequence of mechanical and electrical events that repeats with every heartbeat, from the beginning of one heartbeat to the beginning of the next. Its duration equals the reciprocal of the heart rate:
Duration (s/beat) = 60 / Heart rate (beats/min)
At a heart rate of 75 beats/min → cycle duration = 0.8 seconds
At 72 beats/min → ~0.833 seconds
Initiation
Each cycle is initiated by spontaneous action potential generation in the sinoatrial (SA) node (superior lateral wall of the right atrium). The impulse travels through both atria, then through the AV bundle into the ventricles. The AV node introduces a delay of >0.1 second, allowing atria to contract before the ventricles - the atria act as "primer pumps."
Wiggers Diagram
The 7 Phases of the Cardiac Cycle
The cycle is divided into 7 phases (A through G), spanning systole and diastole:
DIASTOLE
Phase A - Atrial Systole
| Parameter | Event |
|---|---|
| ECG | P wave (atrial depolarization) → PR interval |
| Valves | Mitral valve open; aortic valve closed |
| Pressures | Left atrial pressure rises; small "blip" rise in LV pressure |
| Volume | Ventricular volume increases (final ~20% of filling) |
| Venous pulse | a wave (atrial contraction reflected back into veins) |
| Heart sound | S4 (not audible in normals; heard in decreased ventricular compliance, e.g. LV hypertrophy) |
- The left ventricle is relaxed and mitral valve is already open - passive filling has been occurring
- Atrial contraction contributes <20% of stroke volume at rest; rises to ~40% during heavy exercise
- Atria act mainly as passive reservoirs, but do boost ventricular filling
Phase B - Isovolumetric Ventricular Contraction (IVC)
| Parameter | Event |
|---|---|
| ECG | QRS complex (ventricular depolarization) |
| Valves | Mitral valve closes → aortic valve still closed → ALL VALVES CLOSED |
| Pressures | LV pressure rises steeply; no change in volume |
| Volume | Constant (isovolumetric) |
| Venous pulse | c wave (bulging of AV valves back toward atria) |
| Heart sound | S1 ("lub") - closure of mitral (then tricuspid) valve |
- As LV contracts, LV pressure exceeds LA pressure → mitral valve snaps shut
- Both valves are now closed; pressure builds rapidly with no ejection
- S1 may be physiologically split because mitral closes slightly before tricuspid
- This is the period of highest rate of pressure rise (dP/dt max)
SYSTOLE
Phase C - Rapid Ventricular Ejection
| Parameter | Event |
|---|---|
| ECG | ST segment |
| Valves | Aortic valve opens (when LV pressure > aortic pressure ~80 mmHg); mitral still closed |
| Pressures | LV pressure peaks (~120 mmHg); aortic pressure rises rapidly |
| Volume | Dramatic decrease - most of stroke volume ejected |
| Heart sound | None |
- Blood is rapidly ejected from LV into aorta down a pressure gradient
- Aortic pressure increases sharply due to blood suddenly added to aorta
- Left atrial filling begins - LA pressure slowly rises as pulmonary veins return blood
Phase D - Reduced Ventricular Ejection
| Parameter | Event |
|---|---|
| ECG | T wave (ventricular repolarization begins) |
| Valves | Aortic valve still open; mitral still closed |
| Pressures | LV pressure falls (ventricle repolarizing); aortic pressure begins to fall (run-off exceeds inflow) |
| Volume | Continues to fall (reaches end-systolic volume, ESV) |
| Heart sound | None |
- Ejection continues but at a slower rate
- Ventricular volume reaches its minimum (ESV ~50 mL)
- At end of ejection: LV contains ~50 mL (ESV); it had ~130 mL at end of diastole (EDV)
- Stroke Volume = EDV - ESV ≈ 80 mL
DIASTOLE (resumes)
Phase E - Isovolumetric Ventricular Relaxation (IVR)
| Parameter | Event |
|---|---|
| ECG | After T wave (ventricular repolarization complete) |
| Valves | Aortic valve closes (LV pressure < aortic pressure) → ALL VALVES CLOSED again |
| Pressures | LV pressure falls dramatically; aortic shows dicrotic notch |
| Volume | Constant (isovolumetric relaxation) |
| Venous pulse | v wave (venous pressure peaks due to filling of atria while AV valves are closed) |
| Heart sound | S2 ("dub") - closure of aortic (then pulmonic) valve |
- Aortic valve closes slightly before pulmonic → S2 physiological splitting during inspiration
- Mechanism of inspiratory splitting: decreased intrathoracic pressure → increased venous return to right heart → increased RV stroke volume → prolonged RV ejection → pulmonic valve closes later
- The dicrotic notch on the aortic pressure trace marks aortic valve closure
Phase F - Rapid Ventricular Filling
| Parameter | Event |
|---|---|
| ECG | Isoelectric (between T and next P wave) |
| Valves | Mitral valve opens (LV pressure falls below LA pressure) |
| Pressures | LV pressure is low and relatively constant; LA pressure falls as it empties |
| Volume | Rapid increase in LV volume |
| Heart sound | S3 - heard in children/young adults (normal); pathological in adults >40 (suggests heart failure, volume overload) |
- Blood rushes passively from LA into LV down a pressure gradient
- This is the period of most rapid ventricular filling (~70-80% of filling occurs here)
Phase G - Reduced Ventricular Filling (Diastasis)
| Parameter | Event |
|---|---|
| ECG | Isoelectric |
| Valves | Mitral valve still open |
| Pressures | LA and LV pressures equalize; both rise slowly |
| Volume | Slowly increases toward plateau |
| Heart sound | None |
- "Diastasis" - a period of quiescence where atrial and ventricular pressures nearly equalize
- Very little blood flows (mitral valve wide open, minimal gradient)
- Cycle then restarts with the next P wave → atrial systole (Phase A)
Summary Table
| Phase | ECG | Valve Event | Volume | Sound |
|---|---|---|---|---|
| A - Atrial Systole | P wave | - | ↑ (final filling) | S4 (abnormal) |
| B - Isovolumetric Contraction | QRS | Mitral closes | Constant | S1 |
| C - Rapid Ejection | ST segment | Aortic opens | ↓↓ | - |
| D - Reduced Ejection | T wave | - | ↓ (reaches ESV) | - |
| E - Isovolumetric Relaxation | Post-T | Aortic closes | Constant | S2 |
| F - Rapid Filling | Isoelectric | Mitral opens | ↑↑ | S3 (abnormal in adults) |
| G - Diastasis | Isoelectric | - | ↑ (slow) | - |
Key Pressures (Left Heart)
| Parameter | Value |
|---|---|
| LV systolic pressure (peak) | ~120 mmHg |
| LV diastolic pressure (lowest) | ~0-8 mmHg |
| Aortic systolic pressure | ~120 mmHg |
| Aortic diastolic pressure | ~80 mmHg |
| Aortic mean pressure | ~100 mmHg |
| LA pressure (mean) | ~5 mmHg |
| End-diastolic volume (EDV) | ~130 mL |
| End-systolic volume (ESV) | ~50 mL |
| Stroke Volume | ~80 mL |
| Ejection Fraction (EF) | ~60% (normal >55%) |
Jugular Venous Pulse (JVP) Waves
| Wave | Mechanism | Phase |
|---|---|---|
| a wave | Atrial contraction | Phase A |
| c wave | Tricuspid valve bulges into atrium during IVC | Phase B |
| x descent | Atrial relaxation + tricuspid pulled downward during ventricular systole | Systole |
| v wave | Venous filling of atria while tricuspid is closed | Phase E |
| y descent | Tricuspid opens → atrial emptying | Phase F |
Heart Sounds Summary
| Sound | Cause | Timing | Clinical Note |
|---|---|---|---|
| S1 | Closure of mitral (+tricuspid) | Start of systole (IVC) | Physiological splitting is normal |
| S2 | Closure of aortic (+pulmonic) | Start of diastole (IVR) | Splits on inspiration (normal) |
| S3 | Rapid ventricular filling | Early diastole (Phase F) | Normal in children; heart failure in adults |
| S4 | Atrial contraction into stiff ventricle | Late diastole (Phase A) | Always abnormal; LV hypertrophy, ischemia |
Effect of Heart Rate on Cycle Duration
- At 72 bpm: systole ~0.4 of total cycle; diastole ~0.6
- At 3× normal rate: systole ~0.65 of cycle
- At very high heart rates, diastole shortens disproportionately, impairing ventricular filling
- This is why tachyarrhythmias reduce cardiac output - inadequate filling time
Right vs Left Heart
The events are the same for both ventricles, but:
- Right-sided pressures are lower (pulmonary circulation is a low-resistance circuit)
- RV systolic pressure ~25 mmHg; pulmonary artery systolic ~25 mmHg
- Pulmonic valve closes after aortic valve (especially on inspiration)
- The volume changes of RV and LV are identical (cardiac outputs must match)
Sources: Costanzo Physiology 7th Ed., p. 160-163 | Guyton & Hall Medical Physiology | Medical Physiology (Boron & Boulpaep), p. 746
Give me proper cardiac cycle note for 1st year paramedical student
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I have all the content I need. Here is the simplified, student-friendly note:
🫀 The Cardiac Cycle
Notes for 1st Year Paramedical Students
What is the Cardiac Cycle?
The cardiac cycle is all the events that happen in the heart during one complete heartbeat - from the start of one beat to the start of the next.
- At a normal heart rate of 72 beats per minute, one cardiac cycle lasts about 0.8 seconds
- Every cycle has two main phases:
- Systole = heart muscle contracting (squeezing blood out)
- Diastole = heart muscle relaxing (filling with blood)
Simple formula: Duration of cycle = 60 ÷ Heart rate Example: 60 ÷ 75 beats/min = 0.8 seconds per beat
How Does the Cycle Start?
Each heartbeat starts with an electrical signal from the SA node (Sinoatrial node) - the natural pacemaker of the heart, located in the right atrium.
- The signal travels through the atria first → atria contract
- Then it passes through the AV node (with a slight delay of 0.1 sec) → ventricles contract
- This delay is important - it lets the atria finish squeezing blood into the ventricles before the ventricles contract
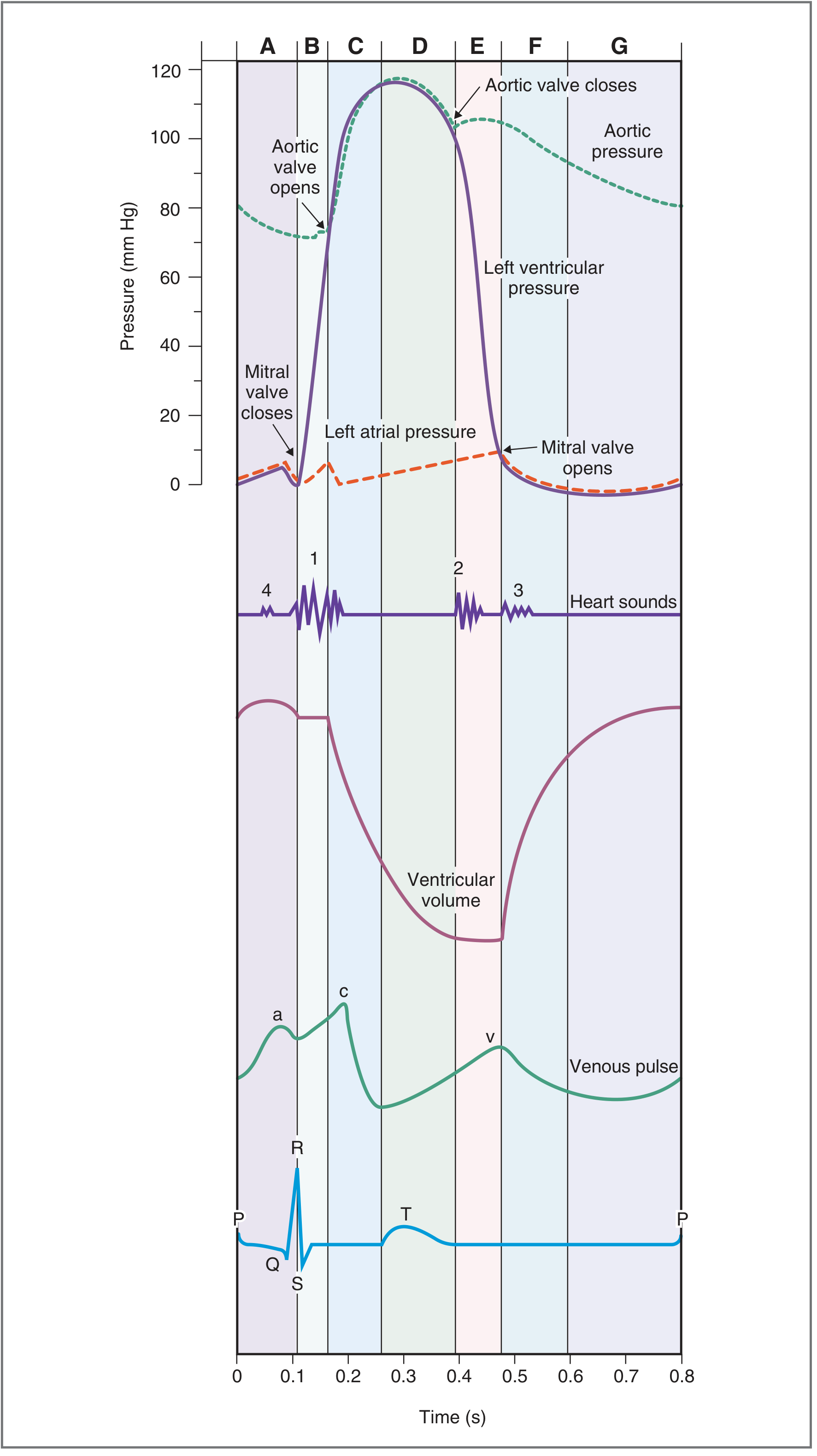
The Cardiac Cycle Diagram (Wiggers Diagram)
This diagram shows all the events of one cardiac cycle. The 7 phases are labeled A to G. Read it top to bottom: pressure changes → ventricular volume → venous pulse → ECG.
The 7 Phases of the Cardiac Cycle
The cycle is divided into 7 phases (A through G):
🔵 DIASTOLE (Relaxation Phase)
Phase A - Atrial Systole ("Atria Squeeze")
What happens: The atria contract and push the last bit of blood into the ventricles.
| What to Note | Detail |
|---|---|
| ECG | P wave (atria are electrically activated) |
| Valves | Mitral valve is OPEN; Aortic valve is CLOSED |
| Blood flow | Blood moves from left atrium → left ventricle |
| Heart sound | S4 (usually not heard in normal healthy adults) |
Think of it as: The atria giving the ventricles a final "top-up" of blood before the big squeeze.
🔴 SYSTOLE (Contraction Phase)
Phase B - Isovolumetric Ventricular Contraction ("Pressure Build-Up")
What happens: The ventricles start to contract but no blood is ejected yet - all valves are closed.
| What to Note | Detail |
|---|---|
| ECG | QRS complex (ventricles electrically activated) |
| Valves | Mitral valve CLOSES → ALL VALVES CLOSED |
| Ventricular pressure | Rises steeply |
| Ventricular volume | No change (isovolumetric = "same volume") |
| Heart sound | S1 - "Lub" (mitral valve snapping shut) |
Think of it as: Squeezing a closed water balloon - pressure builds but no water escapes yet.
"Isovolumetric" = both the inlet (mitral) and outlet (aortic) valves are closed, so volume stays the same even as pressure rises.
Phase C - Rapid Ventricular Ejection ("Fast Pumping")
What happens: Ventricular pressure exceeds aortic pressure, aortic valve opens, blood rushes out fast.
| What to Note | Detail |
|---|---|
| ECG | ST segment |
| Valves | Aortic valve OPENS |
| Ventricular pressure | Reaches its peak (~120 mmHg) |
| Ventricular volume | Falls sharply - most blood is ejected here |
| Aortic pressure | Rises rapidly |
| Heart sound | None |
Think of it as: A dam breaking - blood rushes into the aorta rapidly.
Phase D - Reduced Ventricular Ejection ("Slow Pumping")
What happens: The ventricle starts to relax, ejection slows down but continues.
| What to Note | Detail |
|---|---|
| ECG | T wave (ventricles repolarizing/relaxing) |
| Valves | Aortic valve still open |
| Ventricular pressure | Starts to fall |
| Ventricular volume | Reaches its minimum (End-Systolic Volume ~50 mL) |
| Heart sound | None |
Think of it as: The last trickle of water coming out of a squeezed sponge.
🔵 DIASTOLE (Relaxation Phase - resumes)
Phase E - Isovolumetric Ventricular Relaxation ("Pressure Drop")
What happens: Ventricles fully relax; aortic valve closes; all valves are closed again.
| What to Note | Detail |
|---|---|
| ECG | After T wave |
| Valves | Aortic valve CLOSES → ALL VALVES CLOSED |
| Ventricular pressure | Falls sharply |
| Ventricular volume | No change (isovolumetric again) |
| Aortic pressure | Shows Dicrotic Notch (small "blip" when valve closes) |
| Heart sound | S2 - "Dub" (aortic valve snapping shut) |
Think of it as: The balloon deflating inside a sealed box - pressure drops rapidly.
The dicrotic notch on the aortic pressure curve is a small dip that marks the exact moment the aortic valve closes.
Phase F - Rapid Ventricular Filling ("Fast Filling")
What happens: Mitral valve opens, blood rushes from the atrium into the relaxed ventricle.
| What to Note | Detail |
|---|---|
| ECG | Flat line (between beats) |
| Valves | Mitral valve OPENS |
| Ventricular pressure | Low and relatively flat |
| Ventricular volume | Rises rapidly (~70-80% of filling happens here) |
| Heart sound | S3 (normal in children; sign of heart failure in adults >40 yrs) |
Think of it as: A dry sponge rapidly soaking up water when dropped into a bowl.
Phase G - Reduced Ventricular Filling / Diastasis ("Slow Filling")
What happens: Filling continues slowly; atrial and ventricular pressures nearly equalize.
| What to Note | Detail |
|---|---|
| ECG | Flat line |
| Valves | Mitral valve still open |
| Ventricular volume | Rises slowly toward plateau |
| Heart sound | None |
Think of it as: That last slow drip of water into an almost-full glass.
Then the P wave appears again, and the whole cycle repeats from Phase A.
Quick Summary Table
| Phase | Name | ECG | Valve Action | Volume | Heart Sound |
|---|---|---|---|---|---|
| A | Atrial Systole | P wave | - | ↑ slightly | S4 |
| B | Isovolumetric Contraction | QRS | Mitral closes | No change | S1 (Lub) |
| C | Rapid Ejection | ST segment | Aortic opens | ↓↓ fast | - |
| D | Reduced Ejection | T wave | - | ↓ to ESV | - |
| E | Isovolumetric Relaxation | Post-T | Aortic closes | No change | S2 (Dub) |
| F | Rapid Filling | Flat | Mitral opens | ↑↑ fast | S3 |
| G | Diastasis | Flat | - | ↑ slowly | - |
Key Numbers to Remember
| Term | Value |
|---|---|
| Normal heart rate | 72 beats/min |
| Duration of one cycle | ~0.8 seconds |
| Systole duration | ~0.3 sec |
| Diastole duration | ~0.5 sec |
| End-Diastolic Volume (EDV) | ~130 mL (how full the heart is before ejection) |
| End-Systolic Volume (ESV) | ~50 mL (how much blood is left after ejection) |
| Stroke Volume (SV) | ~80 mL (EDV - ESV = blood pumped per beat) |
| Ejection Fraction (EF) | ~60% (normal = above 55%) |
| Peak LV pressure (systolic) | ~120 mmHg |
| LV pressure at rest (diastolic) | ~8 mmHg |
The 4 Heart Sounds - Simple Memory Aid
| Sound | "Name" | When | Cause | Normal? |
|---|---|---|---|---|
| S1 | "Lub" | Start of systole | Mitral + Tricuspid valves closing | ✅ Always normal |
| S2 | "Dub" | Start of diastole | Aortic + Pulmonic valves closing | ✅ Always normal |
| S3 | "Kentucky" (Ken-tuc-ky) | Early diastole | Rapid filling vibrates the ventricle | ✅ Normal in kids; ❌ Heart failure in adults |
| S4 | "Tennessee" (Ten-nes-see) | Late diastole | Stiff ventricle resists atrial filling | ❌ Always abnormal |
Memory trick for normal heart sounds: Listen for "Lub-Dub" - S1 then S2. That is one complete heartbeat.
Systole vs. Diastole - At a Glance
| Feature | Systole | Diastole |
|---|---|---|
| Heart action | Contracting | Relaxing |
| Blood flow | Out of ventricles → aorta/pulmonary artery | Into ventricles from atria |
| Valves open | Aortic + Pulmonic | Mitral + Tricuspid |
| Duration (at rest) | ~0.3 seconds | ~0.5 seconds |
| ECG | QRS to end of T wave | T wave to next QRS |
| Blood pressure measured | Systolic BP (top number ~120) | Diastolic BP (bottom number ~80) |
Why is Diastole Longer Than Systole?
The heart needs more time to fill than to empty. At rest, diastole is roughly twice as long as systole. This is why fast heart rates (like in tachycardia) reduce the heart's pumping efficiency - diastole gets shortened too much and the ventricles do not fill properly before the next beat.
Clinical Relevance for Paramedics
| Situation | What Happens in the Cardiac Cycle |
|---|---|
| High blood pressure | The aortic valve needs extra force to open; ventricle works harder |
| Tachycardia (fast HR) | Diastole shortens, less filling time, stroke volume falls |
| Heart failure | S3 sound heard - ventricle is too full/floppy |
| Aortic stenosis | Aortic valve is narrowed; murmur heard during systole (Phases C-D) |
| Mitral stenosis | Mitral valve is narrowed; murmur heard during diastole (Phase F) |
Source: Costanzo Physiology 7th Ed. | Guyton & Hall Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.