Difference of croup and epiglottis, give possible differential diagnosis for stridor and important history taking.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have comprehensive data from multiple authoritative sources. Let me compile the full answer.
Croup vs. Epiglottitis: Full Clinical Comparison, Differential Diagnosis of Stridor, and History Taking
1. Croup vs. Epiglottitis - Key Differences
The following comparison is drawn directly from Rosen's Emergency Medicine and Scott-Brown's Otolaryngology, with bacterial tracheitis included as an important "third" entity to distinguish.
| Parameter | Croup (Viral Laryngotracheobronchitis) | Epiglottitis (Supraglottitis) | Bacterial Tracheitis |
|---|---|---|---|
| Peak age | 6 months - 3 years | 5-7 years (now increasingly adults) | 3-5 years (but seen throughout childhood) |
| Onset | Gradual (2-3 day URI prodrome) | Rapid progression over hours | Several-day croup-like prodrome then rapid deterioration |
| Pathology | Subglottic mucosal edema (narrowest part of pediatric airway) | Inflammation/edema of epiglottis and aryepiglottic folds | Bacterial superinfection; mucopurulent secretions obstructing the trachea |
| Organisms | Parainfluenza virus type I (most common), RSV, adenovirus, influenza | H. influenzae type b (Hib), Group A beta-hemolytic streptococcus, S. aureus, S. pneumoniae | S. aureus (most common) or mixed flora |
| Fever | Low-grade (38-38.5°C) | High fever, toxic appearance | High fever, toxic appearance |
| Cough | Classic barky, seal-like cough | Absent or minimal | Variable |
| Voice/cry | Hoarse voice | Muffled/"hot potato" voice, often absent | Variable |
| Stridor | Inspiratory stridor | Inspiratory stridor (biphasic if severe) | Inspiratory AND expiratory (biphasic) |
| Drooling | Absent | Prominent (cannot swallow secretions) | Variable |
| Posture | Normal or prefers sitting | Tripod/sniffing position - jaw jutted forward, neck extended | Usually too ill, recumbent |
| Toxicity | Child appears well or mildly ill | Child appears toxic, anxious | Child appears very toxic |
| Response to steroids/epinephrine | Responds well | Does not reliably respond | Fails to respond (key distinguishing feature) |
| X-ray (AP neck) | "Steeple sign" (subglottic narrowing) | "Thumbprint sign" (enlarged epiglottis on lateral view), thickened aryepiglottic folds, loss of vallecula air | Shaggy/irregular tracheal air column |
| Management | Steroids (dexamethasone), nebulized epinephrine, oxygen; rarely needs intubation | Secure airway first (OR, with tracheostomy tray); IV antibiotics | Intubation almost always needed; IV antibiotics |
Key clinical pearl: Children with croup do NOT drool and do NOT look toxic - in contrast to epiglottitis. Drooling + tripod position + toxic appearance = epiglottitis until proven otherwise.
- ROSEN's Emergency Medicine, p. 3174; Scott-Brown's Otolaryngology, p. 369
Radiographic Signs
Croup - "Steeple Sign" (AP chest/neck X-ray):
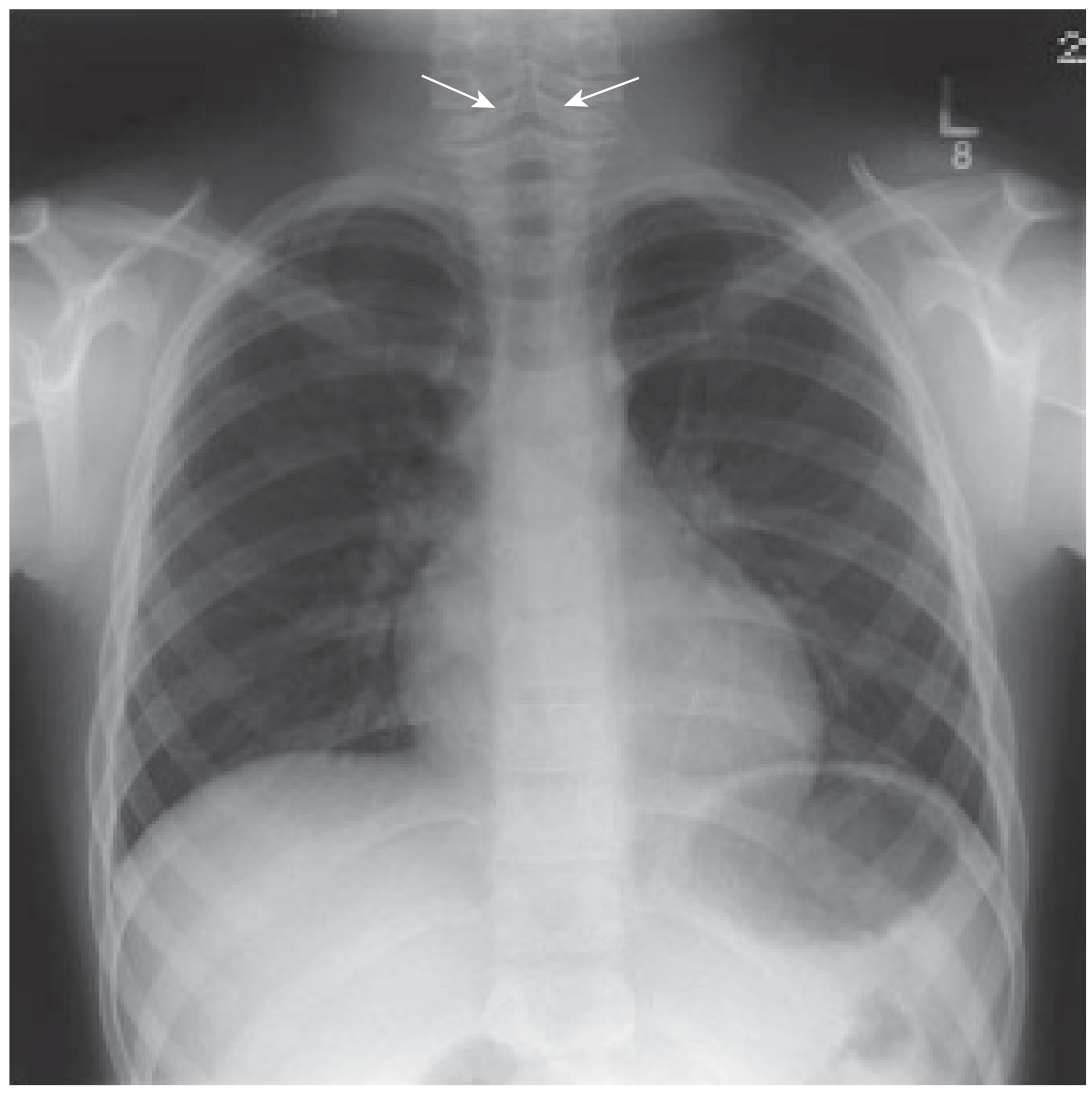 Narrowing of the subglottic airway on AP view due to mucosal edema (arrows). - Scott-Brown's Otolaryngology
Narrowing of the subglottic airway on AP view due to mucosal edema (arrows). - Scott-Brown's Otolaryngology
Epiglottitis - "Thumbprint Sign" (lateral neck X-ray):
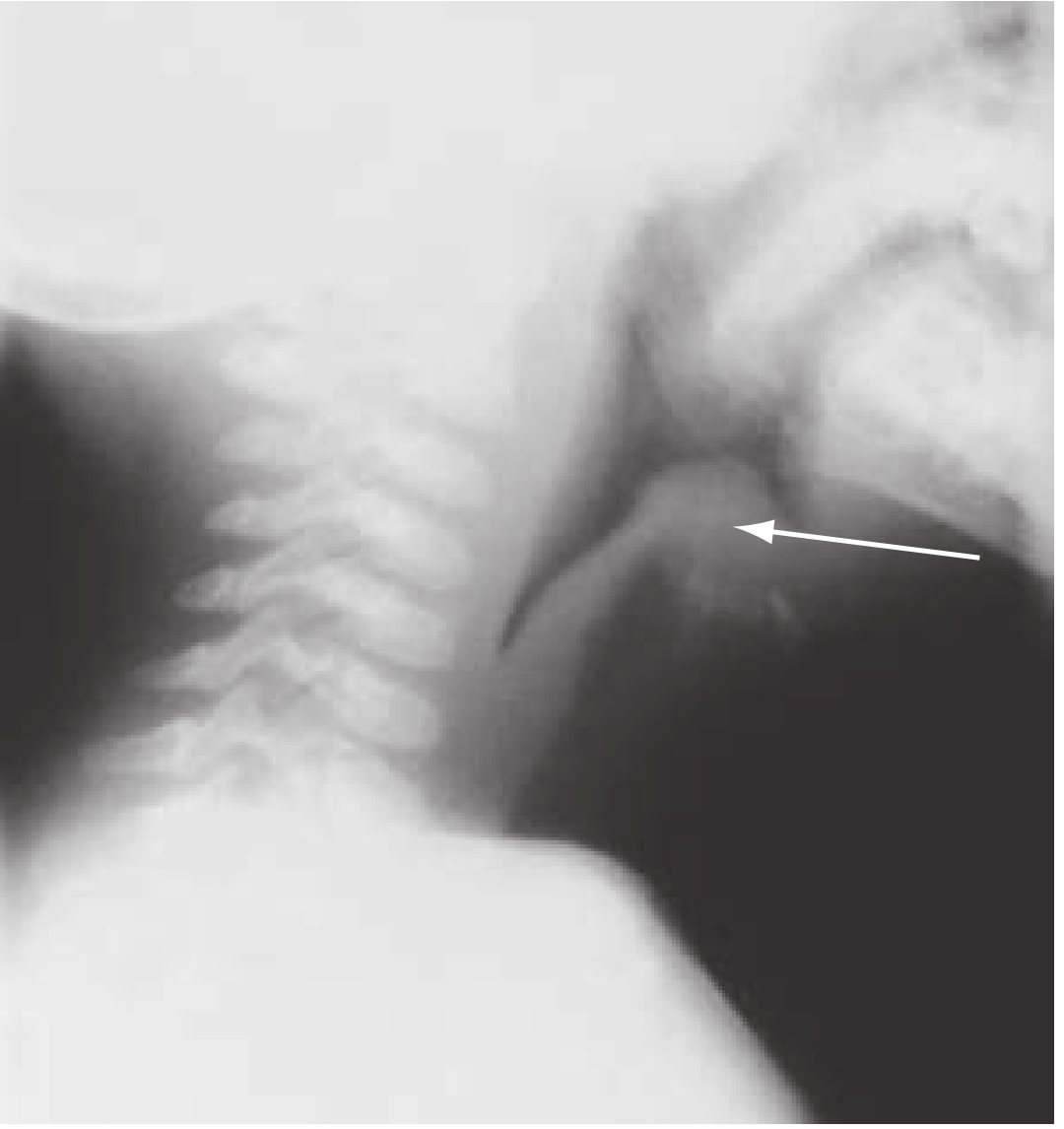 Enlarged, thumb-like epiglottis on lateral neck radiograph (arrow). Up to 70% of cases may have normal radiographs. - ROSEN's Emergency Medicine
Enlarged, thumb-like epiglottis on lateral neck radiograph (arrow). Up to 70% of cases may have normal radiographs. - ROSEN's Emergency Medicine
Important note on epiglottitis today: Due to widespread Hib vaccination, epiglottitis is now far less common in vaccinated children. It has increasingly become a disease of adults and unvaccinated individuals. Other organisms (Group A strep, S. aureus) now account for more cases. - Morgan & Mikhail's Clinical Anesthesiology, p. 1718
2. Differential Diagnosis of Stridor
Stridor is a symptom, not a diagnosis. The differential depends primarily on age and acuity of onset.
By Age Group
Infants < 6 months (usually congenital/structural):
| Cause | Key Features |
|---|---|
| Laryngomalacia | Most common (60% of neonatal laryngeal problems); stridor from birth; worsens with crying, improves prone/with neck extension; resolves by 18 months |
| Vocal cord paralysis | Hoarse cry (unilateral) or normal voice with stridor + dyspnea (bilateral); may cause cyanosis |
| Subglottic stenosis | Congenital or acquired; persistent stridor; often misdiagnosed as recurrent croup |
| Airway hemangioma | Subglottic; progressive; may have cutaneous hemangiomas |
| Vascular ring/sling | Persistent stridor + feeding problems; right-sided aortic arch on CXR |
| Tracheomalacia | Stridor worsens first weeks of life; worsens supine/with agitation |
Children > 6 months (usually infectious/acquired):
| Cause | Key Features |
|---|---|
| Croup | Age 6 months - 3 years; barky cough, hoarseness, low-grade fever; gradual onset |
| Epiglottitis | Rapid onset; toxic; drooling; tripod position; high fever |
| Bacterial tracheitis | Croup-like then toxic; fails steroids/epinephrine; biphasic stridor |
| Foreign body aspiration | Sudden onset (no fever); age 6 months - 5 years; witnessed choking episode; variation in stridor pattern |
| Retropharyngeal abscess | Fever, neck stiffness, neck swelling, refusal to move neck |
| Peritonsillar abscess | Older child; muffled "hot potato" voice, uvular deviation, trismus |
| Angioedema | Allergic history; urticaria; rapid onset; lip/tongue swelling |
| Spasmodic/atypical croup | Recurrent episodes; associated with allergy, atopy, GERD; no fever |
Adults (wider differential):
| Cause | Key Features |
|---|---|
| Acute epiglottitis | Now more common in adults |
| Anaphylaxis/angioedema | Allergic trigger, rapid onset |
| Laryngeal/tracheal neoplasm | Progressive, chronic hoarseness |
| Laryngeal trauma | History of injury |
| Bilateral vocal cord paralysis | Post-thyroid surgery, malignancy |
| Tracheal stenosis | Post-intubation history |
| Thyroid goiter | Gradually enlarging neck mass |
Tintinalli's Emergency Medicine, Table 126-1; Scott-Brown's Otolaryngology, p. 369
By Phase of Stridor (Anatomical Localization)
- Inspiratory only → Supraglottic obstruction (above true vocal cords)
- Expiratory only → Subglottic/intrathoracic obstruction
- Biphasic → At the level of the true vocal cords, or severe obstruction
- Marked variation in pattern → Consider foreign body until proven otherwise
3. Important History Taking for Stridor
Onset and Duration
- When did the stridor start? (sudden vs. gradual)
- How has it progressed? (worsening, stable, improving, intermittent/recurrent)
- Present at birth or developed later?
Character of Stridor
- Is it inspiratory, expiratory, or both?
- Is it constant or positional? (worse lying down, improves in certain positions)
- Does it worsen with crying/agitation or improve?
- Does it vary throughout the day?
Associated Symptoms
- Fever? (suggests infectious cause - croup, epiglottitis, bacterial tracheitis, abscess)
- Cough? barky/seal-like (croup) vs. absent (epiglottitis)
- Hoarseness or voice change? (laryngeal involvement)
- Drooling? (cannot swallow - epiglottitis/retropharyngeal abscess)
- Dysphagia or odynophagia? (epiglottitis, retropharyngeal abscess)
- Posture preference? (tripod = epiglottitis)
- Cyanosis or apneic episodes?
- Feeding difficulties or failure to thrive? (chronic structural cause)
- Skin lesions? (hemangiomas - may suggest subglottic hemangioma)
Precipitating Event
- Witnessed choking episode? (foreign body aspiration - must exclude until proven otherwise)
- Recent intubation or airway instrumentation?
- Trauma to the neck/airway?
- Exposure to allergen? Drug exposure? (angioedema)
Birth and Neonatal History
- Prematurity? (increases risk of subglottic stenosis from intubation)
- Neonatal ICU stay, intubation history?
- Perinatal complications?
- Onset of stridor shortly after birth vs. later? (congenital vs. acquired)
Medical History
- Vaccination status - particularly Hib vaccine (changes risk of epiglottitis significantly)
- Known congenital anomalies (Down syndrome, DiGeorge - associated with tracheomalacia/structural abnormalities)
- Cardiac anomalies (vascular rings, pulmonary sling)
- History of atopy, allergy, asthma, GERD (spasmodic croup)
- Immunodeficiency (necrotizing epiglottitis, unusual organisms)
- Recurrent episodes? (subglottic stenosis, recurrent croup, papillomatosis, tracheomalacia)
Family History
- Atopy/allergies
- History of hereditary angioedema
Social History
- Daycare exposure, sick contacts (viral croup spreads in epidemics - seasonal peaks autumn/winter)
- Small toys or objects accessible to child (foreign body risk)
"A thorough history and examination will often lead to a working diagnosis. Inquire about the time and events surrounding the onset of stridor, the presence of fever, known congenital anomalies, cardiac abnormalities, perinatal complications, prematurity, neonatal intensive care unit interventions, and previous endotracheal intubation or instrumentation." - Tintinalli's Emergency Medicine
Key Clinical Summary
| Croup | Epiglottitis | |
|---|---|---|
| Red flag to rule OUT epiglottitis | Absent drooling, low-grade fever, barky cough, appears non-toxic | Drooling + tripod + toxic + rapid onset = EMERGENCY |
| Don't do | Unnecessary investigation if mild | Do NOT examine throat, do NOT lay patient down - risk of total obstruction |
| Airway | Rarely needs securing | Secure in OR with tracheostomy tray ready |
| Treatment | Dexamethasone + nebulized epinephrine | Intubation + IV antibiotics (ceftriaxone) |
Sources: ROSEN's Emergency Medicine, p. 3167-3174; Morgan & Mikhail's Clinical Anesthesiology, p. 1718-1719; Scott-Brown's Otolaryngology Head & Neck Surgery, p. 369-371; Tintinalli's Emergency Medicine, Table 126-1; K.J. Lee's Essential Otolaryngology, p. 1030
This is a shared conversation. Sign in to Orris to start your own chat.