Give me info about Cranial nerves
Reading File
Finding Sources
Searching Images
cranial nerves overview diagram
Reading File
Reading File
Reading File
Loading Image
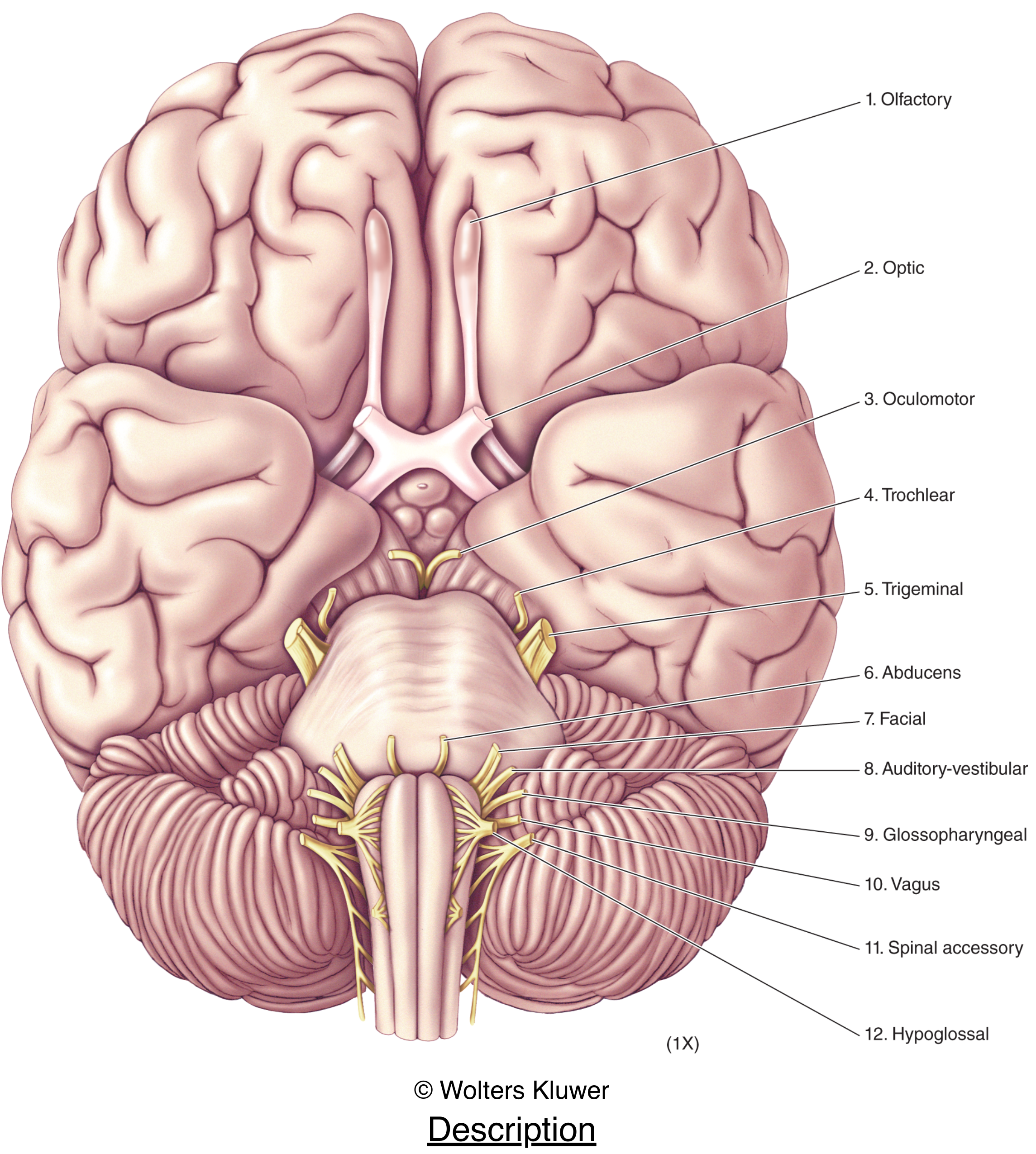
Here is a comprehensive overview of the 12 cranial nerves, sourced from Neuroscience: Exploring the Brain and Gray's Anatomy for Students.
The 12 Cranial Nerves
Twelve pairs of cranial nerves emerge from the base of the brain and pass through foramina or fissures in the cranial cavity. The first two (Olfactory and Optic) are technically parts of the CNS; the remaining ten are peripheral nerves. Each has associated nuclei in the midbrain, pons, or medulla.
Quick Reference Table
| # | Name | Fiber Type | Key Function | Skull Exit |
|---|---|---|---|---|
| I | Olfactory | Special sensory (SA) | Smell | Cribriform plate of ethmoid |
| II | Optic | Special sensory (SA) | Vision | Optic canal |
| III | Oculomotor | Somatic motor (GSE) + Visceral motor (GVE) | Eye/eyelid movement; pupil constriction (parasympathetic) | Superior orbital fissure |
| IV | Trochlear | Somatic motor (GSE) | Eye movement (superior oblique muscle) | Superior orbital fissure |
| V | Trigeminal | Somatic sensory (GSA) + Somatic motor (BE) | Facial touch/pain/temperature; muscles of mastication | Superior orbital fissure (V1), foramen rotundum (V2), foramen ovale (V3) |
| VI | Abducens | Somatic motor (GSE) | Eye movement (lateral rectus muscle) | Superior orbital fissure |
| VII | Facial | Somatic motor (BE) + Special sensory (SA) + Visceral motor (GVE) | Muscles of facial expression; taste (anterior 2/3 tongue); lacrimal & salivary glands | Stylomastoid foramen |
| VIII | Vestibulocochlear | Special sensory (SA) | Hearing (cochlear division); balance (vestibular division) | Internal acoustic meatus |
| IX | Glossopharyngeal | Mixed (GSA, GVA, SA, GVE, BE) | Taste (posterior 1/3 tongue); parotid gland; carotid sinus/body sensing; stylopharyngeus muscle | Jugular foramen |
| X | Vagus | Mixed (GSA, GVA, SA, GVE, BE) | Parasympathetic to heart/lungs/abdominal viscera; visceral sensation; pharynx/larynx muscles | Jugular foramen |
| XI | Accessory | Somatic motor (BE) | Sternocleidomastoid & trapezius muscles | Jugular foramen |
| XII | Hypoglossal | Somatic motor (GSE) | All intrinsic tongue muscles + hyoglossus, genioglossus, styloglossus | Hypoglossal canal |
Functional Component Types
Cranial nerves carry several types of fibers not found in spinal nerves:
| Abbreviation | Full Name | Function |
|---|---|---|
| GSA | General Somatic Afferent | Touch, pain, temperature |
| GVA | General Visceral Afferent | Sensory from viscera |
| SA | Special Afferent | Smell, taste, vision, hearing, balance |
| GSE | General Somatic Efferent | Motor to voluntary muscles |
| GVE | General Visceral Efferent | Motor to smooth muscle, cardiac muscle, glands |
| BE | Branchial Efferent | Motor to pharyngeal arch–derived skeletal muscles |
Individual Nerve Highlights
CN I — Olfactory
Olfactory receptor neurons in the nasal epithelium project axons through the cribriform plate directly to the olfactory bulb. It is the only sensory nerve that projects ipsilaterally without a thalamic relay.
CN II — Optic
Actually a CNS tract (myelinated by oligodendrocytes, not Schwann cells). Fibers from nasal retina cross at the optic chiasm; fibers from temporal retina remain ipsilateral. Projects to the lateral geniculate nucleus, superior colliculus, and pretectum.
CN III — Oculomotor
Innervates four of the six extraocular muscles (superior, inferior, medial rectus; inferior oblique) plus levator palpebrae superioris. The visceral motor (parasympathetic) component controls the sphincter pupillae (pupil constriction) and ciliary muscle (accommodation). A blown pupil (dilated, fixed) is a classic sign of CN III compression.
CN IV — Trochlear
The only cranial nerve to exit from the dorsal surface of the brainstem and the only one to decussate entirely before exiting. Innervates the superior oblique muscle (depression and intorsion of the adducted eye).
CN V — Trigeminal (3 divisions)
- V1 (Ophthalmic) — Forehead, scalp, cornea, nasal mucosa
- V2 (Maxillary) — Cheek, upper lip, upper teeth, nasal cavity
- V3 (Mandibular) — Lower lip, lower teeth, chin, anterior tongue (general sensation), and motor to muscles of mastication (masseter, temporalis, pterygoids)
CN VI — Abducens
Innervates only the lateral rectus muscle (abduction of the eye). Long intracranial course makes it vulnerable in raised intracranial pressure → false localizing sign.
CN VII — Facial
- Motor: muscles of facial expression (derived from 2nd pharyngeal arch), stapedius, posterior digastric, stylohyoid
- Sensory: taste from anterior 2/3 of tongue via chorda tympani
- Parasympathetic: lacrimal gland, submandibular & sublingual salivary glands
- Bell's palsy = LMN lesion → ipsilateral complete facial paralysis (including forehead)
CN VIII — Vestibulocochlear
Two divisions: the cochlear nerve (hearing — hair cells in the organ of Corti) and the vestibular nerve (balance — hair cells in the semicircular canals, utricle, saccule). Nuclei lie at the pontomedullary junction.
CN IX — Glossopharyngeal
- Sensory: posterior 1/3 of tongue (taste + general sensation), carotid sinus/body (baroreception, chemoreception), middle ear, pharynx
- Motor: stylopharyngeus (sole muscle it innervates)
- Parasympathetic: parotid gland (via otic ganglion)
- Clinical: loss → absent gag reflex (afferent limb)
CN X — Vagus ("Wandering")
The most widely distributed cranial nerve. Provides parasympathetic control of the heart (slows rate), lungs, esophagus, and abdominal viscera as far as the splenic flexure. Motor branches (via recurrent laryngeal nerve) innervate almost all laryngeal muscles — damage → hoarseness.
CN XI — Accessory
Innervates the sternocleidomastoid (ipsilateral head rotation away from lesion) and trapezius (shoulder shrug). Note: the nerve actually has both a cranial root (joining CN X) and a spinal root arising from C1–C5.
CN XII — Hypoglossal
Pure motor to all intrinsic tongue muscles and the hyoglossus, genioglossus, and styloglossus. LMN lesion → tongue deviates toward the side of the lesion on protrusion (ipsilateral weakness).
Clinical Pearl: Mnemonic
"On Old Olympus' Towering Top, A Finn And German Viewed Some Hops" — first letter of each word = CN I through XII (Olfactory, Optic, Oculomotor, Trochlear, Trigeminal, Abducens, Facial, Auditory-vestibular, Glossopharyngeal, Vagus, Spinal accessory, Hypoglossal).
Fiber type mnemonic: "Some Say Marry Money But My Brother Says Big Brains Matter More" — S = sensory, M = motor, B = both (applied sequentially to CNs I–XII).
Sources: Neuroscience: Exploring the Brain, 5th Ed., pp. 701–704; Gray's Anatomy for Students, 4th Ed., pp. 1033–1035
Breathing condition me badhti hai
Asking for Preferences
Finding Sources
Searching PubMed
"sleep apnea" AND treatment
Reading File
Reading File
Finding Sources
Reading File
Searching Images
obstructive sleep apnea airway diagram CPAP treatment
Ab main aapko Sleep Apnea ke baare mein puri detail deta hoon - Hindi mein, textbooks se liya gaya.
😴 Sleep Apnea (Neend mein Saans Rukna)
🔍 Kya Hota Hai Sleep Apnea Mein?
Sleep apnea ek aisi condition hai jisme neend ke dauran saans baar baar rukti hai - har episode kam se kam 10 second ya usse zyada ka hota hai. Raat bhar aisi 300 se 500 episodes ho sakti hain. Har baar saans rukne se:
- Blood mein oxygen kam ho jaata hai (PO₂ gir jaata hai)
- CO₂ badh jaata hai
- Brain signal deta hai - achanak jaag ke saans leni padti hai
- Neend toot jaati hai - chahe yaad na rahe
📋 Teen Types
1. Obstructive Sleep Apnea (OSA) - Sabse Common
Kya hota hai: Gale (pharynx) ki muscles neend mein relax ho jaati hain aur airway band ho jaata hai. Hawa andar nahi ja sakti.
Kise hota hai:
- Mote logon ko (neck mein extra fat airway compress karta hai)
- Bade (older) logon ko
- Badhay huay tonsils ya adenoids walon ko
- Bade tongue walon ko
Symptoms:
- 🔊 Zor se kharrate (snoring)
- 😴 Din mein neend aana (excessive daytime sleepiness)
- Subah uthke sir dard
- Raat ko baar baar uthna
- Pair mein partner ki shikayat
2. Central Sleep Apnea (CSA)
Kya hota hai: Airway theek hai, lekin brain se signal hi nahi jaata respiratory muscles ko. CNS ka respiratory drive temporarily band ho jaata hai.
Kaaran: Brain injury, stroke, ya respiratory centers ki koi bimari. Yeh log sedatives aur painkillers ke liye bahut sensitive hote hain.
3. Mixed (Complex) Sleep Apnea
- OSA aur CSA dono ka combination
- Lagbhag 15% cases mein hota hai
- Kabhi kabhi CPAP shuru karne par bhi CSA nikal aata hai
⚕️ Complications - Agar Treatment Na Ho
Sleep apnea sirf thakaan ka masla nahi - iske serious natije hote hain:
| Organ | Asar |
|---|---|
| Dil | High blood pressure, heart rate badh jaati hai |
| Lungs | Pulmonary hypertension |
| Dimag | Stroke ka risk, memory problems |
| Blood vessels | Sympathetic activity badhti hai |
| Overall | Cardiovascular disease ka risk bahut zyada |
JAMA (2023) meta-analysis mein paya gaya ki jo log CPAP treatment follow karte hain, unmein recurrent cardiovascular events ka risk kam hota hai (PMID: 37787793).
🩺 Diagnosis Kaise Hoti Hai?
STOP-Bang Questionnaire (Screening tool):
- Snoring - kya kharrate aate hain?
- Tired - din mein thakaan?
- Observed apnea - kisi ne saans rukti dekhi?
- Pressure - high blood pressure?
- BMI - 35 se zyada?
- Age - 50 se upar?
- Neck size - badi?
- Gender - mard?
Epworth Sleepiness Scale
Yeh test check karta hai ki aap kahan kahan so jaate hain (TV dekhte, car mein baithke, baatein karte). Score 10+ ho to daaktar se milein.
Polysomnography (Sleep Study) - Gold Standard
Raat ko lab mein ya ghar par monitor karke:
- Breathing patterns
- Blood oxygen levels
- Brain activity
- Heart rate
AHI (Apnea-Hypopnea Index): Ek ghante mein kitni baar saans ruki - isi se severity decide hoti hai.
- 5-15: Mild
- 15-30: Moderate
- 30+: Severe
💊 Treatment
1. CPAP (Continuous Positive Airway Pressure) - Main Treatment
- Ek machine hoti hai jo naak par mask lagake halka pressure deta hai
- Airway khula rakhta hai raat bhar
- Bahut effective hai - OSA aur CSA dono ke liye
- Stroke ke baad iska use recovery improve karta hai
2. Surgery
- Uvulopalatopharyngoplasty (UPPP) - Gale ke peeche ki extra tissue nikalna
- Tonsil/Adenoids nikalna (agar wohi kaaran ho)
- Tracheostomy - severe cases mein trachea mein opening banana
3. Lifestyle Changes
- Weight kam karna - sabse important (neck fat airway compress karta hai)
- Side mein sona (pith ke bal sone se airway aur dabta hai)
- Sharab aur sleeping pills se bachein (muscles aur relax ho jaati hain)
- Smoking band karna
4. Central Sleep Apnea ke liye
- CPAP ya BiPAP
- CO₂ stimulants (saans ko stimulate karne ki dawai)
- Underlying cause treat karna (jaise stroke)
🗓️ Kab Daaktar Se Milen?
Agar aapko ya family member ko yeh problems hain:
- Zor se kharrate + din mein neend
- Koi dekhe ki neend mein saans ruk rahi hai
- Subah sar dard + thakaan daily
- High BP jo control nahi ho raha
Yeh condition serious hai lekin treatment se bahut better ho jaati hai!
Sources: Guyton & Hall Textbook of Medical Physiology; Goldman-Cecil Medicine; Murray & Nadel's Textbook of Respiratory Medicine; Miller's Anesthesia
What is cortex
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.