Posterior interosseous nerve
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have all the information needed for a comprehensive answer. Let me compile it.
Posterior Interosseous Nerve (PIN)
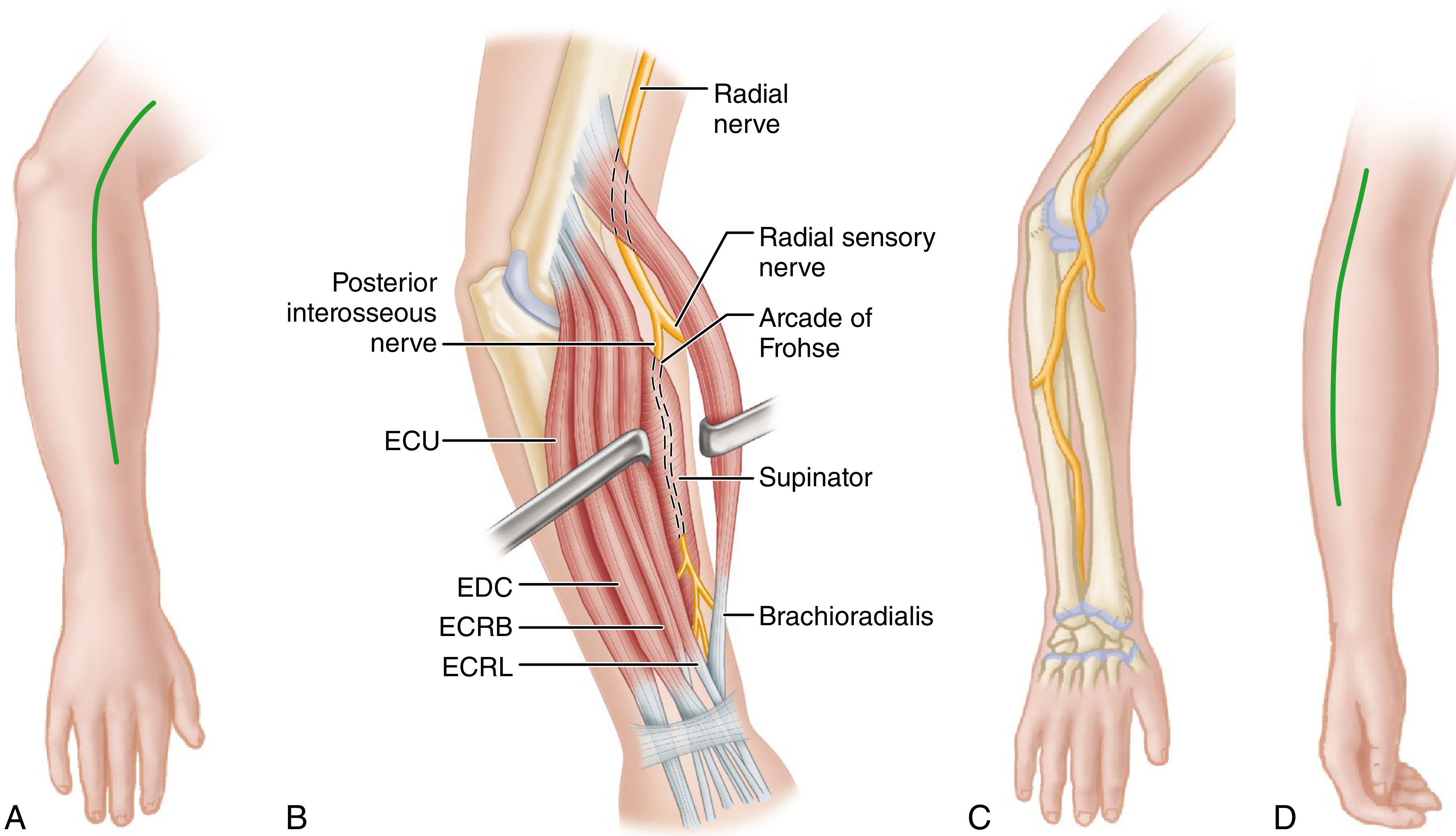
Surgical anatomy of the PIN: the radial nerve divides into the superficial radial sensory nerve and the deep motor branch (PIN), which enters the supinator through the arcade of Frohse. ECU = extensor carpi ulnaris, EDC = extensor digitorum communis, ECRB/ECRL = extensor carpi radialis brevis/longus.
Origin and Course
The PIN is the deep motor branch of the radial nerve (C5-C8, T1), which arises from the posterior cord of the brachial plexus. The radial nerve divides just proximal to the lateral epicondyle into:
- A superficial sensory branch (continues down the radial side of the forearm)
- A deep motor branch - this becomes the PIN
Before becoming the PIN, the deep branch innervates the extensor carpi radialis brevis and gives branches to the supinator. It then pierces the supinator muscle through the arcade of Frohse - a fibrous tendinous arch at the proximal edge of the superficial layer of supinator. After emerging from between the two layers of the supinator muscle, it is formally called the posterior interosseous nerve and runs along the dorsal surface of the interosseous membrane.
The PIN terminates distally as articular branches that pass deep to the extensor pollicis longus to reach the wrist joint.
- Gray's Anatomy for Students, p. 2722-2728
- Imaging Anatomy Vol. 3, p. 3161
Muscles Innervated
The PIN supplies all extensor muscles of the forearm except those already innervated by the radial nerve proper proximal to the bifurcation:
| Muscle | Action |
|---|---|
| Supinator | Supinates forearm |
| Extensor digitorum communis (EDC) | Extends MCP joints of fingers 2-5 |
| Extensor digiti minimi | Extends little finger MCP |
| Extensor carpi ulnaris (ECU) | Extends and adducts wrist |
| Abductor pollicis longus (APL) | Abducts thumb |
| Extensor pollicis brevis (EPB) | Extends thumb MCP |
| Extensor pollicis longus (EPL) | Extends thumb IP joint |
| Extensor indicis proprius | Extends index finger independently |
Spared (innervated proximal to PIN origin): brachioradialis, extensor carpi radialis longus (ECRL), and frequently extensor carpi radialis brevis (ECRB).
Key Anatomical Landmark: Arcade of Frohse
The arcade of Frohse is a fibrous arch formed by the proximal edge of the superficial layer of the supinator muscle. It is the most common site of PIN compression. The nerve is vulnerable here, especially with repetitive pronation/supination. This fibrous arch is present in ~30% of people as a thick tendinous band (vs. a fleshy edge), making compression more likely in those individuals.
- Imaging Anatomy Vol. 3, p. 3161
PIN Syndrome (Posterior Interosseous Nerve Entrapment)
Sites of Compression (4 classic locations in the radial tunnel)
- Fibrous edge of the extensor carpi radialis brevis origin
- Adhesions around the radial head / radiocapitellar joint
- Radial recurrent arterial fan (leash of Henry)
- Arcade of Frohse (most common) - as the PIN enters the supinator; occasionally at the distal border as the nerve exits
Causes
-
Trauma (fracture-dislocations of the elbow, radial head fractures)
-
Inflammatory - especially rheumatoid arthritis (synovitis at the radiocapitellar joint)
-
Space-occupying lesions (lipoma, fibroma, ganglia, hemangioma of supinator, aneurysm of the posterior interosseous artery, schwannoma)
-
Repetitive occupational or athletic stress (violinists, orchestra conductors, swimmers, frisbee players, tennis players)
-
Volkmann ischemic contracture
-
Iatrogenic (radial head resection)
-
Campbell's Operative Orthopaedics 15th Ed, p. 8896-8920
-
Localization in Clinical Neurology 8e, p. 1695-1699
Spinner's Classification
Two types of PIN entrapment:
- Complete - all PIN-supplied muscles paralyzed (EDC, EIP, EDM, ECU, APL, EPB)
- Partial - only one or a few muscles are paralyzed
Clinical Features
| Feature | Detail |
|---|---|
| Pain | Forearm pain, often over the radial tunnel (4-5 cm distal to lateral epicondyle) |
| Wrist extension | Preserved but deviates radially (ECU weak, ECRL/ECRB intact) |
| Finger extension | Loss of MCP extension ("drop-finger" deformity) - IP extension preserved via intrinsics |
| Thumb | Difficulty extending at IP joint, abducting thumb |
| Sensory loss | None - PIN is purely motor |
| Reflexes | Normal |
Key distinguishing point: because ECRL is spared (branches off before PIN) but ECU is paralyzed, the wrist deviates radially on attempted extension. This differs from a high radial nerve palsy (wrist drop) where the wrist cannot extend at all.
An isolated "drop-thumb" deformity can occur if only the descending distal branch is compressed within the supinator (affecting EPL, EPB, APL, and sometimes EIP).
- Rheumatology 2-Volume Set 2022, p. 2893-2904
- Localization in Clinical Neurology 8e, p. 1703-1707
Diagnosis
- Clinical: Radial tunnel tenderness (distal to lateral epicondyle), pain on resisted supination, pain on resisted extension of the long finger (middle finger test)
- EMG/NCS: Confirms denervation in PIN-supplied muscles; rarely diagnostic for radial tunnel syndrome (pain only), but useful to exclude radiculopathy
- MRI: Identifies space-occupying lesions; can show muscle denervation changes
- Differential: Lateral epicondylitis (tennis elbow), posterior cord lesion, C7 radiculopathy
Note: A 2011 study found that 84% of PIN syndromes actually had proximal radial nerve lesions at the upper arm level (partial fascicular lesions) rather than focal compression at the arcade of Frohse - making neuroimaging an important complementary tool. (Localization in Clinical Neurology 8e, p. 1701)
Treatment
Conservative (first-line)
- Rest, NSAIDs, activity modification
- Splinting in wrist/finger extension
- Corticosteroid injection into the radial tunnel
- Physical therapy
Surgical
- Indicated when conservative management fails (typically after 3-6 months), or when a space-occupying lesion is identified
- Surgical decompression of the PIN at the radial tunnel - releasing all four potential compression sites (Campbell's 15th Ed, p. 8950-8956)
- For complete PIN palsy with no recovery after 3-6 months, nerve exploration and repair/grafting may be needed
- Tendon transfers can restore function if nerve recovery is not expected
Summary: PIN vs. Radial Nerve Palsy
| High Radial Nerve Palsy | PIN Syndrome | |
|---|---|---|
| Wrist extension | Lost (wrist drop) | Radially deviated (preserved but weak) |
| Finger MCP extension | Lost | Lost |
| Brachioradialis | Weak | Normal |
| Sensory loss | Dorsal hand/thumb | None |
| Reflexes | Brachioradialis reduced | Normal |
This is a shared conversation. Sign in to Orris to start your own chat.