Gohns complex and it's fate Full details for md exams 15marks answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive textbook content from Robbins (both editions) and Goldman-Cecil. Let me compile the complete 15-mark MD exam answer.
Ghon's Complex — Full Details for MD Examination (15 Marks)
1. DEFINITION
Ghon's complex is the pathological hallmark of primary tuberculosis (TB). It consists of two components:
- Ghon focus — a 1–1.5 cm area of gray-white caseous consolidation in the lung parenchyma
- Regional lymph node involvement — caseous necrosis of the draining hilar/tracheobronchial lymph nodes, connected to the Ghon focus by a lymphangitic streak
The combination of the parenchymal lung lesion + draining lymph node involvement = Ghon complex (also called the Primary complex or Ranke complex when calcified).
(Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 353; Robbins & Kumar Basic Pathology, p. 475)
2. CAUSATIVE ORGANISM
- Mycobacterium tuberculosis (primary pathogen)
- Rarely: M. bovis (from unpasteurized milk) — produces a similar primary complex in the intestine (mesenteric lymph node + intestinal Ghon focus) or tonsil
3. SITE OF THE GHON FOCUS
| Feature | Detail |
|---|---|
| Location in lung | Distal airspaces of the lower part of the upper lobe or upper part of the lower lobe |
| Proximity | Usually subpleural |
| Reason | Bacilli inhaled in aerosol droplets settle in well-ventilated zones (no pre-existing immunity to deflect them) |
| Laterality | Either side; right more common (wider right main bronchus) |
In countries where bovine TB and infected milk have been eliminated, primary TB almost always begins in the lungs (as opposed to intestinal/tonsillar primary complex).
4. PATHOGENESIS — HOW GHON'S COMPLEX FORMS
Stage 1: Initial Infection (Days 1–3)
- Inhaled bacilli (droplet nuclei, 1–5 µm) reach alveoli
- Engulfed by alveolar macrophages, but mycobacteria resist killing by:
- Inhibiting phagolysosome fusion
- Scavenging reactive oxygen intermediates
- Producing lipoarabinomannan (LAM)
- Bacteria multiply within macrophages → macrophage death → local inflammatory exudate
Stage 2: Early Bacillemia (Weeks 1–3)
- Bacilli (free or within phagocytes) drain via lymphatics to regional hilar lymph nodes
- Hematogenous seeding of distant organs (bones, kidneys, meninges, liver, spleen) — clinically silent at this stage
- No cell-mediated immunity yet → no effective killing
Stage 3: Sensitization & Cell-Mediated Immunity (Weeks 3–8)
- Mycobacterial antigens processed by dendritic cells → presented to CD4+ T cells in draining lymph nodes
- IL-12 (from macrophages) drives differentiation into Th1 subset
- Th1 cells secrete IFN-γ → activates macrophages → release:
- TNF (monocyte recruitment)
- iNOS → nitric oxide (bactericidal)
- Antimicrobial peptides (defensins)
- Activated macrophages differentiate into epithelioid histiocytes → fuse to form Langhans giant cells → form granulomas
Stage 4: Granuloma Formation & Caseous Necrosis
- Classic caseating granuloma = central caseous necrosis surrounded by:
- Epithelioid macrophages
- Langhans giant cells (nuclei arranged in horseshoe/ring pattern)
- Peripheral rim of CD4+ lymphocytes
- Fibroblastic capsule
- In the lung → Ghon focus; in lymph nodes → caseating lymphadenopathy
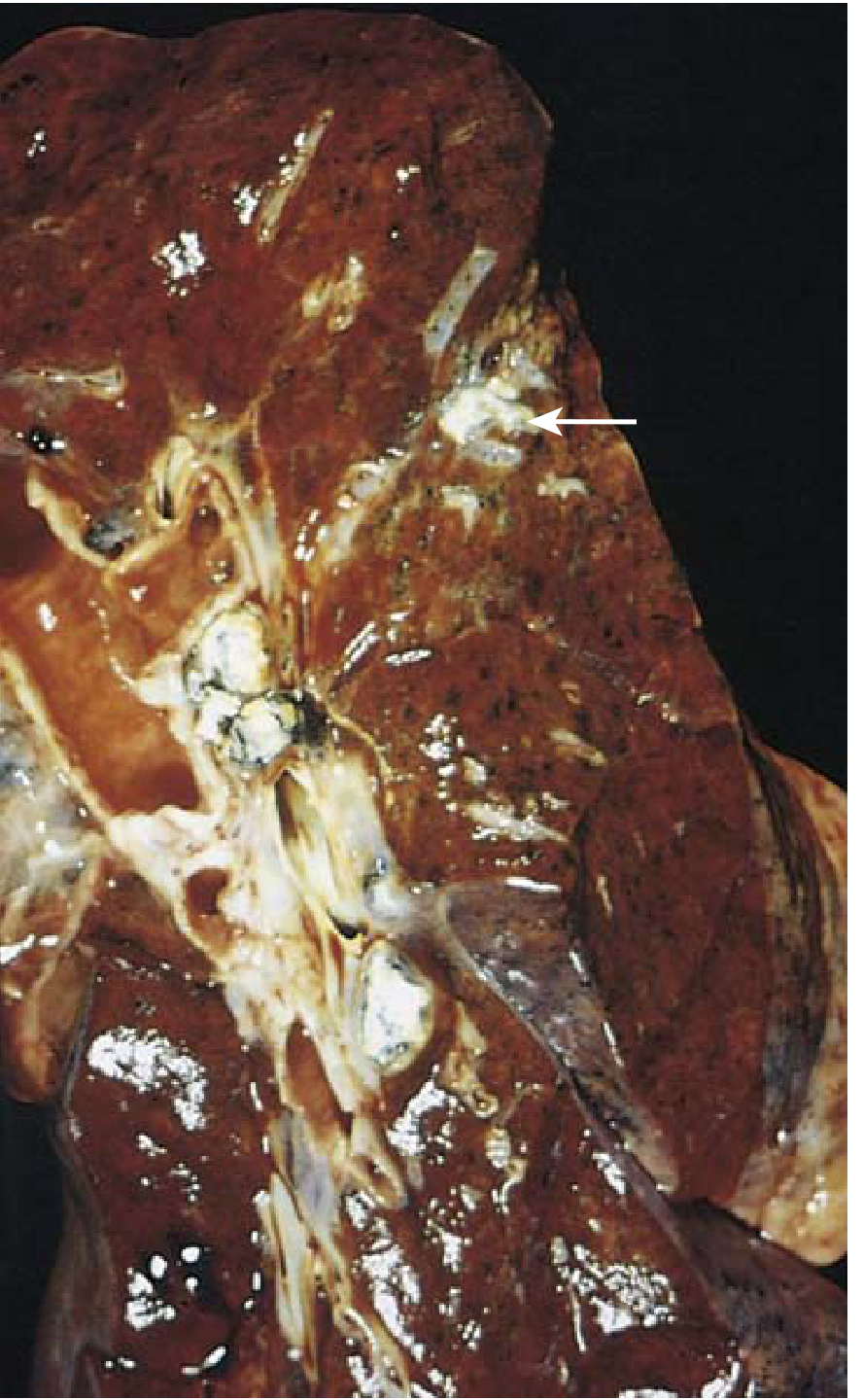
5. GROSS MORPHOLOGY
- Ghon focus: 1–1.5 cm, gray-white, firm, subpleural consolidation; center undergoes caseous necrosis (cheese-like, amorphous, acellular material)
- Lymph node: Enlarged hilar/tracheobronchial nodes with caseous necrosis
- Lymphangitic streak: Visible inflammatory track connecting focus to lymph node
6. HISTOLOGY
| Feature | Description |
|---|---|
| Tubercle | Central caseous necrosis + epithelioid macrophages + Langhans giant cells + lymphocytes + fibroblast rim |
| Giant cells | Langhans type — peripheral, horseshoe arrangement of nuclei |
| Individual tubercles | Microscopic; become macroscopic only when they coalesce |
| Immunocompromised | Granulomas absent; sheets of macrophages loaded with bacilli (no organized response) |
| Special stain | Acid-fast bacilli (Ziehl-Neelsen stain / auramine-rhodamine fluorescence) — positive in early exudative phase |
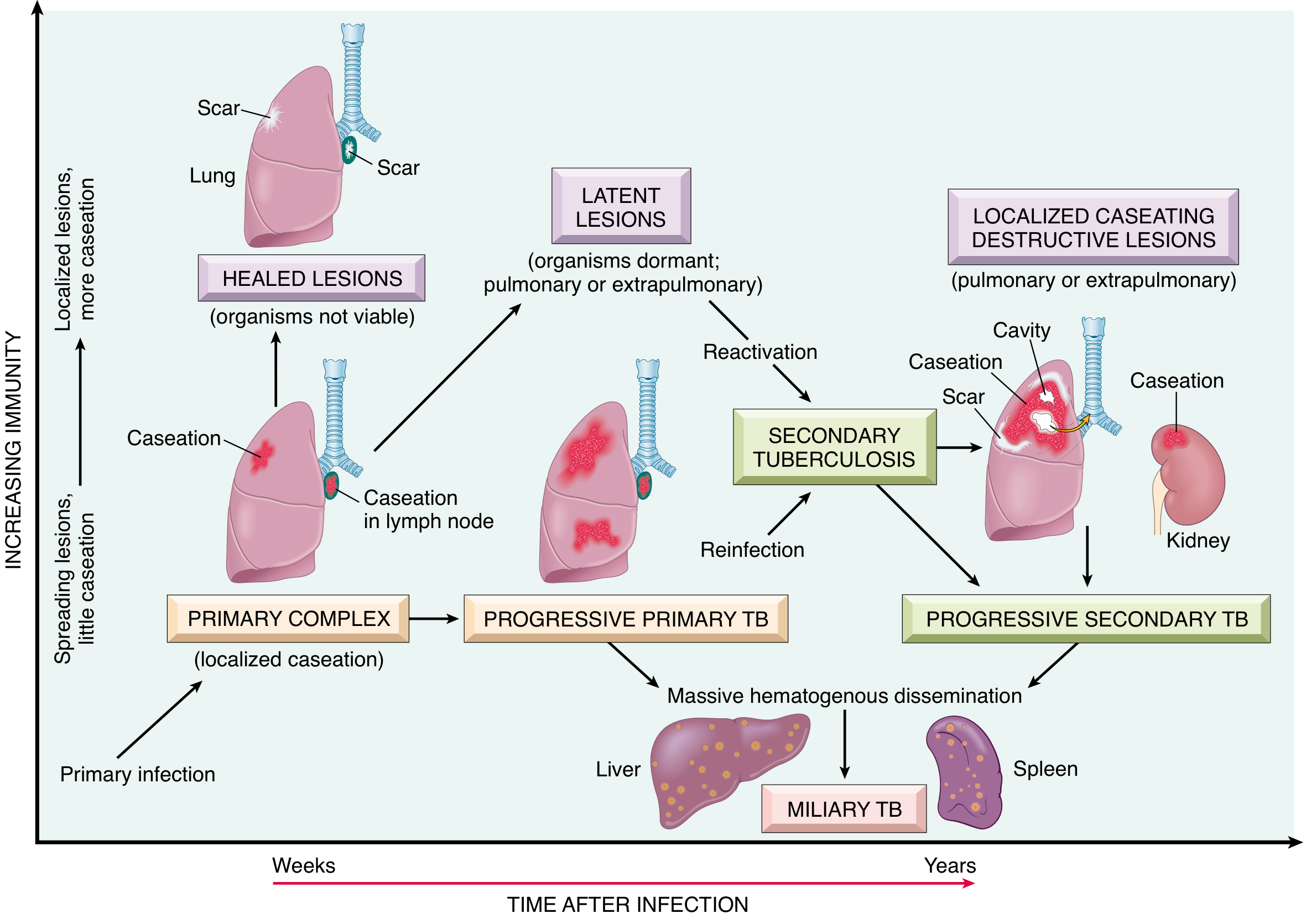
7. FATE OF GHON'S COMPLEX (Most Important for Exams)
In ~95% of cases, effective cell-mediated immunity controls the infection. The various fates are:
A. HEALING / RESOLUTION (Most Common — 95%)
- Granulomas undergo progressive fibrosis
- Followed by dystrophic calcification (calcium deposits in the caseous necrotic material)
- The calcified lesion is visible on chest X-ray as a calcified mid-lung nodule ± calcified hilar nodes
- When calcification of both the Ghon focus and hilar nodes is visible radiographically → called the Ranke complex
- Bacilli may remain viable (dormant) within the fibrocalcific lesion for decades → latent TB
- Tuberculin skin test (Mantoux) / IGRA converts to positive (indicating sensitization)
Goldman-Cecil Medicine (p. 3251): "The Ghon complex may leave a calcified Ghon lesion in the mid-lung fields or calcified hilar nodes; when found together this is referred to as the Ranke complex."
B. LATENT TUBERCULOSIS INFECTION (LTBI)
- Organisms remain dormant; immune system keeps them in check
- No symptoms, non-infectious
- Positive Mantoux / IGRA
- May reactivate decades later if immunity wanes (secondary/post-primary TB)
- Risk factors for reactivation: HIV, malnutrition, diabetes, immunosuppressive drugs (especially anti-TNF agents), renal failure, malignancy
C. PROGRESSIVE PRIMARY TUBERCULOSIS (~5%)
Occurs in:
- Children (immature immunity)
- Elderly
- HIV-positive (especially CD4 < 200 cells/µL)
- Severely malnourished
- Other immunocompromised states
Features:
- No granuloma formation (absent or poorly formed)
- Macrophages contain massive numbers of bacilli
- Resembles acute bacterial lobar pneumonia — lobe consolidation + hilar lymphadenopathy + pleural effusion
- Enlarged lymph nodes can cause bronchial compression → lobar/segmental collapse (epecially middle/upper lobe)
- May progress to miliary TB or TB meningitis
D. REACTIVATION / SECONDARY (POST-PRIMARY) TB
- Dormant bacilli in the Ghon focus or seeded organs reactivate months to years later
- Typically involves the apical segments of upper lobes (high O₂ tension)
- Features: cavitation, fibrosis, bronchogenic spread
- Regional lymph node involvement is less prominent than in primary TB (because pre-existing hypersensitivity mounts rapid response)
- Presents with: cough, hemoptysis, weight loss, night sweats, low-grade fever
E. HEMATOGENOUS DISSEMINATION → MILIARY TB
- During the first few weeks of primary infection, hematogenous spread seeds distant organs
- In 95%, this is controlled; in others (immunocompromised), leads to:
- Miliary TB: 2-mm yellow-white foci scattered throughout lungs, liver, spleen (resembling millet seeds)
- TB meningitis
- TB of bones (Pott's disease — vertebral TB), joints, kidneys, adrenals, etc.
- Can occur from progressive primary TB or secondary TB
F. ENDOGENOUS REINFECTION / LYMPH NODE COMPLICATIONS
- Caseous lymph nodes may rupture into bronchus → endobronchial TB
- Rupture into adjacent structures → sinus formation
- Epituberculosis (in children): enlarged hilar nodes compress adjacent bronchus → lobar collapse/consolidation
8. SUMMARY TABLE — FATE OF GHON'S COMPLEX
| Fate | Frequency | Mechanism | Outcome |
|---|---|---|---|
| Fibrosis + Calcification (Ranke complex) | ~95% | Effective CMI | Healed; LTBI; +ve Mantoux |
| Latent TB | Most of the 95% | Dormant viable bacilli | Reactivation possible |
| Progressive primary TB | ~5% | Failed CMI | Lobe consolidation, miliary TB, meningitis |
| Reactivation (Secondary TB) | <5% of primary | Waning immunity, reinfection | Apical cavitation |
| Miliary TB | Rare | Massive hematogenous dissemination | Multi-organ seeding |
| TB meningitis | Rare | Hematogenous/direct | Life-threatening |
9. RADIOLOGICAL FEATURES
| Finding | Description |
|---|---|
| Ghon focus | Small (<2 cm) opacity in mid-lower lung zones (often subpleural) |
| Hilar lymphadenopathy | Unilateral; involves hilum + right paratracheal nodes |
| Ghon complex (active) | Parenchymal opacity + hilar adenopathy |
| Ranke complex (healed) | Calcified parenchymal nodule + calcified hilar nodes |
| Miliary pattern | Diffuse 1–3 mm nodules throughout both lungs |
| Progressive primary | Lobar/segmental consolidation ± pleural effusion |
A transient pleural effusion may develop in primary TB (Goldman-Cecil, p. 3251).
10. IMMUNOLOGICAL SIGNIFICANCE
- The Ghon complex represents the intersection of innate and adaptive immunity in TB
- Tuberculin skin test (Mantoux) converts to positive 3–8 weeks after primary infection — marks the development of CMI
- False-negative Mantoux may occur in: active TB disease, HIV, malnutrition, sarcoidosis, viral infections, Hodgkin lymphoma, immunosuppression
- False-positive Mantoux: prior BCG vaccination, atypical mycobacteria
- IFN-γ release assays (IGRAs): more specific; not affected by BCG; preferred in BCG-vaccinated populations
11. DIFFERENCES: PRIMARY vs. SECONDARY TB
| Feature | Primary TB | Secondary (Reactivation) TB |
|---|---|---|
| Host immunity | None (first exposure) | Pre-existing (sensitized host) |
| Site | Mid-lower lung zones; subpleural | Apices of upper lobes |
| Lymph node involvement | Prominent | Less prominent |
| Cavitation | Rare | Common |
| Granuloma | Present (if immunocompetent) | Prompt, well-formed |
| Symptoms | Usually asymptomatic | Insidious: cough, hemoptysis, night sweats |
| Progression | 5% → progressive | Can lead to extensive destruction |
12. KEY EPONYMOUS TERMS (Frequently Asked)
| Term | Definition |
|---|---|
| Ghon focus | Parenchymal lung lesion alone (1–1.5 cm caseous consolidation) |
| Ghon complex | Ghon focus + draining lymph node involvement ± lymphangitic streak |
| Ranke complex | Calcified Ghon complex (calcified nodule + calcified hilar nodes) — healed primary TB |
| Simon foci | Small seeded apical foci from hematogenous spread; may reactivate → secondary TB |
| Assmann focus | Early apical infiltrate in secondary TB (also called Assmann-Redeker focus) |
| Puhl's lesion | Healed apical scarring |
KEY POINTS FOR EXAM
- Ghon complex = Ghon focus + regional lymph node caseous necrosis
- Location: lower part of upper lobe or upper part of lower lobe, subpleural
- Fate in 95%: fibrosis → calcification → Ranke complex (latent TB)
- Fate in 5%: progressive primary TB (children, immunocompromised, HIV)
- Histology: caseating granuloma with epithelioid macrophages, Langhans giant cells, lymphocytes
- Immunocompromised → no granulomas, sheets of macrophages loaded with bacilli
- Hematogenous seeding during primary infection → Simon foci (apical) → later reactivation
- Mantoux converts positive 3–8 weeks after primary infection
- Miliary TB = uncontrolled hematogenous dissemination
- Ghon complex is the sine qua non of primary TB — distinguishes it from secondary TB
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed.), pp. 352–356
- Robbins & Kumar Basic Pathology (11th ed.), pp. 474–478
- Goldman-Cecil Medicine, pp. 3250–3252
This is a shared conversation. Sign in to Orris to start your own chat.